KETONES IN DIABETES MELLITUS
MLS 419: AUBF LEC ➔ Ketonuria shows insulin deficiency and the need to
MIDTERMS WEEK 2 – LESSON 2 regulate dosage
CHEMICAL EXAMINATION OF URINE II ➔ Ketoacids accumulate in the patient’s plasma (decrease
in pH and bicarbonate levels)
KETONES ◆ Normal blood pH: 7.35- 7.45
➔ Intermediate products of fat metabolism ◆ Accumulation makes the pH acidic
◆ Acetone (2%)- 2nd to form ➔ Diuresis is initiated to remove glucose and ketones
◆ Acetoacetic acid (20%)- 1st to form ◆ not good without replenishment
◆ β-hydroxybutyrate (78%)- 3rd to form ➔ Chemical imbalance ensues which may lead to diabetic
➔ Present only when the use of available carbohydrates coma which may also lead to death
becomes compromised ➔ Ketones in the urine are valuable in the monitoring and
◆ Fats are metabolized to supply energy in lieu of management of type 1 DM
carbohydrates
◆ Normally no measurable ketones are produced CLASSIC TESTS FOR KETONE
● Renal threshold: 70 mg/dL Ferric chloride test
● Also eliminated in the lungs through breathing ➔ Gerhardt’s test, 1865
● Symptom of ketoacidosis: acetone breath ➔ Discontinued due to many false-positive reactions
(salicylates)
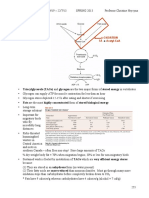
FORMATION
Nitroprusside test
➔ Legal’s test, 1883; modified by Rothera in 1908
➔ More sensitive to acetone and acetoacetate than reagent
strips
➔ Sensitivity:
◆ Acetoacetate: 1-5 mg/dL
◆ Acetone: 10-25 mg/dL
➔ Positive: Purple-colored ring formation
➔ Disadvantage: Impractical, time-consuming, laborious
REAGENT STRIP REACTIONS
➔ Normal end products of fatty acid metabolism are carbon
dioxide and water
➔ Ketogenesis
◆ happens when there is an excessive amount of fats
and occurs
◆ happens in the mitochondria of the liver
◆ limited availability of carbohydrates forces the liver
to oxidize fatty acids
➔ Most brands of reagent strips are only sensitive to ➔ Currently performed test for ketones
acetoacetate ➔ Uses sodium nitroprusside (nitroferricyanide) to
measure ketones
CLINICAL SIGNIFICANCE ➔ Acetoacetate reacts with sodium nitroprusside to
Inability to metabolize carbohydrate produce a change in color from beige to purple (large
➔ Diabetes mellitus (diabetic acidosis, insulin dosage amount)
monitoring) ◆ For Multistix
◆ Especially Type 1 ➔ The addition of glycine enables the detection of acetone
◆ Insulin- to metabolize carbohydrates ◆ For Chemstrip
Increased loss of carbohydrate ➔ Detection of ketones is qualitative (+/-) or
➔ Vomiting semi-qualitative
Inadequate intake of carbohydrate ➔ Presence of one ketone bodies is enough
➔ Starvation (several days) ➔ Sensitivity:
➔ Malabsorption/pancreatic disorders ◆ Acetoacetate: 5-10 mg/dL
◆ Acetone: 50-70 mg/dL
➔ Better test for routine urinalysis
REACTION INTERFERENCE HEMATURIA
➔ False-positive (difference: color fades rapidly on ➔ From trauma or damage of renal or genitourinary origin
standing) ◆ Renal calculi- kidney stones
◆ Phthalein dyes ◆ Glomerulonephritis- inflammation
◆ Highly-pigmented red urine (major concern) ◆ Pyelonephritis- inflammation
◆ Levodopa ◆ Tumors- swelling/inflammation
◆ Medications containing free sulfhydryl groups ◆ Exposure to chemicals and anticoagulant
(MESNA, captopril) therapy
➔ False-negative ➔ May also be due to post-strenuous exercise and
◆ Improperly preserved specimens due to rapid menstrual contamination
volatilization of ketones (remedy: test immediately
or refrigerate) HEMOGLOBINURIA
➔ Lysis of RBC produced in the urinary tract particularly in
Acetest tablets dilute, alkaline urine
◆ RBCs in microscopic exam may be seen
➔ Intravascular hemolysis
◆ No RBC in microscopic exam because hemolysis
started prior to the blood reaching the kidneys
◆ Normally: free hemoglobin forms a complex with
haptoglobin (no Hgb in urine)
◆ If all available haptoglobin is bound, free hgb is
filtered by glomerulus
◆ May be processed by renal tubular cells into
hemosiderin
◆ Hemolytic anemias, transfusion reactions,
severe burns, strenuous exercise, brown
recluse spider bites, infections (e. g. malaria)
➔ Confirmatory test for questionable ketone strip results
➔ Advantage: may be used on other specimens
➔ Contains:
◆ Nitroprusside- detect acetoacetate
◆ Glycine- detect acetone
◆ Lactose- aid in the enhancement of color reaction
(purple)
➔ 1 drop of specimen into the tablet and wait for 30
seconds
➔ Difference of concentration: intensity of the color
➔ Sensitivity:
◆ Acetoacetate: 5-10 mg/dL
◆ Acetone: 20 mg/dL (more sensitive than reagent MYOGLOBINURIA
strip) ➔ Myoglobin: heme-containing protein found in muscle
tissue
BLOOD ➔ Muscle destruction/rhabdomyolysis
➔ May be present in the urine in the form of intact red ◆ Trauma
blood cells (hematuria) or as the product of RBC ◆ Crush injuries and contact sports
destruction (hemoglobinuria) ◆ Muscle ischemia (prolonged coma, alcoholism)
➔ Most accurate method in determining the presence of ◆ Muscle infections
blood in urine ◆ Myopathy from medications
◆ 5 cells/μL of urine is clinically significant (may not ◆ Seizures/convulsions
be detected microscopically) ◆ Toxins from snake and spider bites
➔ Positive chemical test for blood is nonspecific: red blood
cells, hemoglobin, myoglobin Hemoglobinuria vs Myoglobinuria
➔ Blood reagent strip measures the presence of heme ➔ Historical test: ammonium sulfate precipitation
moiety (present in hgb and myoglobin) ➔ 2.8 g of ammonium sulfate is added to 5 mL of
centrifuged urine
CLINICAL SIGNIFICANCE ➔ Mix and let the specimen sit for 5 minutes
➔ Hematuria ➔ Filter/centrifuge urine and test supernatant with reagent
◆ intact red blood cells strip for blood
◆ cloudy or smoky red urine ➔ Hemoglobin is larger and is precipitated
➔ Hemoglobinuria ◆ Myoglobin present: supernatant remains red,
◆ Hemoglobin in urine due to RBC destruction positive for blood
◆ clear red urine ◆ Hemoglobin present: red precipitate, negative for
➔ Myoglobinuria blood
◆ tissue destruction
◆ clear red-brown urine
Parameter Hemoglobinuria Myoglobinuria
CLINICAL SIGNIFICANCE
Urine color Pink, red, brown Pink, red, brown
Blood reagent strip test Positive Positive
Serum color Pink to red Pale yellow
(hemolysis) (normal)
Serum chemistry tests:
Haptoglobin Decreased to absent Normal
Myoglobin Normal Increased
Free hemoglobin Increased Normal
Creatinine Kinase Increased, but <10 Increased, but
times upper >10 times upper
reference limit reference limit
REAGENT STRIP REACTIONS
➔ Pseudoperoxidase activity of hemoglobin (heme
moiety)
◆ Heme component + tetramethylbenzidine
chromogen + peroxide = green-blue color
REACTION INTERFERENCE
➔ False-positive
◆ Menstrual contamination
◆ Strong oxidizing reagents
◆ Vegetable peroxidase and bacterial enzymes (e.g.
E. coli peroxidase)
➔ False-negative
◆ High SG/crenated RBCs, unmixed specimens
◆ Formalin as preservative
◆ Captopril ➔ 3 fates of urobilinogen:
◆ High concentrations of nitrite and ascorbic acid ◆ Stays in the intestine & contribute to the color of
level > 25 mg/dL stool
◆ Reabsorbed into the circulation ⇒ liver ⇒ intestine
BILIRUBIN ◆ Reabsorbed into the circulation ⇒ kidney ⇒ urine
➔ Provides an early indication of liver disease urobilinogen
Jaundice Conditions Urine Fecal ➔ 2-5% of all produced urobilinogen is sent to the kidney
Classification color via blood circulation
➔ Prehepatic Jaundice
Prehepatic Hemolytic Bilirubin: Normal
(increased disorders Negative
◆ Negative urine bilirubin
heme -Transfusion Urobilinogen: ↑ ◆ ↑urobilinogen (urine & stool)
degradation) reactions ➔ Hepatic Jaundice
-Sickle cell disease ◆ Normal/↑ urine urobilinogen
-Hereditary
spherocytosis
◆ ↑urine bilirubin (positive)
-Hemolytic disease ➔ Posthepatic
of newborn ◆ ↓urobilinogen (urine & stool)
◆ ↑urine bilirubin
Ineffective
erythropoiesis
-Thalassemia REAGENT STRIP REACTIONS
-Pernicious anemia ➔ Diazo reaction
◆ Conjugated bilirubin couples with a diazonium salt
Hepatic Hepatitis Bilirubin: Normal in an acid medium to form azobilirubin (brown in
(Hepatocellular Cirrhosis Positive
disorder) Genetic disorder Urobilinogen:
color)
Normal to ↑
Posthepatic Gallstones Bilirubin: Pale,
(Obstruction) Tumors Positive chalky,
(carcinoma) Urobilinogen: ↓ “alcoholic”
Fibrosis to absent
REACTION INTERFERENCE REAGENT STRIP REACTIONS
➔ False-positive ➔ Multistix: Ehrlich’s aldehyde reaction
◆ Highly-pigmented urine (e.g. phenazopyridine)
◆ Indican (intestinal disorders)
◆ Metabolites of Lodine
➔ False-negative
◆ Exposure to light
◆ Ascorbic acid > 25 mg/dL
◆ High nitrite concentrations ➔ Chemstrip: diazo reaction using
4-methoxybenzene-diazonium-tetrafluoroborate (more
ICTOTEST TABLETS specific)
➔ Confirmatory test for bilirubin
◆ Can detect 0.05 to 0.1 mg/dL of bilirubin
◆ Reagent strip: 0.5 mg/dL lower limit of detection
➔ 10 drops of urine to an absorbent test mat
➔ Place 1 Ictotest tablet to the moistened area
➔ Add 1 drop of water to the tablet and wait 5 seconds
➔ Add 1 drop of water to the tablet; water runs off the tablet REACTION INTERFERENCE
onto the mat ➔ Multistix
➔ Observe color change after 60 seconds (positive: from ◆ False-positive: Ehrlich reactive substances
white to blue to purple color) ◆ False-negative: old specimens, formalin
preservation
UROBILINOGEN ➔ Chemstrip
➔ Normally present in urine in concentrations of 1 mg/dL ◆ False-positive: highly pigmented urine
or less ◆ False-negative: old specimens, formalin
➔ Best specimen for quantifying and monitoring: 2 hours preservation, high nitrite concentrations
after mid-day meal (2-4 PM)
◆ Alkaline tide- the parietal cells, aside from NITRITE
releasing hydrochloric acid, also releases ➔ Rapid screening test for the presence of UTI
bicarbonate and induces a temporary shift from ➔ Valuable in detecting initial bladder infection (cystitis)
acid to alkaline ◆ Many UTIs start in the bladder and progress
◆ enhanced urobilinogen excretion in alkaline urine upward; may also be asymptomatic
➔ Labile in acid urine and easily photo-oxidizes into urobilin ◆ Early detection of bacteriuria plus antibiotic
therapy can prevent pyelonephritis and other
CLINICAL SIGNIFICANCE complications
➔ Early detection of liver disease ➔ Can be used to evaluate antibiotic therapy
➔ Liver disorders, hepatitis, cirrhosis, carcinoma ➔ Can be used as periodical screen in persons at high risk
➔ Hemolytic disorders for UTI (esp. women)
Classic Ehrlich’s reaction REAGENT STRIP REACTIONS
➔ Based on the ability of certain bacteria to reduce nitrate
(normal constituent) to nitrite
➔ Sensitivity: 100,000 organisms/mL
➔ Greiss reaction
➔ Nitrite + aromatic amine (p-arsanilic acid or
sulfanilamide) = diazonium salt
➔ Diazonium slat + tetrahydrobenzoquinolin = pink azodye
➔ Old qualitative screening for urobilinogen
➔ Urobilinogen reacts with p-dimethylaminobenzaldehyde REACTION INTERFERENCE
(Ehrlich’s reagent) in an acid medium to form a pink, ➔ Bacteria that lack nitrate reductase
magenta, or red color ◆ Nitrate reductase is found in many Gram-negative
➔ 1 part Ehrlich’s reagent + 10 parts urine in a tube and bacteria that most frequently cause UTI
incubate for 5 minutes ◆ Other organisms (non-nitrate-reducing bacteria,
➔ Nonspecific test (many Ehrlich reactive substances) yeasts, T. vaginalis) that cause UTI are not
detected
➔ Insufficient contact time between bacteria and nitrate ➔ False-negative
◆ At least 4 hours ◆ High concentrations of protein, glucose, oxalic acid,
◆ First morning specimen is ideal Vitamin C, gentamicin, cephalosporins,
➔ Lack of urinary nitrate tetracyclines
◆ Nitrate is commonly found in green vegetables ◆ Inaccurate timing (note: read LE after 2 minutes)
◆ Diet is not controlled pre-testing so false-negative
results may occur SPECIFIC GRAVITY
➔ Large quantities of bacteria further reducing nitrite to ➔ Expression of solute concentration
nitrogen ➔ A fixed SG of 1.010 regardless of hydration implies
➔ Antibiotics which inhibit bacterial metabolism significant renal tubular dysfunction
➔ Vitamin C ➔ Reagent strip measures ionic or charged solutes only
➔ High specific gravity ➔ The higher the specific gravity, the more concentrated
the urine is
LEUKOCYTE ESTERASE
➔ In conjunction with nitrite to detect the presence of UTI
➔ Normally, WBCs may be present in urine in small
numbers
◆ 20/hpf indicates pathologic process
◆ High WBC count is more often found in women than
men
➔ A more standardized test than microscopic examination
of urine sediment
➔ Not designed to measure the concentration of leukocytes
➔ Can detect lysed WBCs which are not seen in
microscopic examination
➔ Sensitivity: 10-25 WBCs/microliter
◆ Note: a negative result does not rule out increased
number of WBCs
CLINICAL SIGNIFICANCE
➔ Increased WBCs are indicators of UTI or inflammation
in the urinary tract
➔ Detects the presence of esterase in granulocytes and
monocytes (also present in Trichomonas and
histiocytes)
REAGENT STRIP REACTIONS
➔ Infections caused by Trichomonas, Chlamydia, yeast,
➔ Based on the change in pKa of a polyelectrolyte in an
and inflammation of renal tissue produce leukocyturia
alkaline medium
without bacteriuria
➔ Number of ions in a solution = ionization of
➔ Assessment of LE and nitrite tests can be cost-effective
polyelectrolyte = release of hydrogen ions
measures to determine the necessity of performing urine
➔ More concentrated urine, more hydrogen ions are
culture
released, pH lowers
REAGENT STRIP REACTIONS
Direct and indirect SG measurements
➔ Ester hydrolysis and azo coupling reaction
➔ Direct specific gravity methods determine the actual
◆ Indoxylcarbonic acid ester = indoxyl + acid
or true density of urine, regardless of the solutes
indoxyl
present. All solutes are detected and measured. Not
◆ Indoxyl + diazonium salt = purple azodye
commonly used.
◆ Examples: Urinometry, harmonic oscillation
densitometry (cause false increase)
◆ Other solutes are present because of other
abnormal processes unrelated to concentrating
ability.
◆ Impractical
➔ Indirect SG methods
◆ Reagent strip and refractometry
You are incredibly brave.
REACTION INTERFERENCE
➔ False-positive
◆ Vaginal secretions contamination
◆ Strong oxidizing agents or formalin in the container
◆ Highly –pigmented urine
◆ Nitrofurantoin
You might also like
- Case Study Questions - Type I Diabetes in The AdultDocument11 pagesCase Study Questions - Type I Diabetes in The Adultoliviawooliver75% (4)
- KidneyDocument19 pagesKidneySridharNo ratings yet
- Black's Veterinary DictionaryDocument801 pagesBlack's Veterinary DictionaryGeorgiana Rosu88% (8)
- Biomedical Science-Clinical BiochemistryDocument59 pagesBiomedical Science-Clinical BiochemistryBiology BảoNo ratings yet
- Mtap - Aubf Review NotesDocument8 pagesMtap - Aubf Review NotesMoira Pauline LibroraniaNo ratings yet
- 1 Intro To HematologyDocument2 pages1 Intro To HematologyAldrin ChrisNo ratings yet
- MUCLecture 2022 52049892Document21 pagesMUCLecture 2022 52049892علي عبيد العتابيNo ratings yet
- Fluid and ElectrolytesDocument45 pagesFluid and ElectrolytesALYNo ratings yet
- PD 3.3 Alterations in GI Function Part 2Document15 pagesPD 3.3 Alterations in GI Function Part 2Kim DeeNo ratings yet
- SDLS 2008 Serum Total Protein and Albumin DeterminationDocument2 pagesSDLS 2008 Serum Total Protein and Albumin DeterminationgenieqtNo ratings yet
- CC Lab 6 TransesDocument6 pagesCC Lab 6 TransesCiara PamonagNo ratings yet
- CC Lab 6 TransesDocument6 pagesCC Lab 6 TransesCiara PamonagNo ratings yet
- Renal Function (2)Document20 pagesRenal Function (2)nekemwbnheismwbwoNo ratings yet
- Non Protein Nitrogens 1Document22 pagesNon Protein Nitrogens 1Sheine EspinoNo ratings yet
- UABF-Final CoachingDocument39 pagesUABF-Final CoachingBen SabladaNo ratings yet
- Toxocology: Abdullah Alolayan, R4Document6 pagesToxocology: Abdullah Alolayan, R4soulstakersNo ratings yet
- AUBF MidtermsDocument24 pagesAUBF MidtermsPrince SalvaNo ratings yet
- CT10382Document4 pagesCT10382Nguyễn HuynhNo ratings yet
- Clerks UA FADocument2 pagesClerks UA FALanceNo ratings yet
- Drug Lab Interaction FinalDocument133 pagesDrug Lab Interaction FinalJunnin Gay GarayNo ratings yet
- Fluid and ElectrolytesDocument6 pagesFluid and ElectrolytesMarvie TorralbaNo ratings yet
- Midterm - CC1 LabDocument11 pagesMidterm - CC1 LabHazel Joyce Gonda RoqueNo ratings yet
- NCM 112 - Renal System-Pharma-Tubes and DrainsDocument2 pagesNCM 112 - Renal System-Pharma-Tubes and DrainsCailah Sofia SelausoNo ratings yet
- Non-Protein Nitrogenous Compounds (NPN'S) : Reman A. Alingasa, RMTDocument47 pagesNon-Protein Nitrogenous Compounds (NPN'S) : Reman A. Alingasa, RMTLoulou Apollo100% (1)
- Clinical Chemistry Lecture NPNDocument5 pagesClinical Chemistry Lecture NPNmizunoNo ratings yet
- Inborn Errors of MetabolismDocument2 pagesInborn Errors of MetabolismLode DeocadesNo ratings yet
- UrinaryDocument3 pagesUrinaryIYA LABAO100% (1)
- Clinical Pathology-IDocument188 pagesClinical Pathology-IZain HadiNo ratings yet
- Diabetes: Section B2 - Group 5Document49 pagesDiabetes: Section B2 - Group 5Marvin OcampoNo ratings yet
- Renal Function Test DiscussionDocument5 pagesRenal Function Test DiscussionMard SumalpongNo ratings yet
- CM Important NotesDocument11 pagesCM Important NotesJasmine MedinaNo ratings yet
- Liver DiseasesDocument27 pagesLiver DiseasesharideepNo ratings yet
- FLG 332 Renal - 3 (2023)Document19 pagesFLG 332 Renal - 3 (2023)c6d5hggz6dNo ratings yet
- Farmakoterapi Sistem RenalDocument89 pagesFarmakoterapi Sistem RenalNhovieNhowaaNo ratings yet
- Liver Function Tests TransDocument7 pagesLiver Function Tests TransMaria Leona CentenoNo ratings yet
- Tubular Diseases: Immune-Mediated Toxic SubstancesDocument4 pagesTubular Diseases: Immune-Mediated Toxic SubstancesMoira Pauline LibroraniaNo ratings yet
- Comprehensive Clin Chem 4 1Document6 pagesComprehensive Clin Chem 4 1Binky SophiaNo ratings yet
- NPN ReviewDocument46 pagesNPN Reviewmika de guzmanNo ratings yet
- Cc1 Reading SummarizedDocument10 pagesCc1 Reading SummarizedPrecious EvangelistaNo ratings yet
- Tube Collection GuideDocument2 pagesTube Collection GuideCamella Beatrice Lujan ValleNo ratings yet
- Acute Renal Failure Case Presentation GRP 3Document60 pagesAcute Renal Failure Case Presentation GRP 3varish100% (1)
- Altered Elimination Multi System ProblemDocument9 pagesAltered Elimination Multi System ProblemCG Patron BamboNo ratings yet
- Blood AnalysisDocument10 pagesBlood AnalysisHry WkNo ratings yet
- Sindroma NefrotikDocument27 pagesSindroma NefrotikIkbal SetiawanNo ratings yet
- Tests For Glucose 1 - Benedict'S Test: Cus04 (Cupric Sulfide) + Reducing Substance HeatDocument17 pagesTests For Glucose 1 - Benedict'S Test: Cus04 (Cupric Sulfide) + Reducing Substance HeatLyka PapaNo ratings yet
- AUBF Lecture PDFDocument5 pagesAUBF Lecture PDFbravojarleneNo ratings yet
- Lab 5 Lec - Urea 2Document13 pagesLab 5 Lec - Urea 2عم رNo ratings yet
- Specimen Considerations in HematologyDocument4 pagesSpecimen Considerations in HematologydmclmllNo ratings yet
- Amino Acids and Protein: DDC Medical Laboratory Science DepartmentDocument32 pagesAmino Acids and Protein: DDC Medical Laboratory Science DepartmentMelody Jane PardilloNo ratings yet
- AubfecalysisDocument47 pagesAubfecalysisRazmine RicardoNo ratings yet
- (Trans) Aubf: Urinalysis Iii: Jean BelciñaDocument2 pages(Trans) Aubf: Urinalysis Iii: Jean BelciñaJean BelciñaNo ratings yet
- Congenital and Acquired Hemolytic Anemias: Ellis J. Neufeld MD, PHDDocument63 pagesCongenital and Acquired Hemolytic Anemias: Ellis J. Neufeld MD, PHDRabi DhakalNo ratings yet
- CKD and Uti-2Document9 pagesCKD and Uti-2Corazon Arellano RamosNo ratings yet
- Anticoagulants 1Document3 pagesAnticoagulants 1Erika VerastigueNo ratings yet
- Kidney FunctionDocument64 pagesKidney FunctionVincent LivandyNo ratings yet
- PH Protein Glucose Ketones Blood Bilirubin Urobilinogen Nitrite Leukocyte Esterase Specific GravityDocument20 pagesPH Protein Glucose Ketones Blood Bilirubin Urobilinogen Nitrite Leukocyte Esterase Specific GravityChrissa Mae Tumaliuan CatindoyNo ratings yet
- P2W3 Introduction To Increased Destruction of ErythrocytesDocument16 pagesP2W3 Introduction To Increased Destruction of ErythrocytesAyessa VillacorteNo ratings yet
- CM Review Notes 2Document22 pagesCM Review Notes 2USMAN Juhamin100% (1)
- CM Lecture NotesDocument30 pagesCM Lecture NotesJefferson SorianoNo ratings yet
- Biomedx Flow PrimerDocument5 pagesBiomedx Flow PrimerbiomedxNo ratings yet
- Biochemistry: A Short Course: Fatty Acid DegradationDocument22 pagesBiochemistry: A Short Course: Fatty Acid DegradationEli JohnsonNo ratings yet
- Dka and HonkDocument30 pagesDka and HonkignasachyntiaNo ratings yet
- Diabetic Ketoacidosis: From Wikipedia, The Free EncyclopediaDocument4 pagesDiabetic Ketoacidosis: From Wikipedia, The Free EncyclopediaTika Fajar WulandariNo ratings yet
- Blood SugarDocument4 pagesBlood SugarEleanor WilliamsNo ratings yet
- Kerygma Magazine July 2019Document52 pagesKerygma Magazine July 2019Andre Gere AdsuaraNo ratings yet
- Fight Cancer With A Ketogenic Diet (2nd Edition) - Ellen DavisDocument134 pagesFight Cancer With A Ketogenic Diet (2nd Edition) - Ellen DavisHarman Chandigarhiyaa100% (3)
- Understanding Your Urinalysis ResultsDocument2 pagesUnderstanding Your Urinalysis ResultsgoofyjeffgordonNo ratings yet
- Ketone BodiesDocument16 pagesKetone BodiesAsim Ali100% (1)
- HW - Carbohydrate Metabolism II & Lipid MetabolismDocument2 pagesHW - Carbohydrate Metabolism II & Lipid MetabolismyanNo ratings yet
- Lipid MetabolismDocument11 pagesLipid MetabolismKlint Leyesa100% (1)
- Ketone Bodies 2012Document15 pagesKetone Bodies 2012Adhya MurugesanNo ratings yet
- Chapter 25: Lipid Metabolism: Multiple ChoiceDocument7 pagesChapter 25: Lipid Metabolism: Multiple ChoiceMaxinefgc Baculo100% (1)
- Fatty Acid Oxidation: Molecular Biochemistry IIDocument39 pagesFatty Acid Oxidation: Molecular Biochemistry IIDozdi100% (1)
- Urine Sediment GuideDocument4 pagesUrine Sediment GuideSagir AlvaNo ratings yet
- 5 Day Water Fast What To Expect On The Healing JourneyDocument26 pages5 Day Water Fast What To Expect On The Healing JourneysiesmannNo ratings yet
- Lipid & AA MetabolismDocument90 pagesLipid & AA MetabolismUmi LatifahNo ratings yet
- Vet Clinical MedicineDocument222 pagesVet Clinical Medicineviswanathan periyasamy100% (1)
- Impact of Ketogenic Diet On Athletes Current InsightsDocument13 pagesImpact of Ketogenic Diet On Athletes Current InsightsMattiaNo ratings yet
- Acute DM ComplicationsDocument34 pagesAcute DM ComplicationsHillary RabinNo ratings yet
- BCH 376 (Urinalysis Lecture Notes)Document7 pagesBCH 376 (Urinalysis Lecture Notes)biddyusmc100% (1)
- Presentation by Dr. Mary Vernon at KU Medical CenterDocument77 pagesPresentation by Dr. Mary Vernon at KU Medical CenterMyIMSOnlineNo ratings yet
- DIABETES ProjectDocument26 pagesDIABETES ProjectIshq KaurNo ratings yet
- Smart Ketosis Weight Loss On Auto Pilot by Ken Roberts FREE Keto E-BookDocument13 pagesSmart Ketosis Weight Loss On Auto Pilot by Ken Roberts FREE Keto E-BookKhalilahmad KhatriNo ratings yet
- KETO DIET OVERVIEW by Guru Mann PDFDocument2 pagesKETO DIET OVERVIEW by Guru Mann PDFAbhayNo ratings yet
- Lipid and Fat MetabolismDocument25 pagesLipid and Fat MetabolismCassy WalkerNo ratings yet
- Human Anatomy and Physiology II: Biology 1414 Unit 8 Metabolism and NutritionDocument103 pagesHuman Anatomy and Physiology II: Biology 1414 Unit 8 Metabolism and Nutritionciroj25No ratings yet
- The Metabolic Map Lipids Part Two Illustration AtfDocument1 pageThe Metabolic Map Lipids Part Two Illustration AtfJoax Wayne SanchezNo ratings yet