You might also like
- How To Prevent Shin Splints 11 Steps (With Pictures) - WikiHowDocument3 pagesHow To Prevent Shin Splints 11 Steps (With Pictures) - WikiHowGeorge Alexander El-MallakhNo ratings yet
- Nutrition Month qUIZDocument29 pagesNutrition Month qUIZXeuweenNo ratings yet
- Emotional Minds PDFDocument332 pagesEmotional Minds PDFTecnologías triple BNo ratings yet
- Capnography - Self Study - GuideDocument22 pagesCapnography - Self Study - GuideSuresh KumarNo ratings yet
- Casper Cheat SheetDocument3 pagesCasper Cheat SheetMichael Moore100% (1)
- Scaffold and Fall Protection PDFDocument84 pagesScaffold and Fall Protection PDFnewnse2008100% (1)
- Mrcog Part1Document7 pagesMrcog Part1Yogeshwari Pardeshi100% (3)
- Capnometry: Dhanya VDocument49 pagesCapnometry: Dhanya VdaviddanamrajanNo ratings yet
- ACR BI-RADS® Atlas Fifth EditionDocument2 pagesACR BI-RADS® Atlas Fifth EditionRamiro Tupayachi100% (5)
- Example Method Statement For The Installation of Concrete Floor SlabsDocument8 pagesExample Method Statement For The Installation of Concrete Floor SlabsMohammad Ali ElhamNo ratings yet
- Capnography and Its ApplicationsDocument37 pagesCapnography and Its ApplicationsTraceNo ratings yet
- Bronchoscopy 1Document5 pagesBronchoscopy 1mahes2011No ratings yet
- Blue Cross v. OlivaresDocument1 pageBlue Cross v. OlivaresWV Gamiz Jr.No ratings yet
- Etco2: in Theatre, Emergency Department, Intensive Care Unit and OthersDocument42 pagesEtco2: in Theatre, Emergency Department, Intensive Care Unit and OthersyennyNo ratings yet
- End-Tidal CO2 - AAST Technical GuidelineDocument4 pagesEnd-Tidal CO2 - AAST Technical GuidelineLusy Octavia SaputriNo ratings yet
- MU Eng 12 CapnographyDocument9 pagesMU Eng 12 Capnographykareenguallpa0No ratings yet
- Continuous End Tidal Carbon Dioxide MonitoringDocument10 pagesContinuous End Tidal Carbon Dioxide MonitoringydtrgnNo ratings yet
- Critical Care in The Emergency Department: Monitoring The Critically Ill PatientDocument4 pagesCritical Care in The Emergency Department: Monitoring The Critically Ill PatientNurul Falah KalokoNo ratings yet
- Cap No GraphyDocument4 pagesCap No GraphysakkarashiiNo ratings yet
- Capnography: July 2015Document25 pagesCapnography: July 2015Juan Manuel Medina RodriguezNo ratings yet
- 203 1667 Applications20of20capnographyDocument25 pages203 1667 Applications20of20capnographyLusy Octavia SaputriNo ratings yet
- Capnography Application in Acute and Critical Care: Tom Ahrens, DNS, RN, CCRN, CS Carrie Sona, MSN, RN, CCRN, CSDocument10 pagesCapnography Application in Acute and Critical Care: Tom Ahrens, DNS, RN, CCRN, CS Carrie Sona, MSN, RN, CCRN, CSJavier Enrique Barrera PachecoNo ratings yet
- Carbon Dioxide Monitors, Exhaled GasDocument7 pagesCarbon Dioxide Monitors, Exhaled GasLee ThoongNo ratings yet
- Capnography - A ValuableTool For Airway Management. 2008Document17 pagesCapnography - A ValuableTool For Airway Management. 2008N. TrejosNo ratings yet
- CO Solutions: Quick Reference GuideDocument20 pagesCO Solutions: Quick Reference GuideEng - Mohamed Makram100% (1)
- Respiratory SarachoDocument13 pagesRespiratory SarachoDianne Erika MeguinesNo ratings yet
- Practical Use of Capnography in Exotic Animal Anesthesia: Michael Stanford, BVSC, MrcvsDocument4 pagesPractical Use of Capnography in Exotic Animal Anesthesia: Michael Stanford, BVSC, MrcvstobymusicltdNo ratings yet
- (2014) Capnography During Cardiopulmonary Resuscitation - Current Evidence and Future DirectionsDocument10 pages(2014) Capnography During Cardiopulmonary Resuscitation - Current Evidence and Future DirectionsDominik Chirito PastorNo ratings yet
- Capnography Outside The OTDocument10 pagesCapnography Outside The OTqueenartemisNo ratings yet
- Review2 PDFDocument7 pagesReview2 PDFFadly TaralaluNo ratings yet
- Capnography in DogsDocument14 pagesCapnography in DogswalczakcNo ratings yet
- Time To Throw AwayDocument10 pagesTime To Throw AwayPuteri Indah Achmad HasyimNo ratings yet
- March 2015Document98 pagesMarch 2015Steph MederoNo ratings yet
- Biomedical Signal Processing and Control: Surita Sarkar, Parthasarathi Bhattacharyya, Madhuchhanda Mitra, Saurabh PalDocument10 pagesBiomedical Signal Processing and Control: Surita Sarkar, Parthasarathi Bhattacharyya, Madhuchhanda Mitra, Saurabh PalAlaina MalsiNo ratings yet
- Review ArticleDocument11 pagesReview Articlemuhamad abdul kodirNo ratings yet
- The Accuracy of Non-Invasive Nasal Capnography in Morbidly Obese Patients After Bariatric Surgery A Y, C Z, F R, V C, G S R NDocument12 pagesThe Accuracy of Non-Invasive Nasal Capnography in Morbidly Obese Patients After Bariatric Surgery A Y, C Z, F R, V C, G S R NFer45No ratings yet
- JURDING 1 - Usefulness of Lung Ultrasound For Early Detection of Hospital-Acquired Pneumonia in Cardiac Critically Ill Patients On Venoarterial Extracorporeal Membrane OxygenationDocument10 pagesJURDING 1 - Usefulness of Lung Ultrasound For Early Detection of Hospital-Acquired Pneumonia in Cardiac Critically Ill Patients On Venoarterial Extracorporeal Membrane OxygenationLivia Meidy UbayidNo ratings yet
- Brochardrespmonitconsof 16 CC 2012Document15 pagesBrochardrespmonitconsof 16 CC 2012Leandro VillamilNo ratings yet
- Developing An Algorithm For Pulse Oximetry DerivedDocument8 pagesDeveloping An Algorithm For Pulse Oximetry DerivedSabri KhalidNo ratings yet
- 10 1378@chest 09-2690Document9 pages10 1378@chest 09-2690Alvaro Andres Flores JimenezNo ratings yet
- Capnoin EDDocument4 pagesCapnoin EDMirela CiobanescuNo ratings yet
- Dr. Radhika Dhanpal: Department of Anesthesiology and Critical Care, St. John's Medical College Hospital BangaloreDocument67 pagesDr. Radhika Dhanpal: Department of Anesthesiology and Critical Care, St. John's Medical College Hospital Bangalorethalida24No ratings yet
- Volumetric CapnographyDocument7 pagesVolumetric CapnographyAlejandra Castillo MantillaNo ratings yet
- CAPNOGRAPHYDocument10 pagesCAPNOGRAPHYJessica GuzmanNo ratings yet
- An Introduction To Surgical Icu.: Mohamed Emad Abdel-Ghaffar. Professor of Anesthesiology, Fom, King Faisal UniversityDocument38 pagesAn Introduction To Surgical Icu.: Mohamed Emad Abdel-Ghaffar. Professor of Anesthesiology, Fom, King Faisal UniversityHassan.shehriNo ratings yet
- An Introduction To Surgical Icu.: by DR Farrukh SaeedDocument33 pagesAn Introduction To Surgical Icu.: by DR Farrukh SaeedTARIQNo ratings yet
- Respiratory Monitoring in The IcuDocument14 pagesRespiratory Monitoring in The IcuLorena DobrescuNo ratings yet
- Cytologic and Hematologic Tests Arterial Blood Gases: Medical Background: Chronic Restrictive Pulmonary DiseaseDocument7 pagesCytologic and Hematologic Tests Arterial Blood Gases: Medical Background: Chronic Restrictive Pulmonary Diseasejoanna gurtizaNo ratings yet
- Apnea Test PDFDocument10 pagesApnea Test PDFaeagesNo ratings yet
- Riding The WavesDocument76 pagesRiding The WavesMedic03431No ratings yet
- Control of Respiratory Drive by Extracorporeal CO Removal in Acute Exacerbation of COPD Breathing On Non-Invasive NAVADocument9 pagesControl of Respiratory Drive by Extracorporeal CO Removal in Acute Exacerbation of COPD Breathing On Non-Invasive NAVAMileth GonzalezNo ratings yet
- Noninvasive Tidal Volume Measurements, Using A Time-of-Flight Camera, Under High-Flow Nasal Cannula-A Physiological Evaluation, in Healthy VolunteersDocument10 pagesNoninvasive Tidal Volume Measurements, Using A Time-of-Flight Camera, Under High-Flow Nasal Cannula-A Physiological Evaluation, in Healthy VolunteersgiadungdanamallNo ratings yet
- 7 - Capnography ProcedureDocument2 pages7 - Capnography ProcedurejasminemuammilNo ratings yet
- BronchosDocument5 pagesBronchosNeicoNo ratings yet
- A 1-D Deformable Convolutional Neural Network For The Quantitative Analysis of Capnographic SensorDocument7 pagesA 1-D Deformable Convolutional Neural Network For The Quantitative Analysis of Capnographic SensorHari PrasadNo ratings yet
- J Vet Emergen Crit Care - 2012 - Brainard - RECOVER Evidence and Knowledge Gap Analysis On Veterinary CPR Part 5Document20 pagesJ Vet Emergen Crit Care - 2012 - Brainard - RECOVER Evidence and Knowledge Gap Analysis On Veterinary CPR Part 5sebastian Jimenez PNo ratings yet
- ETCO2 ReadingDocument19 pagesETCO2 ReadingTuan TrinhNo ratings yet
- 3-Monitoreo Del PX en EmergenciasDocument6 pages3-Monitoreo Del PX en EmergenciasHoracio A. AguilarNo ratings yet
- CDI Background: Respiratory Failure: Definitions For Acute Respiratory Failure and ARDS Endorsed by Sutter SystemDocument5 pagesCDI Background: Respiratory Failure: Definitions For Acute Respiratory Failure and ARDS Endorsed by Sutter SystemNafisah Putri WyangsariNo ratings yet
- Cap No GraphyDocument37 pagesCap No GraphyLeypotNo ratings yet
- Cardiac Output Estimation Using Ballistocardiography: A Feasibility Study in Healthy SubjectsDocument9 pagesCardiac Output Estimation Using Ballistocardiography: A Feasibility Study in Healthy SubjectsshucksmaamNo ratings yet
- Endobronchial Nerve Ablation For Chronic Obstructive Pulmonary DiseaseDocument5 pagesEndobronchial Nerve Ablation For Chronic Obstructive Pulmonary DiseaseJEFFERSON MUÑOZNo ratings yet
- Viren PC BasedDocument21 pagesViren PC BasedAman SainiNo ratings yet
- E000939 FullDocument7 pagesE000939 Fullvenkat_bhagavatiNo ratings yet
- Journal Homepage: - : IntroductionDocument9 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Poximeter 2.0Document34 pagesPoximeter 2.0Srinivasa Reddy Devireddy100% (1)
- 2019 QPEM PPT Presentation Final Capnography 2Document10 pages2019 QPEM PPT Presentation Final Capnography 2oliviamonicadNo ratings yet
- Respiratory Care j2Document15 pagesRespiratory Care j2juan carlosNo ratings yet
- Program Latihan Minggu 44-53Document27 pagesProgram Latihan Minggu 44-53JohannaMaizunNo ratings yet
- Medicine: Effects of Motivational Methods On Oral Hygiene of Orthodontic PatientsDocument8 pagesMedicine: Effects of Motivational Methods On Oral Hygiene of Orthodontic PatientsNurul pattyNo ratings yet
- Prevention Science RCTDocument10 pagesPrevention Science RCTYunquanNo ratings yet
- Hydrotherapy Stroke ChinaDocument7 pagesHydrotherapy Stroke China黃姵儒No ratings yet
- Mild Moderate Severe Subset: Respiratory Arrest ImminentDocument7 pagesMild Moderate Severe Subset: Respiratory Arrest ImminentPia VSNo ratings yet
- Medical Students: What Educational Resources Are They Using?Document8 pagesMedical Students: What Educational Resources Are They Using?Farhad JabarNo ratings yet
- Essential Intrapartum Care: From Evidence To PracticeDocument78 pagesEssential Intrapartum Care: From Evidence To PracticeGeline Joy D. SamillanoNo ratings yet
- Enviormnetal Psychology Abhay Sunny George A1506919059Document9 pagesEnviormnetal Psychology Abhay Sunny George A1506919059Editor OfficeNo ratings yet
- GMC Benefit Manual - 22Document28 pagesGMC Benefit Manual - 22SwaNo ratings yet
- Leadership 5.1 Leadership and CommitmentDocument1 pageLeadership 5.1 Leadership and CommitmentAnabela GibraltarNo ratings yet
- Civic Education Year 6Document11 pagesCivic Education Year 6mohamad hanafi SalamonNo ratings yet
- Level of Service Quality of Fast Food Restaurants As Assessed by The Customers in Daet, Camarines NorteDocument24 pagesLevel of Service Quality of Fast Food Restaurants As Assessed by The Customers in Daet, Camarines NorteAtlas MayoNo ratings yet
- Takeover Day ToolkitDocument40 pagesTakeover Day ToolkitТатьяна МогорянNo ratings yet
- Thiyagarajan Subramanian: D.M.E., DIS.,IOSH.Document5 pagesThiyagarajan Subramanian: D.M.E., DIS.,IOSH.Achyut KrishnaNo ratings yet
- CBSE Class 7 Science - Nutrition in AnimalsDocument5 pagesCBSE Class 7 Science - Nutrition in Animalssifat mongaNo ratings yet
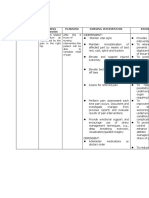
- NCP (Acute Pain)Document1 pageNCP (Acute Pain)Joan QuebalayanNo ratings yet
- Victim and VictimizationDocument21 pagesVictim and VictimizationLeo BaccayNo ratings yet
- Clinical Dermatology: Postgraduate Certificate inDocument4 pagesClinical Dermatology: Postgraduate Certificate inAlveera ZafarNo ratings yet
- Merritt Morning Market 3771 - Dec 12Document2 pagesMerritt Morning Market 3771 - Dec 12Kim LeclairNo ratings yet
- Ways To Manage StressDocument12 pagesWays To Manage StressJia YinnNo ratings yet
- 23ID009626 SummaryPDFEn PDFDocument6 pages23ID009626 SummaryPDFEn PDFZakiah SyahidahNo ratings yet