1
Test Bank for Organizational Behaviou Understanding and Managing
Life at Work Canadian Edition Canadian 9th Edition Johns Saks
0133347508 9780133347500
Full link download:
https://testbankpack.com/p/test-bank-for-organizational-behaviou-
understanding-and-managing-life-at-work-canadian-edition-canadian-9th-
edition-johns-saks-0133347508-9780133347500/
Test Bank for Johns/Saks, Organizational Behaviour, Ninth Edition
Chapter 2
1) An individual's personality encompasses
a. a relatively stable set of psychological characteristics.
b. a constantly shifting set of personal characteristics.
c. all aspects of the individual's consciousness.
d. behaviours which are mostly learned through childhood experience.
e. all aspects of the individual's physical and emotional response to their environment.
Answer: a
Diff: 2
Type: MC
Page Reference: 44
Skill: Recall
Objective: 2.1 Define "personality" and discuss its general role in influencing
organizational behaviour.
2) Personality will have the most impact in which situation?
a. Weak situations of loosely defined roles with few rules
b. Strong situations with well defined roles, rules, and contingencies
c. Both weak and strong situations
d. Situations of medium strength
e. Weak situations with well defined roles, rules, and contingencies
Answer: a
Copyright © 2014 Pearson Canada Inc.
2
Diff: 3
Type: MC
Page Reference: 45
Skill: Recall
Objective: 2.1 Define "personality" and discuss its general role in influencing
organizational behaviour.
3) Personality is most commonly thought to consist of general dimensions.
a. four
b. five
c. three
d. seven
e. six
Answer: b
Diff: 1
Type: MC
Page Reference: 46
Skill: Recall
Objective: 2.3 Discuss the Five-Factor Model of personality.
4) The personality dimension of extraversion is defined as
a. the extent to which a person is outgoing and enjoys social situations.
b. the degree to which a person has appropriate emotional control.
c. the extent to which a person is friendly and approachable.
d. the degree to which a person thinks flexibly and is receptive to new ideas.
e. the degree to which a person is responsible and achievement oriented.
Answer: a
Diff: 1
Type: MC
Page Reference: 46
Skill: Recall
Objective: 2.3 Discuss the Five-Factor Model of personality.
5) The personality dimension of emotional stability is defined as
Copyright © 2014 Pearson Canada Inc.
3
a. the extent to which a person is outgoing and enjoys social situations.
b. the degree to which a person has appropriate emotional control.
c. the extent to which a person is friendly and approachable.
d. the degree to which a person thinks flexibly and is receptive to new ideas.
e. the degree to which a person is responsible and achievement oriented.
Answer: b
Diff: 1
Type: MC
Page Reference: 46
Skill: Recall
Objective: 2.3 Discuss the Five-Factor Model of personality.
6) Extraversion is especially important for jobs that require
a. low interpersonal interaction and independence.
b. in-depth research and analysis with great independence.
c. extensive education and credibility, e.g., Ph.D.
d. a lot of interpersonal interaction such as sales and management.
e. being a solo practitioner.
Answer: d
Diff: 2
Type: MC
Page Reference: 46
Skill: Recall
Objective: 2.3 Discuss the Five-Factor Model of personality.
7) The personality dimension of agreeableness is defined as
a. the extent to which a person is outgoing and enjoys social situations.
b. the degree to which a person has appropriate emotional control.
c. the extent to which a person is friendly and approachable.
d. the degree to which a person thinks flexibly and is receptive to new ideas.
e. the degree to which a person is responsible and achievement oriented.
Answer: c
Diff: 1
Copyright © 2014 Pearson Canada Inc.
4
Type: MC
Page Reference: 47
Skill: Recall
Objective: 2.3 Discuss the Five-Factor Model of personality.
8) Emotional stability helps support positive work performance because
a. the person is neurotic about their responsibilities and is fanatically detail oriented.
b. the person is more calm and has highly effective interactions with co-workers and
customers.
c. the person is obsessive with customer service quality.
d. the person expresses great detachment and apathy.
e. the person sticks to their established patterns and ignores updated information.
Answer: b
Diff: 2
Type: MC
Page Reference: 46
Skill: Recall
Objective: 2.3 Discuss the Five-Factor Model of personality.
9) The personality dimension of conscientiousness is defined as
a. the extent to which a person is outgoing and enjoys social situations.
b. the degree to which a person has appropriate emotional control.
c. the extent to which a person is friendly and approachable.
d. the degree to which a person thinks flexibly and is receptive to new ideas.
e. the degree to which a person is responsible and achievement oriented.
Answer: e
Diff: 1
Type: MC
Page Reference: 47
Skill: Recall
Objective: 2.3 Discuss the Five-Factor Model of personality.
10) The personality dimension of openness to experience is defined as
a. the extent to which a person is outgoing and enjoys social situations.
Copyright © 2014 Pearson Canada Inc.
5
b. the degree to which a person has appropriate emotional control.
c. the extent to which a person is friendly and approachable.
d. the degree to which a person thinks flexibly and is receptive to new ideas.
e. the degree to which a person is responsible and achievement oriented.
Answer: d
Diff: 1
Type: MC
Page Reference: 47
Skill: Recall
Objective: 2.3 Discuss the Five-Factor Model of personality.
11) The personality dimension which helps foster cooperation and nurturing of others and
teamwork is
a. emotional stability.
b. conscientiousness.
c. general self-efficacy.
d. self-monitoring.
e. agreeableness.
Answer: e
Diff: 1
Type: MC
Page Reference: 47
Skill: Recall
Objective: 2.3 Discuss the Five-Factor Model of personality.
12) Recent studies suggest that extraversion is related to absenteeism in a positive
direction. This means that
a. extraverts tend to be absent less often than introverts.
b. the more extraverted a person is, the less absent they are.
c. extraverts tend to be absent more often than introverts.
d. the more introverted a person is, the more absent they are.
e. people become more extraverted through higher absenteeism.
Answer: c
Copyright © 2014 Pearson Canada Inc.
6
Diff: 3
Type: MC
Page Reference: 47
Skill: Recall
Objective: 2.3 Discuss the Five-Factor Model of personality.
13) Edward has recently been told that he is very effective at networking with potential
customers. However, his follow-up after initial contact is sloppy and his files are not up
to date. In order to be more effective on the job he needs to keep working on the
part of his personality.
a. emotional stability
b. openness to experience
c. neuroticism
d. conscientiousness
e. independence
Answer: d
Diff: 2
Type: MC
Page Reference: 47
Skill: Applied
Objective: 2.3 Discuss the Five-Factor Model of personality.
14) Janet has shown her boss how effective she is on the job because she is naturally
curious about what is happening with her company, has broad interests, and has a vibrant
imagination. She is demonstrating great
a. willingness to get along with everyone.
b. openness to experience.
c. focus on getting promoted and is highly ambitious.
d. emotional stability.
e. reluctance to work long hours.
Answer: b
Diff: 2
Type: MC
Page Reference: 47
Skill: Applied
Copyright © 2014 Pearson Canada Inc.
7
Objective: 2.3 Discuss the Five-Factor Model of personality.
15) Gary Reynolds is the CEO of Reynolds Software Limited. He attributes his success to
careful planning, hard work, and a good business education. In terms of locus of control,
Gary is most likely a(n)
a. external.
b. extravert.
c. introvert.
d. internal.
e. high self-monitor.
Answer: d
Diff: 2
Type: MC
Page Reference: 48
Skill: Applied
Objective: 2.4 Describe and discuss the consequences of "locus of control," "self-
monitoring," and "self-esteem."
16) A person who is a high self-monitor will
a. observe the situation when determining how to behave.
b. ignore the situation when determining how to behave.
c. be rather rigid in his or her leadership style.
d. be prone to uncontrollable emotional outbursts.
e. have difficulty regulating their behaviour in social situations.
Answer: a
Diff: 2
Type: MC
Page Reference: 49
Skill: Applied
Objective: 2.4 Describe and discuss the consequences of "locus of control," "self-
monitoring," and "self-esteem."
17) A person with low self-esteem will likely
a. react well to ambiguous stressful situations.
Copyright © 2014 Pearson Canada Inc.
8
b. be able to deal with negative feedback.
c. be less susceptible to external and social influences.
d. respond well to mentoring.
e. be less pliable than someone with high self-esteem.
Answer: d
Diff: 2
Type: MC
Page Reference: 50
Skill: Applied
Objective: 2.4 Describe and discuss the consequences of "locus of control," "self-
monitoring," and "self-esteem."
18) Learning is
a. a relatively temporary change in behaviour potential due to experience.
b. a relatively permanent change in behaviour potential due to experience.
c. not directly related to behaviour or experience.
d. related to behaviour more than experience.
e. concerned with both permanent and temporary changes.
Answer: b
Diff: 2
Type: MC
Page Reference: 53
Skill: Recall
Objective: 2.6 Define "learning" and what is learned in organizations.
19) Which of the following is not one of the four primary categories of learning content
in organizations?
a. Practical skills
b. Intrapersonal skills
c. Interpersonal skills
d. Cultural awareness
e. Financial management
Answer: e
Copyright © 2014 Pearson Canada Inc.
9
Diff: 1
Type: MC
Page Reference: 53
Skill: Recall
Objective: 2.6 Define "learning" and what is learned in organizations.
20) Social cognitive theory is most strongly associated with which of the following
concepts?
a. Punishment
b. Delayed reinforcement
c. Partial reinforcement
d. Modelling
e. Extinction
Answer: d
Diff: 2
Type: MC
Page Reference: 61
Skill: Recall
Objective: 2.10 Explain social cognitive theory and discuss "observational learning,"
"self-efficacy beliefs," and "self-regulation."
21) To obtain the best compromise between the speed of acquisition of a desired response
and resistance to its extinction, which reinforcement strategy should be used in training?
(In other words, how do we get the fastest learning combined with the strongest
resistance to extinction?)
a. Continuous reinforcement
b. Begin with self-management and then go to modeling.
c. Begin with delayed and partial reinforcement and gradually go to immediate and
continuous reinforcement.
d. Begin with immediate and continuous reinforcement and gradually go to delayed and
partial reinforcement.
e. Begin with negative reinforcement and gradually change to continuous positive
reinforcement.
Answer: d
Diff: 3
Copyright © 2014 Pearson Canada Inc.
10
Type: MC
Page Reference: 57
Skill: Applied
Objective: 2.8 Explain when to use immediate versus delayed reinforcement and when to
use continuous versus partial reinforcement.
22) Ron is a sensitive person, and he works very hard so that his boss doesn't criticize
him. Criticism is a(n) of Ron's work.
a. positive reinforcer
b. extinguisher
c. negative reinforcer
d. punisher
e. continuous reinforcer
Answer: c
Diff: 2
Type: MC
Page Reference: 55
Skill: Applied
Objective: 2.7 Explain "operant learning theory" and differentiate between positive and
negative reinforcements.
23) A company converted its machine operators from piece rate pay to hourly pay and
found that accidents involving the machines were reduced to almost zero from a
previously high level. What can we conclude?
a. Safe working practices were positively reinforced.
b. Unsafe working practices were punished.
c. Safe working practices were negatively reinforced.
d. Unsafe working practices were extinguished.
e. Hourly pay resulted in bigger paycheques for the machine operators.
Answer: d
Diff: 3
Type: MC
Page Reference: 58
Skill: Applied
Copyright © 2014 Pearson Canada Inc.
11
Objective: 2.9 Distinguish between "extinction" and "punishment" and explain how to
use punishment effectively.
24) A supervisor complimented each of his workers as he or she arrived promptly to
work every morning. Due to time constraints, the supervisor had to stop this practice,
resulting in a much higher rate of tardiness among his workers. Which of the following
statements best explains this situation in operant terms?
a. The supervisor was inadvertently punishing his workers by not complimenting them,
so the workers didn't arrive on time any more.
b. The supervisor's negative reinforcement strategy was stopped, thus extinguishing the
behaviour of arriving promptly.
c. The supervisor was using a continuous, immediate reinforcement strategy, and
behaviour learned under such conditions is easily extinguishable.
d. The supervisor was using a partial reinforcement strategy, and behaviour learned under
such conditions is easily extinguishable.
e. The supervisor was using a delayed reinforcement strategy, and behaviour learned
under such conditions is easily extinguishable.
Answer: c
Diff: 3
Type: MC
Page Reference: 57
Skill: Applied
Objective: 2.8 Explain when to use immediate versus delayed reinforcement and when to
use continuous versus partial reinforcement.
25) Which of the following statements concerning extinction is false?
a. Extinction works best when coupled with the reinforcement of a desired substitute
behaviour.
b. Behaviours learned under delayed or partial reinforcement schedules are more difficult
to extinguish than those learned under continuous, immediate reinforcement.
c. Extinction can be successful in reducing an unwanted behaviour by removing the
reinforcer of that behaviour.
d. Using the application of an unpleasant stimulus after an unwanted behaviour,
extinction can reduce the probability of that behaviour occurring again.
e. Behaviours which are eliminated through extinction may reappear if they become
positively reinforced again.
Answer: d
Copyright © 2014 Pearson Canada Inc.
12
Diff: 3
Type: MC
Page Reference: 58
Skill: Applied
Objective: 2.9 Distinguish between "extinction" and "punishment" and explain how to
use punishment effectively.
26) Which of the following represents the least effective reinforcement strategy?
a. Delayed reinforcement
b. Immediate reinforcement
c. Continuous reinforcement
d. Negative reinforcement
e. This question cannot be answered accurately as stated.
Answer: e
Diff: 2
Type: MC
Page Reference: 57
Skill: Applied
Objective: 2.8 Explain when to use immediate versus delayed reinforcement and when to
use continuous versus partial reinforcement.
27) In learning terms, a model is a person who
a. imitates the behaviour of others.
b. administers a high degree of positive reinforcement.
c. has his or her behaviour imitated.
d. engages in self-management.
e. seeks a mentor.
Answer: c
Diff: 1
Type: MC
Page Reference: 61
Skill: Recall
Objective: 2.10 Explain social cognitive theory and discuss "observational learning,"
"self-efficacy beliefs," and "self-regulation."
Copyright © 2014 Pearson Canada Inc.
13
28) If a behaviour is increasing in probability, we can be certain that it is not being
a. extinguished.
b. positively reinforced.
c. learned.
d. negatively reinforced.
e. modelled.
Answer: a
Diff: 1
Type: MC
Page Reference: 58
Skill: Recall
Objective: 2.7 Explain "operant learning theory" and differentiate between positive and
negative reinforcements.
29) When we say that organizations sometimes confuse rewards with reinforcers, we
mean that
a. rewards cannot serve as reinforcers.
b. people differ as to which rewards are reinforcing.
c. the rewards are not made contingent on a desired behaviour.
d. the reinforcers are not backed up with attractive rewards.
e. only monetary rewards work as effective reinforcers.
Answer: c
Diff: 2
Type: MC
Page Reference: 55
Skill: Recall
Objective: 2.7 Explain "operant learning theory" and differentiate between positive and
negative reinforcements.
30) A positive reinforcer is
a. pay.
b. interesting work.
c. a holiday.
Copyright © 2014 Pearson Canada Inc.
14
d. a company car.
e. There is insufficient information to accurately answer this question.
Answer: e
Diff: 1
Type: MC
Page Reference: 54
Skill: Recall
Objective: 2.7 Explain "operant learning theory" and differentiate between positive and
negative reinforcements.
31) The concepts of observational learning and self-regulation both assume
a. that cognitive learning cannot occur.
b. that extinction is superior to punishment.
c. that people can reinforce themselves.
d. that learning can occur without reinforcement.
e. that all workers prefer the same reinforcers.
Answer: c
Diff: 2
Type: MC
Page Reference: 61
Skill: Recall
Objective: 2.10 Explain social cognitive theory and discuss "observational learning,"
"self-efficacy beliefs," and "self-regulation."
32) decreases the probability of a behaviour by the application of a negative
stimulus after that behaviour occurs.
a. Punishment
b. Extinction
c. Negative reinforcement
d. Positive reinforcement
e. Modelling
Answer: a
Diff: 1
Copyright © 2014 Pearson Canada Inc.
15
Type: MC
Page Reference: 58
Skill: Recall
Objective: 2.9 Distinguish between "extinction" and "punishment" and explain how to
use punishment effectively.
33) increases the probability of a behaviour by the removal of a negative
stimulus after that behaviour occurs.
a. Punishment
b. Extinction
c. Negative reinforcement
d. Positive reinforcement
e. Modelling
Answer: c
Diff: 1
Type: MC
Page Reference: 55
Skill: Recall
Objective: 2.7 Explain "operant learning theory" and differentiate between positive and
negative reinforcements.
34) To reduce the probability of some unwanted behaviour we can use
a. positive reinforcement.
b. extinction.
c. negative reinforcement.
d. continuous reinforcement.
e. immediate reinforcement.
Answer: b
Diff: 2
Type: MC
Page Reference: 58
Skill: Recall
Objective: 2.9 Distinguish between "extinction" and "punishment" and explain how to
use punishment effectively.
Copyright © 2014 Pearson Canada Inc.
Another random document with
no related content on Scribd:
census of 10,000 individuals. Six districts were chosen in different
sections of the city, representing six different economic and social
groups. Great care was exercised in selecting the districts, so that the
population in each might be as homogeneous as possible regarding
economic and sanitary status, as well as race, and living conditions in
general.
We have sought to clarify and to abbreviate our description of the
characteristics of the various districts by incorporating a map,
together with photographs of typical streets in each district. One who
compares these streets as they are seen in the photographs would
scarcely find it necessary to enter the buildings in order to discover
the living conditions of the occupants (Chart XIII).
CHART XIII.
Map of greater Boston showing the
distribution of the districts covered by
the author’s house census.
District I includes an Italian population of 2,000 individuals, one-
half of which live in the most congested portion of the city (see
photograph) known as the North End, while the other half, living in
East Boston, are slightly less crowded.
District II, in South Boston, consists of 2,000 individuals almost
entirely of Irish race stock.
Fig. 1.—District 1. Italian tenements. Very congested and very
poor.
District III, like District I, consists of three groups living in very
similar environment to the two groups of the first district, but
composed chiefly of Jewish race stock of various nationalities. The
photograph for this district represents the area in the “West Side”
near the Charles River Basin. The area in the “South End” is of
similar type, while the area in East Boston is housed similarly to the
Italian district in East Boston. The dwellings in both of these latter
districts correspond to those shown in the second photograph of
District II.
While the first three districts comprise tenement areas, some poor
and the remainder very poor, Districts IV and V represent the middle
class, and consist nearly entirely of “Duplex” and “Three-Decker”
buildings. The first of these comprises 1,000 individuals of mixed
race and nationality, the type broadly spoken of as American. The
second consists of a Jewish population of 1,600.
Fig. 2.—District 2. Irish tenements. Congested and poor.
Fig. 3.—Another street in the Irish tenement district.
Fig. 4.—District 3. Jewish tenements. Very congested. Very poor.
Fig. 5.—District 4. Middle class. Mixed American population.
Fig. 6.—District 5. Middle class. Jewish population. Moderately
well-to-do.
Fig. 7.—District 6. Well-to-do population. Mixed American.
In District VI are included 1,400 individuals belonging to the well-
to-do and moderately wealthy families of Brookline.
The six districts may be considered as representative of the various
strata of society, so that we are enabled to study the influenza and its
mode of action under varying environment. We have selected areas
in the city consisting of households or homes rather than boarding
houses and rooming populations. After a few attempts in the latter
group we became convinced that the information obtained in
rooming houses was utterly valueless. In the Jewish districts we were
able, through the kind co-operation of the Federated Jewish
Charities, to use trained Jewish Social Service Workers, each of
whom had previously worked in the district assigned to her, thereby
possessing the confidence of the inhabitants. They were also able to
speak the language. One-half of the Italian district was surveyed by
an Italian physician and the other half by an American Social Service
Worker who knew the Italian language.
The information obtained was recorded on printed forms, which
were filled out in accordance with detailed written instructions.
Form “A” contained the necessary information concerning the family
as a whole, including statistical data of each individual, description
of the dwelling, of the sanitary condition, of the economic status, etc.
Form “B” was filled out for each individual and gave detailed
information as to the occupation and illnesses during the 1918–19 or
the 1920 influenza epidemics, or during the interval. Form “B” was
so arranged that the inspector was not called upon to make the
diagnosis of influenza, but to record the various symptoms as
described by the patient. The decision as to the diagnosis was made
later, by the author. All blank spaces were filled in with either a
positive or negative answer, so that the reviewer knew that all
questions had been asked and answered. (See Appendix.)
The inspection was begun on February 9th, at the height of the
epidemic. All records were turned in and reviewed by the author,
who blue-penciled obvious inaccuracies and incorporated directions
and questions in those instances where he desired further
information. The records were then returned to the inspectors who,
at the termination of the epidemic early in March, surveyed the
entire 10,000 a second time, checking up their first record,
correcting any inaccuracies, and adding records of additional cases of
influenza which had occurred in the interval.
The most careful statistical surveys and compilations are not
without error. We have gone into considerable detail in the preceding
description in order to demonstrate the several checks that have
been made upon the work, without which information others would
be unable to judge of the accuracy or value of our work.
Diagnostic standards for the 1918 epidemic.—All cases of illness
recorded on the reports, which have occurred during either the 1918
or the 1920 epidemics, or in the interval between them, have been
put into four groups as regards diagnosis of influenza. Cases are
designated as “Yes,” “Probable,” “Doubtful,” and “No.”
Cases of illness occurring during the months of 1918 and 1919 in
which influenza was epidemic and in which the patient remembers
that he had the more definite symptoms, (fever, headache, backache,
pain in the extremities, pneumonia) and in which he was sick at least
three days and in bed at least one day, have been designated as “Yes.”
The symptoms chosen are those most likely to be remembered. The
individual frequently does not remember all. Statements of the
absence of fever are often unreliable. Usually the headache, backache
or pain in the extremities, or even all of these are well recollected.
Cases occurring particularly during the epidemic period in which
the more definite symptoms are unknown, but who were sick three
days or longer and who were in bed at least one day, were probably
influenza. This is particularly true if there were no other symptoms
suggestive of some other definite disease. Such cases were designated
“Probable.”
Cases have been designated as doubtful when the evidence of
illness falls short of the above desiderata. Cases of true influenza may
fall into this group, either because of the extreme mildness of the
symptoms and course or because of the inaccurate memory of the
individual concerning the events of his illness sixteen months
previously. Our results show that the group of doubtful cases is
relatively very small and the number of true cases lost in this group
will be negligible.
One important reason for adhering to the above classification is
that it corresponds closely with that used by Frost and Sydenstricker,
so that our results may easily be compared with theirs.
Standards for 1920.—For 1920 the illnesses were so recent in the
minds of the patients that we have required rather full information
for making the diagnosis of “Yes.” For this designation certain
symptoms are arbitrarily required. Certain additional symptoms, if
present, serve to strengthen the diagnosis of influenza. The required
symptoms are fever, confinement to bed for one day or more and at
least two out of the following three, headache, backache and pain in
the extremities. The additional symptoms which influence the
classification are sudden onset, prostration, lachrymation, epistaxis,
and cough.
Cases designated as probable are those in which the symptoms as
enumerated above are incomplete in one or more details, but yet in
which the diagnosis of influenza would be justified. “Probable,”
therefore, means that the case is to be accepted among the list of true
influenza cases. This is particularly so when the case occurs during
the epidemic period.
“Doubtful” applies to those cases in which the evidence although
suggestive of influenza, is not complete enough to warrant such a
diagnosis. The doubtful feature may be in the lack of too great a
number of the symptoms enumerated, or the presence of symptoms
which might be due to some other disease. Certain cases occurring at
the same time with other cases of typical influenza in the same
household, and which would otherwise have been recorded as
doubtful, have been marked either “Probable” or “Yes.”
Standards of severity.—A purely arbitrary classification of severity
has been adopted. Probably no two observers would agree exactly on
a classification of this nature, but for the purposes of this study the
following will suit all requirements provided the standard used is
carried in mind throughout the comparison.
If a patient with influenza is under medical care, and the case is
one of ordinary severity, the usual period in which the individual is
advised to remain in bed is one week. This is the basis of the criteria
of severity.
Mild.—A case is recorded as mild if the individual has remained in
bed three days or less; Average, if in bed four to seven days; Severe,
if in bed over seven days. Pneumonia. This designation is added to
that of “severe” only in case the physician made such a diagnosis, or
if the evidence under “symptomatology” leaves no doubt as to the
condition.
Examples of individual exceptions to the preceding general
classification are as follows: An individual in bed two days, but sick
for three weeks might be recorded as average. A mother, with a
family of sick children and who spent no time in bed may have been
a severe case of influenza. In fact, we have allowed ourselves a
certain latitude in individual cases in classifying both the diagnosis
and the severity of the disease.
In the final tabulation we have included both the “Yes” and the
“Probable” as being cases of influenza. This has been done after a
careful comparison of both groups.
As a check upon the reliability of the work we have compared our
results for the 1918 epidemic with those reported by Frost and
Sydenstricker and have discovered that with regard to the general
subject discussed in both studies there is close agreement. This is
important in view of the long period that has elapsed between the
first pandemic and the time of our survey, and because we are unable
to compare our tables of incidence for 1918 with those for the city or
the state at large. Our own records do not place the date of
occurrence of the disease in 1918 any more closely than by month.
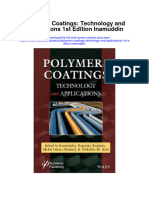
We have compared our 1920 incidence curves with those of
Massachusetts and find a close correspondence, particularly in the
date of onset, peak, and disappearance of the epidemic. We have
done likewise for the occurrence of the disease in the city of Boston
at large (Chart XIV).
In the past but few house-to-house canvasses have been made with
relation to influenza. Auerbach, following the 1889 epidemic,
collected statistics on 200 families distributed throughout the city of
Cologne. Abbott, while not conducting a canvass, did obtain a certain
amount of valuable information by letters addressed to physicians,
institutions and corporations throughout the State of Massachusetts.
There is fairly abundant literature on the disease as it occurred in
institutions. Moody and Capps, in a study of the epidemic in Chicago
in December, 1915 and January, 1916, made a survey of the
personnel and inmates of four institutions in that city. Among other
rather numerous statistical compilations from institutions we may
mention that of Hamilton and Leonard which was devoted
particularly to a study of immunity, and that of Stanley at San
Quentin Prison, California.
Garvie has reported his personal experience with influenza in an
industrial area and discusses the disease as it has occurred in
families in his private practice.
Carnwath reports a “block census” undertaken by Dr. Niven in
Manchester, England. This is of the same nature as our own work.
Reeks has made a detailed house survey of 2,757 persons in New
Britain, Connecticut. D. W. Baker has conducted somewhat similar
surveys for the New York Department of Health, and Winslow and
Rogers quote the excellent record of the Visiting Nurse Association of
New Haven, in which they have information for all of the families
cared for by the nurses. This, however, is a collected group and does
not correspond with the so-called block census.
CHART XIV.
Chart showing the actual incidence of
influenza in Boston by weeks and the
actual incidence among the 10,000
individuals surveyed by weeks during the
first three months of 1920.
Full Line—incidence in the entire city
based upon reports to the Health
Commissioner.
Dotted Line—incidence in the six
districts surveyed.
The most comprehensive and detailed work that has been done in
this line is that reported by Frost and Sydenstricker and by Frost, the
first being the result of a canvass of 46,535 persons in Maryland, and
the second a similar report based on a canvass of 130,033 persons in
several different cities of the United States. We shall have occasion to
refer to these later.
Morbidity.
There has been great actual variation in the morbidity from
influenza in the various epidemics and even in different localities
during single epidemics. Previous to 1889 there were no reliable
statistics for the disease incidence, and subsequent to that date the
records, for the reasons previously mentioned, have still been not
entirely adequate.
In the history of influenza morbidity, as in that of its mortality, we
must content ourselves for information prior to the nineteenth
century with the very general estimates made by contemporary
historians. During the last century the statistics have been more
numerous and more nearly correct. As far back as the first
recognized pandemic, 1510, the extremely high morbidity has been a
recognized characteristic. Thomas Short in speaking of this
pandemic says, “The disease ... attacked at once and raged all over
Europe, not missing a family and scarce a person.”
Pasquier in 1557 spoke of the disease as common to all individuals,
and Valleriola describes the widespread distribution of the epidemic
throughout the whole of France during that year. It spared neither
sex, age, nor rank, neither children nor aged, rich nor poor. The
mortality, however, was low, “children only, dying.” Again, Thomas
Short remarks, “This disease seized most countries very suddenly
when it entered, catching thousands the same moment.”
Of the second pandemic, 1580, Short says, “Though all had it, few
died in these countries except such as were let blood of, or had
unsound viscera.”
Thomas Sydenham remarks that in the epidemic of 1675 no one
escaped, whatever might be his age or temperament, and the disease
ran throughout whole families at once.
Molineux recorded concerning 1693, “All conditions of persons
were attacked, those residing in the country as well as those in the
city; those who lived in the fresh air and those who kept to their
rooms; those who were very strong and hardy were taken in the same
manner as the weak and spoiled; men, women and children, persons
of all ranks and stations in life, the youngest as well as the oldest.”
Schrock tells us that in Augsburg in 1712 not a house was spared by
the disease. According to Waldschmidt in Kiel, ten and more persons
were frequently taken ill in one house, and Slevogt says that the
disease was fearful because so many persons contracted it at the
same time. The disease was, however, not dangerous, for Slevogt
continues: “Fear soon vanished when it was seen that although it had
spread all over the city, it left the sick with equal rapidity.”
It is estimated that in the epidemic of 1729–1730, 60,000 people
developed the disease in Rome, 50,000 in Mayence, and 14,000 in
Turin. In London “barely one per cent. escaped.” In Lausanne one-
half of the population, then estimated at 4,000, was stricken. In
Vienna over 60,000 persons were affected. In the monasteries of
Paris so many of the inmates were suffering from the disease that no
services could be held.
Huxham is quoted in Thomson’s “Annals” as declaring concerning
the epidemic of 1732–33: “Not a house was free from it, the beggar’s
hut and the nobleman’s palace were alike subject to its attack, scarce
a person escaping either in town or country; old and young, strong
and infirm, shared the same fate.”
Finkler writes as follows concerning the epidemic of 1758: “On
Oct. 24th, Whytt continues, the pestilence began to abate. He is not
sure whether this was due to a change in the weather, or because the
disease had already attacked most people, although the latter seems
more plausible to him, particularly as he says that ‘in Edinburgh and
its vicinity not one out of six or seven escaped,’ and in other localities
it is said to have been even worse. In the north of Scotland also, the
epidemic was greatly disseminated from the middle of October to the
end of November. A young physician wrote to Robert Whytt: ‘It was
the most universal epidemic I ever saw, and I am persuaded that
more people were seized with it than escaped.’ This same physician
reported that ‘it was not at all mortal here.’”
In the epidemic of 1762, we learn from Razoux, de Brest, Saillant,
Ehrmann, that the morbidity was great while the mortality was low.
According to Grimm, nine-tenths of the inhabitants of Eisenach
contracted the disease in 1767.
Daniel Rainy, of Dublin, in describing the invasion of an
institution in 1775–76, tells us that from among 367 persons varying
in age from 12 to 90 years, 200 were taken sick. Thomas Glass says:
“There sickened in Exeter Hospital all the inmates, one hundred and
seventy-three in number; one hundred and sixty-two had coughs.
Two or three days after the hospital was invaded the city workhouse
was attacked; of the two hundred paupers housed there only very few
escaped the disease.”
Gilibert described an extraordinary morbidity in Russia in 1780–
81.
Metzger says that in 1782 the Russian catarrh was so universal
during the month of March that in many houses all the inhabitants
were attacked. During this period, “in St. Petersburg, 30,000, and in
Königsberg, 1,000 persons fell ill each day;” in Rome two-thirds of
the inhabitants were attacked; in Munich, three-fourths; and in
Vienna the severity of the epidemic compelled the authorities to
close the theaters for eight days.
The epidemics of 1788–89, 1799–1800 and of 1802–1803 were
characterized by a relatively lower morbidity than that of 1830–32,
in which the morbidity was again enormous. Likewise in 1833, the
morbidity was very great. In Prague “scarcely a house was spared by
the plague.” In Petrograd, 10,000 persons were attacked; in Berlin at
least 50,000. These are the figures of Hufeland. The Gazette
Médicale records the morbidity as being four-fifths of the total
number of inhabitants of Paris.
In 1836, according to Gluge, 40,000 persons suffered from the
disease in Berlin alone.
In London, in the 1847 epidemic, it has been calculated that at
least 250,000 individuals took sick, and in Paris, according to Marc
d’Espine, between one-fourth and one-half of the population
developed the disease, and in Geneva not less than one-third.
Leichtenstern informs us that in 1890 the early reports were made
by clinical men and were mere presumptions. They were almost
universally higher than the later statistical findings. The early
estimates for the morbidity in several German cities were from 40–
50 per cent. On the other hand, one of the highest statistical reports
recorded by Leichtenstern was for Strasbourg in which 36.5 per cent.
of the individuals became sick. The average morbidity reported by
him ran between 20 and 30 per cent. The difference is accounted for
in part by the fact that some of the very mild cases were not recorded
in the statistics, and in part by the tendency in giving estimates, to
exaggerate.
Auerbach has collected the statistics of 200 families distributed
throughout the city of Cologne. He found that 149 of these families
(75 per cent.) were attacked. In these, 235 were ill—59 men, 95
women, and 81 children. The larger number of women was explained
as due to the illness of the female servants. He estimates each family
as consisting on an average of six individuals, and concludes that 20
per cent. were taken with the disease.
Following the 1889 epidemic, Abbott concluded, on a basis of
questionaires sent out to various individuals and institutions in the
State of Massachusetts, that 39 per cent. of the entire population had
been attacked, in all about 850,000 persons.
Moody and Capps, in December, 1915, and January, 1916, made a
survey of the personnel and inmates of four institutions in Chicago,
the Michael Reese Hospital, the Illinois Training School for Nurses,
the Old Men’s Home, and St. Luke’s Hospital Nurses Training
School, making a total of 677 persons surveyed, of whom 144
developed influenza, making a percentage morbidity of 21. They
remarked that there were many others with colds who remained on
duty and were not included in the table and were not diagnosed as
influenza.
We have already described the relatively low morbidity and
mortality in the early spring epidemic in the United States.
According to Soper, the total number affected in March, 1918, at
Camp Forrest and the Reserve Officers Training Camp in the
Oglethorpe Camps was estimated at 2,900. The total strength at that
time was 28,586. The percentage morbidity then was probably a little
over 10 per cent. Dunlop, in describing the May, 1918, epidemic in
Glasgow, says that it was more limited in extent, as well as milder,
than the later epidemic.
It has been estimated that in the autumn epidemic in the United
States Army Camps one out of every four men had influenza, and one
out of every twenty-four men encamped in this country had
pneumonia. During the four autumn months of 1918, 338,343 cases
of influenza were reported to the Surgeon General’s Office; there
were 61,691 cases of pneumonia.
Woolley reports that among the soldiers at Camp Devens, Mass.
30 per cent. of the population was affected.
At Camp Humphreys, 16 per cent. of the entire personnel
developed the disease. The camp had an average strength of 26,600
individuals. Fifty-two per cent. of the entire number of cases
occurred during the peak week, which ended October 4th. The
outbreak began September 13th and ended October 18th.
Hirsch and McKinney report that an epidemic of unusual virulence
swept with great rapidity through several organizations in Camp
Grant between September 21, 1918, and October 18, 1918. During
this time 9,037 patients were admitted to the Base Hospital,
representing about one-fourth of the strength of the camp, and of
these, 26 per cent. developed pneumonia. About 11 per cent. of the
total admissions or 43 per cent. of the total cases of pneumonia died.
Referring to the report of Howard and Love, we quote as follows:
“It is probable that practically all susceptible human material in
infected camps suffered from an attack of the disease during the
continuance of the epidemic. The records from various camps
indicate that from 15 to 40 per cent. of commands suffered from an
attack of the disease. These records, as previously stated, do not
indicate in full the true incidence of the disease. Certain good results
were accomplished in some camps by the application of effective and
early isolation of patients and suspects and other measures generally
recognized as of value. It was sometimes possible to retard the
progress of the epidemic and cause it to be spread over a longer
period of time. The epidemic thus became less explosive in character,
and fewer people were under treatment at the same time. It was
possible to take better care of the sick and thus reduce the incidence
of and deaths from complicating pneumonia. It has not been shown
that such measures accomplished reduction in the absolute number
of cases of influenza occurring in one command as compared with
another.
“The ‘cantonment’ group of camps gave a much higher death rate
from influenza and its complications than the ‘tent’ camp or
‘departmental’ group. At first glance it would appear that the
different housing conditions and the more marked overcrowding in
cantonments at the time would fully account for this divergence.
Closer study, however, leads to the conclusion that geographical
location was a factor of equal or greater importance. It is well known
that the disease was most virulent and fatal in the northern, eastern
and middle west states, a district in which cantonments
predominated. In the southern and Pacific coast states, where the
most of the tent camps were located, a milder type of the disease
prevailed, with fewer resultant fatalities. Camp Lewis, Washington,
and Camp Gordon, Georgia (both cantonments), had relatively low
death rates, approximating those in nearby tent camps. On the other
hand, Camp Syracuse, New York, and Camp Colt, Pennsylvania (both
tent camps), suffered severely and reported death rates
approximating those of cantonments in the same geographical
district.”
Three waves of influenza are reported by Stanley at San Quentin
Prison. During the early wave it was estimated that over 500 of the
1,900 men in the prison population were ill. The wave lasted for a
little over two weeks. In the second epidemic there were 69 cases in
all, ten per cent. of which developed pneumonia, with two deaths.
There were fewer ambulatory cases than in the first. Three and
seven-tenths per cent. of the population was attacked in the second
epidemic, as compared with 27 per cent. in the first. In the third
epidemic there were 59 cases, with no pneumonia and no deaths.
Hernando estimates that in the Philippine Islands, 40 per cent. of
the total population of 7,000,000 was stricken with the disease. The
epidemic began in June, although it did not become severe until
October. The group of ages that suffered most were those between
ten and twenty-nine years. Hernando does not believe that the
disease was imported because cases were reported before ships
arrived from infected countries. After the importation of cases from
elsewhere the disease assumed the more severe form.
Armstrong, in reporting a survey of 700 influenza convalescents in
Framingham, Mass., remarked that 16 per cent. of the entire
population were infected with influenza. Reeks, in a house survey in
New Britain, Connecticut, found from among 2,757 persons that the
morbidity rate reached 234 per thousand. Dr. Niven found in his
block census in Manchester, England, that of 4,721 individuals, 1,108
(25 per cent.) had developed the disease. Fourteen and eight-tenths
You might also like
- Test Bank For Organizational Behaviour Concepts Controversies Applications Canadian 7th Edition Langton Robbins Judge 0134097858 9780134097855Document36 pagesTest Bank For Organizational Behaviour Concepts Controversies Applications Canadian 7th Edition Langton Robbins Judge 0134097858 9780134097855sarah.ide681100% (11)
- Diversity in Families 10Th Edition Zinn Solutions Manual Full Chapter PDFDocument23 pagesDiversity in Families 10Th Edition Zinn Solutions Manual Full Chapter PDFreagan.edwards642100% (9)
- Diversity Consciousness Opening Our Minds To People Cultures and Opportunities 4Th Edition Bucher Solutions Manual Full Chapter PDFDocument32 pagesDiversity Consciousness Opening Our Minds To People Cultures and Opportunities 4Th Edition Bucher Solutions Manual Full Chapter PDFreagan.edwards642100% (12)
- Donursing Calculations 9Th Edition Pickar Test Bank Full Chapter PDFDocument27 pagesDonursing Calculations 9Th Edition Pickar Test Bank Full Chapter PDFreagan.edwards642100% (10)
- Diversity in Families 10Th Edition Zinn Test Bank Full Chapter PDFDocument36 pagesDiversity in Families 10Th Edition Zinn Test Bank Full Chapter PDFreagan.edwards642100% (11)
- Test Bank For Organizational Behavior Tools For Success 2Nd Edition Phillips Gully 1305258347 978130525834 Full Chapter PDFDocument36 pagesTest Bank For Organizational Behavior Tools For Success 2Nd Edition Phillips Gully 1305258347 978130525834 Full Chapter PDFsarah.ide681100% (11)
- Diversity and Society Race Ethnicity and Gender 5Th Edition Healey Test Bank Full Chapter PDFDocument36 pagesDiversity and Society Race Ethnicity and Gender 5Th Edition Healey Test Bank Full Chapter PDFreagan.edwards642100% (10)
- Dynamic Business Law 4Th Edition Kubasek Solutions Manual Full Chapter PDFDocument34 pagesDynamic Business Law 4Th Edition Kubasek Solutions Manual Full Chapter PDFreagan.edwards642100% (11)
- Dosage Calculations Canadian 4Th Edition Pickar Test Bank Full Chapter PDFDocument33 pagesDosage Calculations Canadian 4Th Edition Pickar Test Bank Full Chapter PDFreagan.edwards642100% (11)
- Drugs and The Neuroscience of Behavior An Introduction To Psychopharmacology 2Nd Edition Prus Test Bank Full Chapter PDFDocument36 pagesDrugs and The Neuroscience of Behavior An Introduction To Psychopharmacology 2Nd Edition Prus Test Bank Full Chapter PDFreagan.edwards642100% (11)
- Test Bank For Organizational Behavior Managing People and Organizations 12Th Edition Griffin Phillips Gully 130550139X 9781305501393 Full Chapter PDFDocument36 pagesTest Bank For Organizational Behavior Managing People and Organizations 12Th Edition Griffin Phillips Gully 130550139X 9781305501393 Full Chapter PDFsarah.ide681100% (11)
- Test Bank For Organizational Behavior Improving Performance and Commitment in The Workplace 3Rd Edition Colquitt Lepine Wesson Full Chapter PDFDocument36 pagesTest Bank For Organizational Behavior Improving Performance and Commitment in The Workplace 3Rd Edition Colquitt Lepine Wesson Full Chapter PDFsarah.ide681100% (10)
- Download Design For Excellence In Electronics Manufacturing Cheryl Tulkoff And Greg Caswell full chapterDocument67 pagesDownload Design For Excellence In Electronics Manufacturing Cheryl Tulkoff And Greg Caswell full chapterrichard.gibson910100% (10)
- Download Surveillance Race Culture 1St Ed Edition Susan Flynn full chapterDocument67 pagesDownload Surveillance Race Culture 1St Ed Edition Susan Flynn full chapterlucille.smith144100% (6)
- Download Glencoe Literature American Literature Teachers Edition Glencoe Mcgraw Hill full chapterDocument67 pagesDownload Glencoe Literature American Literature Teachers Edition Glencoe Mcgraw Hill full chapterelizabeth.wilson414100% (3)
- Download Human Relations In Organizations Applications And Skill Building 12Th Edition Robert N Lussier full chapterDocument67 pagesDownload Human Relations In Organizations Applications And Skill Building 12Th Edition Robert N Lussier full chapteraudra.rossetti281100% (6)
- Download Atlas Of Diagnostic Hematology 1At Edition Mohamed Salama Editor full chapterDocument67 pagesDownload Atlas Of Diagnostic Hematology 1At Edition Mohamed Salama Editor full chaptergreg.vasquez490100% (5)
- Download Human Relations Strategies For Success 7Th Edition Lowell Lamberton full chapterDocument67 pagesDownload Human Relations Strategies For Success 7Th Edition Lowell Lamberton full chapteraudra.rossetti281100% (4)
- Download China Russia And Central Asian Infrastructure Fragmenting Or Reformatting The Region Peter Krasnopolsky full chapterDocument68 pagesDownload China Russia And Central Asian Infrastructure Fragmenting Or Reformatting The Region Peter Krasnopolsky full chapterjennifer.doyle352100% (6)
- Download Nanostructured Multiferroics Raneesh Balakrishnan full chapterDocument67 pagesDownload Nanostructured Multiferroics Raneesh Balakrishnan full chapterclaude.hanks203100% (4)
- Download Human Resource Management Gaining A Competitive Advantage 13Th Edition Raymond Noe full chapterDocument67 pagesDownload Human Resource Management Gaining A Competitive Advantage 13Th Edition Raymond Noe full chapteraudra.rossetti281100% (5)
- Download The Oxford Handbook Of The Bible And Ecology Oxford Handbooks Hilary Marlow Editor full chapterDocument67 pagesDownload The Oxford Handbook Of The Bible And Ecology Oxford Handbooks Hilary Marlow Editor full chapterrichard.thomas647100% (6)
- Download The Indian Ocean As A New Political And Security Region 1St Edition Samaan full chapterDocument67 pagesDownload The Indian Ocean As A New Political And Security Region 1St Edition Samaan full chaptermatthew.reed383100% (13)
- Download Human Relations In Organizations Applications And Skill Building 10Th Edition Lussier full chapterDocument67 pagesDownload Human Relations In Organizations Applications And Skill Building 10Th Edition Lussier full chapteraudra.rossetti281100% (4)
- Download Design For Advanced Manufacturing Technologies And Processes Laroux Gillespie full chapterDocument67 pagesDownload Design For Advanced Manufacturing Technologies And Processes Laroux Gillespie full chapterrichard.gibson910100% (13)
- Canadian 7th Edition Mullin Branch Gerolimon Todd and Trineer Isbn 0176570454 9780176570453Document25 pagesCanadian 7th Edition Mullin Branch Gerolimon Todd and Trineer Isbn 0176570454 9780176570453steven.bowers810100% (10)
- Download Shadow Networks Financial Disorder And The System That Caused Crisis Francisco Louca all chapterDocument67 pagesDownload Shadow Networks Financial Disorder And The System That Caused Crisis Francisco Louca all chaptercharles.lockett887100% (2)
- Download Mips Assembly Language Programming Robert Britton full chapterDocument67 pagesDownload Mips Assembly Language Programming Robert Britton full chapternellie.holloway829100% (12)
- Download Oar Feet And Opal Teeth About Copepods And Copepodologists Charles B Miller full chapterDocument62 pagesDownload Oar Feet And Opal Teeth About Copepods And Copepodologists Charles B Miller full chapteredward.rabideau868100% (2)
- Download Oakeshotts Skepticism Politics And Aesthetics 1St Edition Eric S Kos full chapterDocument67 pagesDownload Oakeshotts Skepticism Politics And Aesthetics 1St Edition Eric S Kos full chapteredward.rabideau868100% (3)
- Download Driven Rotation Self Generated Flow And Momentum Transport In Tokamak Plasmas John Rice full chapterDocument67 pagesDownload Driven Rotation Self Generated Flow And Momentum Transport In Tokamak Plasmas John Rice full chapterjennifer.scott404100% (5)
- Download Openai Api Cookbook Build Intelligent Applications Including Chatbots Virtual Assistants And Content Generators 1St Edition Henry Habib full chapterDocument68 pagesDownload Openai Api Cookbook Build Intelligent Applications Including Chatbots Virtual Assistants And Content Generators 1St Edition Henry Habib full chapterpeter.gjertsen340100% (2)
- Download Protected By The Companion A Regency Romance Ladies On Their Own Governesses And Companions Book 5 Pearson all chapterDocument68 pagesDownload Protected By The Companion A Regency Romance Ladies On Their Own Governesses And Companions Book 5 Pearson all chapterkimberly.sanders794100% (4)
- Download Human Resource Development In South Korea Theory And Cases 1St Ed Edition Doo Hun Lim full chapterDocument67 pagesDownload Human Resource Development In South Korea Theory And Cases 1St Ed Edition Doo Hun Lim full chapteraudra.rossetti281100% (5)
- Download Selenium Webdriver Recipes In C Third Edition Courtney Zhan all chapterDocument66 pagesDownload Selenium Webdriver Recipes In C Third Edition Courtney Zhan all chapterkatherine.scott740100% (4)
- Download Selective Anatomy Vol 2 2Nd Edition Vishram Singh all chapterDocument67 pagesDownload Selective Anatomy Vol 2 2Nd Edition Vishram Singh all chapterkatherine.scott740100% (5)
- Test Bank For General Organic and Biological Chemistry 7Th Edition by Stoker Isbn 1285853911 9781285853918 Full Chapter PDFDocument30 pagesTest Bank For General Organic and Biological Chemistry 7Th Edition by Stoker Isbn 1285853911 9781285853918 Full Chapter PDFrex.henderson212100% (12)
- Download Emotional Settings In Early Modern Pedagogical Culture Hamlet The Faerie Queene And Arcadia 1St Ed Edition Judith Owens full chapterDocument51 pagesDownload Emotional Settings In Early Modern Pedagogical Culture Hamlet The Faerie Queene And Arcadia 1St Ed Edition Judith Owens full chapterjulie.navas368100% (4)
- Download Survey Of Operating Systems 5Th Edition Jane Holcombe full chapterDocument67 pagesDownload Survey Of Operating Systems 5Th Edition Jane Holcombe full chapterlucille.smith144100% (6)
- Download Zinc Surfaces A Guide To Alloys Finishes Fabrication And Maintenance In Architecture And Art 1St Edition L William Zahner all chapterDocument68 pagesDownload Zinc Surfaces A Guide To Alloys Finishes Fabrication And Maintenance In Architecture And Art 1St Edition L William Zahner all chapterdevin.brown498100% (7)
- Download Design Fabrication And Calibration Of A Tall Pneumatic Oedometer Apparatus Mehrankarimpour Fardcorresponding Authorshayanzarbakhash Ghazal Rezaie Soufi Alireza Ahadi B P Naveenc full chapterDocument66 pagesDownload Design Fabrication And Calibration Of A Tall Pneumatic Oedometer Apparatus Mehrankarimpour Fardcorresponding Authorshayanzarbakhash Ghazal Rezaie Soufi Alireza Ahadi B P Naveenc full chapterrichard.gibson910100% (13)
- Financial Management Theory Practice 16Th Edition Brigham full chapterDocument51 pagesFinancial Management Theory Practice 16Th Edition Brigham full chapterlorraine.montgomery895100% (11)
- Download A Life Of Experimental Economics Volume I Forty Years Of Discovery 1St Ed Edition Vernon L Smith full chapterDocument67 pagesDownload A Life Of Experimental Economics Volume I Forty Years Of Discovery 1St Ed Edition Vernon L Smith full chapterlina.philpott914100% (7)
- Download Global Taxation How Modern Taxes Conquered The World Philipp Genschel full chapterDocument67 pagesDownload Global Taxation How Modern Taxes Conquered The World Philipp Genschel full chapterkerri.roland216100% (4)
- Download The Indian Ocean As A New Political And Security Region Frederic Grare full chapterDocument67 pagesDownload The Indian Ocean As A New Political And Security Region Frederic Grare full chaptermatthew.reed383100% (11)
- Download Human Resource Management In The Pornography Industry Business Practices In A Stigmatized Trade 1St Ed Edition David M Kopp full chapterDocument68 pagesDownload Human Resource Management In The Pornography Industry Business Practices In A Stigmatized Trade 1St Ed Edition David M Kopp full chapteraudra.rossetti281100% (5)
- Download Fostering The Emotional Well Being Of Our Youth A School Based Approach 1St Edition Philip J Lazarus Editor full chapterDocument67 pagesDownload Fostering The Emotional Well Being Of Our Youth A School Based Approach 1St Edition Philip J Lazarus Editor full chaptereddie.suero154100% (7)
- Download Emotional Choices How The Logic Of Affect Shapes Coercive Diplomacy 1St Edition Robin Markwica full chapterDocument67 pagesDownload Emotional Choices How The Logic Of Affect Shapes Coercive Diplomacy 1St Edition Robin Markwica full chapterjulie.navas368100% (6)
- Download Pseudo Noun Incorporation And Differential Object Marking Imke Driemel 2 all chapterDocument67 pagesDownload Pseudo Noun Incorporation And Differential Object Marking Imke Driemel 2 all chapterjeanne.giacchino850100% (3)
- Download Mirroring Brains How We Understand Others From The Inside Giacomo Rizzolatti full chapterDocument67 pagesDownload Mirroring Brains How We Understand Others From The Inside Giacomo Rizzolatti full chapternellie.holloway829100% (10)
- Download Glencoe Short Stories 1 1St Edition Jeffrey D Wilhelm Et Al full chapterDocument67 pagesDownload Glencoe Short Stories 1 1St Edition Jeffrey D Wilhelm Et Al full chapterelizabeth.wilson414100% (4)
- Download Obesity And Gynecology 2Nd Edition Tahir A Mahmood Editor full chapterDocument67 pagesDownload Obesity And Gynecology 2Nd Edition Tahir A Mahmood Editor full chapteredward.rabideau868100% (4)
- Download Self And Identity Trenton Merricks all chapterDocument67 pagesDownload Self And Identity Trenton Merricks all chapterkatherine.scott740100% (3)
- Download Glencoe Short Stories 2 1St Edition Jeffrey D Wilhelm Et Al full chapterDocument67 pagesDownload Glencoe Short Stories 2 1St Edition Jeffrey D Wilhelm Et Al full chapterelizabeth.wilson414100% (4)
- Download International Accounting 6Th International Student Edition Edition Timothy Doupnik full chapterDocument67 pagesDownload International Accounting 6Th International Student Edition Edition Timothy Doupnik full chaptertimothy.parrott698100% (3)
- Download The Protagonists Journey Scott Myers full chapterDocument67 pagesDownload The Protagonists Journey Scott Myers full chaptertheodore.combs684100% (4)
- Download Nelsons Annual Preachers Sourcvolume 1 Kent Spann David Wheeler Spann full chapterDocument67 pagesDownload Nelsons Annual Preachers Sourcvolume 1 Kent Spann David Wheeler Spann full chapterbarbara.holmes539100% (6)
- Download Polymers Coatings Technology And Applications 1St Edition Inamuddin all chapterDocument67 pagesDownload Polymers Coatings Technology And Applications 1St Edition Inamuddin all chaptermark.clark755100% (5)
- Basic Principles Of Induction Logging Electromagnetic Methods In Borehole Geophysics 1St Edition Edition Alexander Kaufman And Gregory Itskovich Auth full chapterDocument52 pagesBasic Principles Of Induction Logging Electromagnetic Methods In Borehole Geophysics 1St Edition Edition Alexander Kaufman And Gregory Itskovich Auth full chapterguy.smith308100% (3)
- Organizational Behaviou Understanding and Managing Life at Work Canadian Edition Canadian 9th Edition Johns Test BankDocument18 pagesOrganizational Behaviou Understanding and Managing Life at Work Canadian Edition Canadian 9th Edition Johns Test BankKaylaWalkerncas100% (48)
- Locus of Control in Who Moved My CheeseDocument2 pagesLocus of Control in Who Moved My CheeseRA OrtizNo ratings yet
- Workaholism. Family OutcomesDocument13 pagesWorkaholism. Family Outcomessildia009100% (1)
- UTS Module 12-14Document18 pagesUTS Module 12-14mikaela thereseNo ratings yet
- Performance ExpectancyDocument12 pagesPerformance Expectancyfadli adninNo ratings yet
- Meaning of Money: Extension and Exploration of The Money Ethic Scale in A Sample of University Students in TaiwanDocument7 pagesMeaning of Money: Extension and Exploration of The Money Ethic Scale in A Sample of University Students in TaiwanMiguel Hernandes JuniorNo ratings yet
- TB 08Document45 pagesTB 08Ebtehal TamerNo ratings yet
- CBFS-Module 3 - Personality, Ability, Attitudes and ValuesDocument13 pagesCBFS-Module 3 - Personality, Ability, Attitudes and ValuesIrish Claire BaquiranNo ratings yet
- Southeast Asia Psychology Journal Vol.6, (2018) 16-25Document10 pagesSoutheast Asia Psychology Journal Vol.6, (2018) 16-25Viqih AryanataNo ratings yet
- Handout 2Document36 pagesHandout 2xandra joy abadezaNo ratings yet
- Helpless To Mastery PDFDocument268 pagesHelpless To Mastery PDFmaathheusNo ratings yet
- Teaching Slides Chapter 4Document69 pagesTeaching Slides Chapter 4MARTA ARCE MARTINEZNo ratings yet
- Locus of ControlDocument12 pagesLocus of ControlmansiNo ratings yet
- Causes of Dropout Among Secondary School Students in Ughelli South Local Government Area of Delta StateDocument54 pagesCauses of Dropout Among Secondary School Students in Ughelli South Local Government Area of Delta StateJawad AminNo ratings yet
- Rotter Locus of ControlDocument4 pagesRotter Locus of Controlnela yuliya dewiNo ratings yet
- Organizational Behaviour - MGT502 Power Point Slides Lecture 8Document46 pagesOrganizational Behaviour - MGT502 Power Point Slides Lecture 8QasimNo ratings yet
- A-File Description - SpanishDocument23 pagesA-File Description - Spanishmayra almaNo ratings yet
- Psy Tests U GentDocument10 pagesPsy Tests U GentECE MISIRLINo ratings yet
- MAPC PracticalsDocument2 pagesMAPC PracticalsSekhar ViswabNo ratings yet
- Entrepreneurial IntentionDocument13 pagesEntrepreneurial Intentionnishantha12100% (5)
- Thesis On Employee Job PerformanceDocument8 pagesThesis On Employee Job Performancegxgtpggld100% (2)
- Lawrence M Miller - Building Team From Forming To PerformingDocument80 pagesLawrence M Miller - Building Team From Forming To PerformingKasih Ditaningtyas Sari PratiwiNo ratings yet
- Dilmah TeaDocument18 pagesDilmah Teasshreyas100% (1)
- NIH Public Access: Author ManuscriptDocument15 pagesNIH Public Access: Author ManuscriptAbraxas LuchenkoNo ratings yet
- Locus of Control, Happiness, and Self-EsteemDocument11 pagesLocus of Control, Happiness, and Self-Esteemjessie meciNo ratings yet
- Effect of Empowering Leadership On Work EngagementDocument10 pagesEffect of Empowering Leadership On Work EngagementErmelina BacatanNo ratings yet
- ManagementDocument107 pagesManagementabhijitcet100% (1)
- Cognitive Emotional Theories and TraumaDocument21 pagesCognitive Emotional Theories and TraumaumibrahimNo ratings yet
- EDG 3661 - CBI AssignmentDocument3 pagesEDG 3661 - CBI AssignmentMary Miller FoltzNo ratings yet
- Stress Management Model PaperDocument6 pagesStress Management Model PaperkrishnaNo ratings yet
- Career Choice FactorsDocument3 pagesCareer Choice FactorsAlexandria RaboNo ratings yet
- Straight-A Study Skills: More Than 200 Essential Strategies to Ace Your Exams, Boost Your Grades, and Achieve Lasting Academic SuccessFrom EverandStraight-A Study Skills: More Than 200 Essential Strategies to Ace Your Exams, Boost Your Grades, and Achieve Lasting Academic SuccessRating: 3.5 out of 5 stars3.5/5 (6)
- The Everything Guide to Study Skills: Strategies, tips, and tools you need to succeed in school!From EverandThe Everything Guide to Study Skills: Strategies, tips, and tools you need to succeed in school!Rating: 4.5 out of 5 stars4.5/5 (6)
- Make It Stick by Peter C. Brown, Henry L. Roediger III, Mark A. McDaniel - Book Summary: The Science of Successful LearningFrom EverandMake It Stick by Peter C. Brown, Henry L. Roediger III, Mark A. McDaniel - Book Summary: The Science of Successful LearningRating: 4.5 out of 5 stars4.5/5 (55)
- A-level Maths Revision: Cheeky Revision ShortcutsFrom EverandA-level Maths Revision: Cheeky Revision ShortcutsRating: 3.5 out of 5 stars3.5/5 (8)
- TEF Canada Expression Écrite : 150 Topics To SucceedFrom EverandTEF Canada Expression Écrite : 150 Topics To SucceedRating: 4.5 out of 5 stars4.5/5 (17)
- Math Olympiad Contests Preparation For Grades 4-8: Competition Level Math for Middle School Students to Win MathCON, AMC-8, MATHCOUNTS, and Math LeaguesFrom EverandMath Olympiad Contests Preparation For Grades 4-8: Competition Level Math for Middle School Students to Win MathCON, AMC-8, MATHCOUNTS, and Math LeaguesNo ratings yet
- TEST TAKING STRATEGIES FOR EVERYONE: A Comprehensive Guide to Mastering Test Taking (2023 Beginner Crash Course)From EverandTEST TAKING STRATEGIES FOR EVERYONE: A Comprehensive Guide to Mastering Test Taking (2023 Beginner Crash Course)No ratings yet
- BCBA Exam Prep A Study Guide to Practice Test Questions With Answers and Master the Board Certified Behavior Analyst ExaminationFrom EverandBCBA Exam Prep A Study Guide to Practice Test Questions With Answers and Master the Board Certified Behavior Analyst ExaminationNo ratings yet
- A PhD Rollercoaster: A Diary of The Ups And Downs of Being a Doctoral StudentFrom EverandA PhD Rollercoaster: A Diary of The Ups And Downs of Being a Doctoral StudentRating: 4.5 out of 5 stars4.5/5 (16)
- Real Stories: The All-Inclusive Textbook for Developmental Writing and ReadingFrom EverandReal Stories: The All-Inclusive Textbook for Developmental Writing and ReadingNo ratings yet
- 1,001 Questions & Answers for the CWI Exam: Welding Metallurgy and Visual Inspection Study GuideFrom Everand1,001 Questions & Answers for the CWI Exam: Welding Metallurgy and Visual Inspection Study GuideRating: 3.5 out of 5 stars3.5/5 (7)
- 700 Driving Theory Test Questions & Answers: Updated Study Guide With Over 700 Official Style Practise Questions For Cars - Based Off the Highway CodeFrom Everand700 Driving Theory Test Questions & Answers: Updated Study Guide With Over 700 Official Style Practise Questions For Cars - Based Off the Highway CodeNo ratings yet