You might also like
- New Patient Medical History Form 2023 03 29Document2 pagesNew Patient Medical History Form 2023 03 29Trouvaille medicoNo ratings yet
- Modified SBAR Tool Template Example FCG FinalDocument2 pagesModified SBAR Tool Template Example FCG Finalbernie hewsonNo ratings yet
- MSE Level 3Document4 pagesMSE Level 3MARY BARACHIEL SARDUANo ratings yet
- MCN Questionnaire DraftDocument8 pagesMCN Questionnaire DraftJenny AjocNo ratings yet
- 1 Newborn Assessment NU 205 CWDocument9 pages1 Newborn Assessment NU 205 CWGuerlene JeromeNo ratings yet
- NURS 481L - Patient Profile DatabaseDocument7 pagesNURS 481L - Patient Profile DatabaseinnocentforeternityNo ratings yet
- Peds WW Form1 - 1Document17 pagesPeds WW Form1 - 1Karess AvilloNo ratings yet
- Legal History and PEDocument1 pageLegal History and PELoreto District Hospital LDHNo ratings yet
- Massage Intake Form Template 12Document2 pagesMassage Intake Form Template 12Roxanne Cabreros (Xanne)No ratings yet
- New Patient/Consultation Form: AllergiesDocument2 pagesNew Patient/Consultation Form: AllergiesAlexander Flores SaraviaNo ratings yet
- Family Healthcare Program FORMDocument12 pagesFamily Healthcare Program FORMRaquel ReyesNo ratings yet
- DSMES Assessment Template (Chart 7)Document4 pagesDSMES Assessment Template (Chart 7)Bryan MorteraNo ratings yet
- Mental Health Plan Assessment Form: Relationship PhoneDocument6 pagesMental Health Plan Assessment Form: Relationship Phonealotfya100% (1)
- Https Whitewolfdental - Com Wp-Content Uploads 2013 06 Patient-Info-Sheet-71Document2 pagesHttps Whitewolfdental - Com Wp-Content Uploads 2013 06 Patient-Info-Sheet-71Linh NguyễnNo ratings yet
- Alabama Mental Health Intake & Evaluation: Current FunctioningDocument3 pagesAlabama Mental Health Intake & Evaluation: Current FunctioningRobertoTapiaHidalgoNo ratings yet
- محمد عزت قيسيDocument11 pagesمحمد عزت قيسيmotasem.med120No ratings yet
- Massage and All Facial Tratments (AutoRecovered)Document9 pagesMassage and All Facial Tratments (AutoRecovered)Vivi AnaNo ratings yet
- Birth History/Parent Concerns Physical Examination (Unclothed)Document3 pagesBirth History/Parent Concerns Physical Examination (Unclothed)brian@coombsmd.comNo ratings yet
- Provinical Pews Flowsheet August 2016Document7 pagesProvinical Pews Flowsheet August 2016Nisak HumairokNo ratings yet
- Health I StoryDocument1 pageHealth I StorySuzanne DeaultNo ratings yet
- Health History: Print Your Answers. Please Print ClearlyDocument4 pagesHealth History: Print Your Answers. Please Print Clearlymarwan el deebNo ratings yet
- Physical Examination Guide: LesionsDocument4 pagesPhysical Examination Guide: LesionsJenna Liezl BocoNo ratings yet
- Case Study 5Document9 pagesCase Study 5Vivi AnaNo ratings yet
- Community Survey - Profiling-FormDocument6 pagesCommunity Survey - Profiling-FormrodcyruskentNo ratings yet
- Nmanisce@ibew - On.ca: Street City Postal CodeDocument1 pageNmanisce@ibew - On.ca: Street City Postal Code100135007No ratings yet
- Client Information Sheet NCM107Document4 pagesClient Information Sheet NCM107Rolland Ray MendozaNo ratings yet
- Comprehensive Nursing Assessment: Dengue Haemorrhagic Fever)Document4 pagesComprehensive Nursing Assessment: Dengue Haemorrhagic Fever)Devita PutriNo ratings yet
- Pediatric Initial Patient HistoryDocument11 pagesPediatric Initial Patient HistoryLinh TrịnhNo ratings yet
- Primary Care History FormDocument2 pagesPrimary Care History FormAnonymous i8SazYNo ratings yet
- Clinical Pathway ACSDocument7 pagesClinical Pathway ACSherrerachaimNo ratings yet
- 3507P 11Document2 pages3507P 11Hbk RajneeshNo ratings yet
- Clinical Duties - Diagnostic RadiologyDocument2 pagesClinical Duties - Diagnostic RadiologyKim ZhouNo ratings yet
- 1 Patient Health History and Health Assessment FormatDocument8 pages1 Patient Health History and Health Assessment FormatKn VelasquezNo ratings yet
- My Birth Plan: For Labor Immediately After DeliveryDocument1 pageMy Birth Plan: For Labor Immediately After DeliveryLiNin MintonNo ratings yet
- 1 Patient Health History and Health Assessment FormatDocument9 pages1 Patient Health History and Health Assessment Formatgwendee ealdamaNo ratings yet
- Health Examination RecordDocument4 pagesHealth Examination Recordmary joy dela cruzNo ratings yet
- 36316-IUCT22 Client Consultation Form v1Document7 pages36316-IUCT22 Client Consultation Form v1michellepayne1806No ratings yet
- Medical HistoryDocument2 pagesMedical HistoryMiguel San JuanNo ratings yet
- Recommendations To Transportation On The CaseDocument1 pageRecommendations To Transportation On The CaseАнна СкубаNo ratings yet
- Food Donation Ingredients & AllergensDocument3 pagesFood Donation Ingredients & AllergensAndrea FortNo ratings yet
- Treatment Evidence Form: iUBT431 - Facial Electrical TreatmentsDocument5 pagesTreatment Evidence Form: iUBT431 - Facial Electrical TreatmentsVivi AnaNo ratings yet
- Documents in SpanishDocument7 pagesDocuments in SpanishJose Carlos Nahuel Jesiotr DiazNo ratings yet
- Patient Intake FormsDocument5 pagesPatient Intake Formsapi-267621567No ratings yet
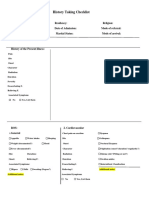
- History Taking ListsDocument4 pagesHistory Taking ListsZahraa DuraidNo ratings yet
- Medical and Support Information Form: PG From Account)Document11 pagesMedical and Support Information Form: PG From Account)Kamala ValluripalliNo ratings yet
- Rhinessa Women's Q EnglishDocument8 pagesRhinessa Women's Q EnglishDavis ShirleyNo ratings yet
- Case Study Template BeautyDocument8 pagesCase Study Template BeautyVivi AnaNo ratings yet
- Your Family Medical History Questionnaire: All About YouDocument5 pagesYour Family Medical History Questionnaire: All About YouLemuel Glenn BautistaNo ratings yet
- Lee Dentist NPT-Info - OnepageDocument1 pageLee Dentist NPT-Info - Onepagecig3fNo ratings yet
- PENGKAJIANDocument3 pagesPENGKAJIANIRSAD SADAMNo ratings yet
- Case Study Template BeautyDocument8 pagesCase Study Template BeautyVivi VivianaNo ratings yet
- Health HistoryDocument12 pagesHealth HistoryGreta D RNNo ratings yet
- Who Standardized Emergency Unit Form TraumaDocument2 pagesWho Standardized Emergency Unit Form TraumaJm uniteNo ratings yet
- Bariatrics Weight Loss IntakeDocument12 pagesBariatrics Weight Loss IntakeErin abelsNo ratings yet
- Intra-Operative Nurse's RecordDocument2 pagesIntra-Operative Nurse's RecordAnna Margarett Mutia CaballarNo ratings yet
- Acute Gastritis CPG FINALDocument5 pagesAcute Gastritis CPG FINALkimadlo656No ratings yet
- New Client Intake FormDocument1 pageNew Client Intake FormTori BaileyNo ratings yet
- PE Maternal FormDocument4 pagesPE Maternal FormJenna Liezl BocoNo ratings yet
- If Success Is Your Goal, These Are the Rules: These Are Some Vital RulesFrom EverandIf Success Is Your Goal, These Are the Rules: These Are Some Vital RulesNo ratings yet
- Lesson 11 Gech02 FinalsDocument14 pagesLesson 11 Gech02 FinalsSEAN JODI M. COSEPENo ratings yet
- Casabar Crislyn Exercise 32 PDFDocument2 pagesCasabar Crislyn Exercise 32 PDFSEAN JODI M. COSEPENo ratings yet
- Guide Questions and Pointers For Film Analysis APAG SSC 002Document1 pageGuide Questions and Pointers For Film Analysis APAG SSC 002SEAN JODI M. COSEPENo ratings yet
- Biochem Expt 6Document5 pagesBiochem Expt 6SEAN JODI M. COSEPENo ratings yet
- Biochem Expt 4 - FLDocument7 pagesBiochem Expt 4 - FLSEAN JODI M. COSEPENo ratings yet
- Biochem Expt 3 - FLDocument5 pagesBiochem Expt 3 - FLSEAN JODI M. COSEPENo ratings yet
- TFN Midterms TransesDocument14 pagesTFN Midterms TransesSEAN JODI M. COSEPENo ratings yet
- Nursing Process Assessment and DiagnosisDocument4 pagesNursing Process Assessment and DiagnosisSEAN JODI M. COSEPENo ratings yet
- PRELIM OUTPUT SelfDocument2 pagesPRELIM OUTPUT SelfSEAN JODI M. COSEPENo ratings yet
- Finals - Ela - BiochemDocument6 pagesFinals - Ela - BiochemSEAN JODI M. COSEPENo ratings yet
- Paper AnalysisDocument4 pagesPaper AnalysisLayali MassisNo ratings yet
- PHCP312 SyllabusDocument9 pagesPHCP312 SyllabusDanica PamintuanNo ratings yet
- Biology Viral DiseasesDocument11 pagesBiology Viral DiseasesPrasoon Singh RajputNo ratings yet
- Amit Agrawal 2303705Document4 pagesAmit Agrawal 2303705Anushtha AgrawalNo ratings yet
- Stanford Hospital & Clinics Antimicrobial Dosing Reference Guide 2013Document3 pagesStanford Hospital & Clinics Antimicrobial Dosing Reference Guide 2013SANCHOSKYNo ratings yet
- Hemorrhoids Case ReportDocument8 pagesHemorrhoids Case ReportTetipuspita SariNo ratings yet
- Arab Board Exam 2008Document7 pagesArab Board Exam 2008alaaNo ratings yet
- A Comparative Study OF NIHSS Between Ischemic Stroke Patients With and Without Risk FactorsDocument4 pagesA Comparative Study OF NIHSS Between Ischemic Stroke Patients With and Without Risk FactorsKlinik HanisNo ratings yet
- CEU Somatic Symptom and Related DisordersDocument78 pagesCEU Somatic Symptom and Related DisordersErika Louise MiChelle Cua NavasNo ratings yet
- Anaphylaxis Guidelines PosterDocument1 pageAnaphylaxis Guidelines PosterBabo SanNo ratings yet
- Pandemic Pathogens ReportDocument17 pagesPandemic Pathogens ReportMaxwell SmartNo ratings yet
- Coronary Artery Disease: Therapeutics and Drug Discovery: Miao Wang EditorDocument345 pagesCoronary Artery Disease: Therapeutics and Drug Discovery: Miao Wang EditorAdina Alexandra CNo ratings yet
- Diagnosis and Treatment of Radiation ProctitisDocument2 pagesDiagnosis and Treatment of Radiation ProctitispatNo ratings yet
- Using Master Tung's Gallbladder Points For Diseases of The Head and NeckDocument2 pagesUsing Master Tung's Gallbladder Points For Diseases of The Head and NeckTrần Hồ Thạnh Phú100% (1)
- Faktor Risiko Tuberkulosis Pada Anak: Muhammad S. D. Wijaya, Max F. J. Mantik, Novie H. RampenganDocument10 pagesFaktor Risiko Tuberkulosis Pada Anak: Muhammad S. D. Wijaya, Max F. J. Mantik, Novie H. RampenganMasithaNo ratings yet
- Case Presentation: Pre EclamsiaDocument66 pagesCase Presentation: Pre EclamsiaEugene Evan Endaya UyNo ratings yet
- Exciplex® 308 NM Phototherapy: Autoimmune Disease?Document28 pagesExciplex® 308 NM Phototherapy: Autoimmune Disease?Band CafeNo ratings yet
- 7-Cardiology and Respiratory MedicineDocument373 pages7-Cardiology and Respiratory Medicinethisar100% (6)
- Tool Box Talk - Working in Hot WeatherDocument1 pageTool Box Talk - Working in Hot WeatherMobashir MahmoodNo ratings yet
- Association of Loneliness With Suicide Risk and Depression in Individuals With Schizophrenia: Moderating Effects of Self - Esteem and Perceived Support From Families and FriendsDocument7 pagesAssociation of Loneliness With Suicide Risk and Depression in Individuals With Schizophrenia: Moderating Effects of Self - Esteem and Perceived Support From Families and Friends簡千芮No ratings yet
- 5f40e819948bc198-209-GP-Epidemiological-S Srujana Reddy-5971861561Document12 pages5f40e819948bc198-209-GP-Epidemiological-S Srujana Reddy-5971861561MOHAMMED KHAYYUMNo ratings yet
- Absent End-Diastolic Velocity in The Umbilical Artery and Its Clinical SignificanceDocument12 pagesAbsent End-Diastolic Velocity in The Umbilical Artery and Its Clinical Significancejakob_saleanNo ratings yet
- Newborn AssessmentDocument24 pagesNewborn Assessmentvincentsharon100% (2)
- Pathological FractureDocument92 pagesPathological FractureSeptyAuliaNo ratings yet
- OCD Case ReportDocument6 pagesOCD Case ReportMariah Ainna B. MatienzoNo ratings yet
- C2b - Hydatidiform Mole (H-Mole Pregnancy) ContentDocument4 pagesC2b - Hydatidiform Mole (H-Mole Pregnancy) ContentGLADYS MAY GUDELOS MEJIASNo ratings yet
- Interpretations: How To Use Faecal Elastase TestingDocument6 pagesInterpretations: How To Use Faecal Elastase TestingguschinNo ratings yet
- Syncope & PalpitationDocument2 pagesSyncope & PalpitationArjunNo ratings yet
- Best Cardiologist in Hyderabad Dr. SanjeevDocument6 pagesBest Cardiologist in Hyderabad Dr. SanjeevBest CardiologistinHyderabadNo ratings yet
- ELGAMAL HATEM Topic No.11Document6 pagesELGAMAL HATEM Topic No.11HATEM ELGAMALNo ratings yet