You might also like
- Credit Card Generator & Validator - Valid Visa Numbers - CardGuruDocument8 pagesCredit Card Generator & Validator - Valid Visa Numbers - CardGuruRahul Singh BhatiNo ratings yet
- Macbook Pro (14-Inch, 2021) : Repair ManualDocument162 pagesMacbook Pro (14-Inch, 2021) : Repair Manualmiruna apostolNo ratings yet
- COA C2018-002 AnnexA-PIFDocument3 pagesCOA C2018-002 AnnexA-PIFRetcheNo ratings yet
- Smart InfrastructureDocument19 pagesSmart Infrastructurekapil100% (1)
- Incident Check-In List ICS 211: Date: TimeDocument6 pagesIncident Check-In List ICS 211: Date: TimeAlo Rio100% (1)
- Module-7 Thin and Thick CylinderDocument52 pagesModule-7 Thin and Thick CylinderRahul SinghNo ratings yet
- Incident Check-In List ICS 211: Date: TimeDocument1 pageIncident Check-In List ICS 211: Date: TimeBuddzilla Francisco33% (3)
- Annexes 033 PDFDocument242 pagesAnnexes 033 PDFanas9889100% (2)
- Training Requisition FormatDocument1 pageTraining Requisition FormatSGNo ratings yet
- Incident Check-In List ICS 211: Date: TimeDocument6 pagesIncident Check-In List ICS 211: Date: TimePELIGRO RAMIENo ratings yet
- PaascheAirbrushCat 2014 PDFDocument24 pagesPaascheAirbrushCat 2014 PDFDavid ZimmermanNo ratings yet
- Ullage Table of MT ELISEDocument65 pagesUllage Table of MT ELISEAbu Syeed Md. Aurangzeb Al Masum100% (1)
- Annex B-2 RR 11-2018Document1 pageAnnex B-2 RR 11-2018Alo Rio100% (3)
- Registration Form For EIARC & EIA PreparerDocument1 pageRegistration Form For EIARC & EIA PreparerRonnie EncarnacionNo ratings yet
- Ics 211 - Checkin ListDocument1 pageIcs 211 - Checkin ListMilan TarigaNo ratings yet
- Ip Ics - Ics 211Document1 pageIp Ics - Ics 211Alo RioNo ratings yet
- Bics Ics 211Document6 pagesBics Ics 211DocJogy SalazarNo ratings yet
- Timesheet VLCDocument1 pageTimesheet VLCOoi Khia ShengNo ratings yet
- RIDS With NRCen NCR Administering Ofcr LTJG BilagotDocument3 pagesRIDS With NRCen NCR Administering Ofcr LTJG BilagotMark Joe Cris MangulabnanNo ratings yet
- MO Form HRGA 0001 Request For RecruitmentDocument2 pagesMO Form HRGA 0001 Request For RecruitmentNovita YuliatantriNo ratings yet
- Application Form For Coc (Organization) Fire Safety PractitionerDocument2 pagesApplication Form For Coc (Organization) Fire Safety PractitionerRyan PattNo ratings yet
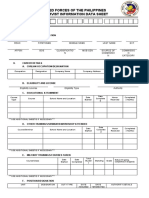
- Armed Forces of The Philippines Reservist Information Data SheetDocument3 pagesArmed Forces of The Philippines Reservist Information Data SheetJoevell Dela CruzNo ratings yet
- New Format Rids 1Document4 pagesNew Format Rids 1Aly VNo ratings yet
- 1 Personal Details: OM 4.3.1 Application FormDocument2 pages1 Personal Details: OM 4.3.1 Application FormVikkiVikiNo ratings yet
- MI 273 SIRB SQC ApplicationDocument2 pagesMI 273 SIRB SQC ApplicationHERMAN DAGIONo ratings yet
- Appln Form 02 2011Document2 pagesAppln Form 02 2011Mahadeva PrasadNo ratings yet
- Armed Forces of The Philippines Reservist Information Data SheetDocument3 pagesArmed Forces of The Philippines Reservist Information Data SheetAngelica Batario100% (2)
- RIDSDocument3 pagesRIDSJaden GonzagaNo ratings yet
- (Tanker) CVDocument5 pages(Tanker) CVMMS SNo ratings yet
- Nrmis RidsDocument3 pagesNrmis RidsBert Cesar G.No ratings yet
- Application Form Non-Teaching FinalDocument11 pagesApplication Form Non-Teaching FinalAbhishek AnandNo ratings yet
- Cash Request Form SampleDocument1 pageCash Request Form SampleEssie Noble KariNo ratings yet
- Armed Forces of The Philippines Reservist Information Data SheetDocument4 pagesArmed Forces of The Philippines Reservist Information Data SheetK Dela CruzNo ratings yet
- Application Form For Non-Teaching Posts 63-22Document6 pagesApplication Form For Non-Teaching Posts 63-22MohammedNo ratings yet
- Candidate Profile Form Expat - TemplateDocument3 pagesCandidate Profile Form Expat - TemplateSalman SiddiquiNo ratings yet
- Drilltech Offshore - Rig-Crew - CVDocument2 pagesDrilltech Offshore - Rig-Crew - CVMohd AhmadNo ratings yet
- Rids FormDocument4 pagesRids Formstephen allan ambalaNo ratings yet
- LT Marine Application TemplateDocument4 pagesLT Marine Application TemplateEirvin JamesNo ratings yet
- Ics Form 211, Incident Check-In List (v3.1)Document4 pagesIcs Form 211, Incident Check-In List (v3.1)jprmargesNo ratings yet
- Seastar Ship Management Private Limited: Application / Personal Data Form For Officer'S & RatingsDocument4 pagesSeastar Ship Management Private Limited: Application / Personal Data Form For Officer'S & RatingsrupalNo ratings yet
- Data Captured FormDocument3 pagesData Captured FormkeiferrosalesNo ratings yet
- UntitledDocument3 pagesUntitledCarlos alfredo Caraveo castilloNo ratings yet
- Format For Applying / Renewal of Accreditation: (Cover Letter)Document10 pagesFormat For Applying / Renewal of Accreditation: (Cover Letter)Anurag kumarNo ratings yet
- ASSESSMENT APPLICATION FORM (Blank)Document2 pagesASSESSMENT APPLICATION FORM (Blank)Sam BlackNo ratings yet
- CJ1 Access Request Form PDFDocument1 pageCJ1 Access Request Form PDFFitra NandesNo ratings yet
- MI 273 SIRB SQC ApplicationDocument2 pagesMI 273 SIRB SQC ApplicationSaro ShyamNo ratings yet
- Ics 211 - MobileDocument3 pagesIcs 211 - MobileVlademir Geb DubouzetNo ratings yet
- Rids FormDocument3 pagesRids FormgianblazinNo ratings yet
- Sample ItineraryDocument1 pageSample Itineraryshadow shadowNo ratings yet
- Leave Application FormatDocument1 pageLeave Application FormatmohdNo ratings yet
- Msme - Technology Development Center, Chennai Application FormDocument1 pageMsme - Technology Development Center, Chennai Application FormRajesh RamakrishnanNo ratings yet
- Rids New FormatDocument4 pagesRids New Formatpj borresNo ratings yet
- Application Form: Technical Education and Skills Development AuthorityDocument2 pagesApplication Form: Technical Education and Skills Development AuthorityKarl OlaveNo ratings yet
- FP-1 Application FormDocument11 pagesFP-1 Application FormtashfinNo ratings yet
- Application Form Rev 4Document4 pagesApplication Form Rev 4MARK ANTHONY TIONGSONNo ratings yet
- Ip Ics - Ics 204Document1 pageIp Ics - Ics 204Alo RioNo ratings yet
- DPR Template For Projects Under Agriculture Infrastructure FundDocument7 pagesDPR Template For Projects Under Agriculture Infrastructure FundRajesh BogulNo ratings yet
- Employment Application FormDocument3 pagesEmployment Application FormKamranNo ratings yet
- Flag CRA I10Document3 pagesFlag CRA I10Today viralszNo ratings yet
- Appendix 11 ORSDocument4 pagesAppendix 11 ORSgennadacaweNo ratings yet
- CL Form Forteaching Staffs NewDocument1 pageCL Form Forteaching Staffs NewcsebitannaNo ratings yet
- Fo Fgo 2 1 Application Form (Engine Department)Document2 pagesFo Fgo 2 1 Application Form (Engine Department)Emerald MedranoNo ratings yet
- Employee Personal Information Form (TGBS)Document3 pagesEmployee Personal Information Form (TGBS)vineetkguptNo ratings yet
- 830a - Crew Application Form - Sea ServiceDocument3 pages830a - Crew Application Form - Sea ServiceJingle PalmaNo ratings yet
- EDD.1.F.012 - Ecozone Utilities EnterpriseDocument12 pagesEDD.1.F.012 - Ecozone Utilities EnterpriseMeowthemathicianNo ratings yet
- AME Written ExamDocument2 pagesAME Written Examhimanshu55No ratings yet
- Popdev Action Plan DraftDocument31 pagesPopdev Action Plan DraftAlo RioNo ratings yet
- Inventory 20Document6 pagesInventory 20Alo RioNo ratings yet
- POPDEV IndicatorsDocument9 pagesPOPDEV IndicatorsAlo RioNo ratings yet
- Population 2015-2023Document6 pagesPopulation 2015-2023Alo RioNo ratings yet
- PopDev Programs and ServicesDocument28 pagesPopDev Programs and ServicesAlo RioNo ratings yet
- R and P FunctionsDocument3 pagesR and P FunctionsAlo RioNo ratings yet
- Ip Ics - Ics 208Document1 pageIp Ics - Ics 208Alo RioNo ratings yet
- Ics 205Document1 pageIcs 205Alo RioNo ratings yet
- Ip Ics - Ics 215Document1 pageIp Ics - Ics 215Alo RioNo ratings yet
- Ip Ics - Ics 215aDocument1 pageIp Ics - Ics 215aAlo RioNo ratings yet
- Ics 208Document1 pageIcs 208Alo RioNo ratings yet
- Ics 204Document1 pageIcs 204Alo RioNo ratings yet
- Communications Plan ICS 205Document2 pagesCommunications Plan ICS 205Alo RioNo ratings yet
- Multi 10-6Document21 pagesMulti 10-6Alo RioNo ratings yet
- Medical Plan ICS 206Document2 pagesMedical Plan ICS 206Alo RioNo ratings yet
- Unt Research Magazine 2018Document48 pagesUnt Research Magazine 2018Alo RioNo ratings yet
- Incident Objectives ICS 202: From (Date and Time) : To (Date and Time)Document2 pagesIncident Objectives ICS 202: From (Date and Time) : To (Date and Time)Alo RioNo ratings yet
- Salary Cafoa 2022 - J.ODocument13 pagesSalary Cafoa 2022 - J.OAlo RioNo ratings yet
- Assignment List ICS 204: From (Date and Time) : To (Date and Time) : Group: Division: Staging AreaDocument3 pagesAssignment List ICS 204: From (Date and Time) : To (Date and Time) : Group: Division: Staging AreaAlo RioNo ratings yet
- (Sample Format) For Livestock Raising Only - Hog Raising: Farm Plan and BudgetDocument7 pages(Sample Format) For Livestock Raising Only - Hog Raising: Farm Plan and BudgetAlo RioNo ratings yet
- Incident Briefing ICS 201-1: 1. Incident/Event Name 2. Date Prepared 3. Time Prepared 4. Map SketchDocument6 pagesIncident Briefing ICS 201-1: 1. Incident/Event Name 2. Date Prepared 3. Time Prepared 4. Map SketchAlo RioNo ratings yet
- (Sample Format) Farm Plan and Budget For Crop Production OnlyDocument7 pages(Sample Format) Farm Plan and Budget For Crop Production OnlyAlo RioNo ratings yet
- (Sample Format) For Livestock Raising Only - Poultry: Farm Plan and BudgetDocument7 pages(Sample Format) For Livestock Raising Only - Poultry: Farm Plan and BudgetAlo RioNo ratings yet
- Farm Record: Super PremiumDocument3 pagesFarm Record: Super PremiumAlo RioNo ratings yet
- (VIDA Company Profile) This Is VIDA 202212Document26 pages(VIDA Company Profile) This Is VIDA 202212Artemis SimetraNo ratings yet
- Operators Manual: Doc #P10226 Rev 1.8Document32 pagesOperators Manual: Doc #P10226 Rev 1.8Christopher DaMatta BarbosaNo ratings yet
- KokkkDocument9 pagesKokkkhalewat AbebeNo ratings yet
- Double-Seat-Valves DSV-Complete Sudmo BrochureDocument16 pagesDouble-Seat-Valves DSV-Complete Sudmo BrochureHector Serrano MagañaNo ratings yet
- Survey Report On The Level of Preparedness of The CSS of Grade 11 Students For TESDA AssessmentDocument14 pagesSurvey Report On The Level of Preparedness of The CSS of Grade 11 Students For TESDA Assessmentsherry mae cordeta0% (1)
- Yealink W70B DECT IP Phone Release Notes of Version 85Document9 pagesYealink W70B DECT IP Phone Release Notes of Version 85tristan.zfrNo ratings yet
- Thomas JungDocument4 pagesThomas JungSubhadip Das SarmaNo ratings yet
- PSS Inv Manual 2020Document1,117 pagesPSS Inv Manual 2020ArifAzriNo ratings yet
- Predictive Maintenance (PDM) & Proactive Maintenance (Pam) : Dr. Khaleel AbushgairDocument22 pagesPredictive Maintenance (PDM) & Proactive Maintenance (Pam) : Dr. Khaleel AbushgairAbd Elrahman IssaNo ratings yet
- QW-QAL-626 - (Rev-00) - Prod. and QC Process Flow Chart - Ventura Motor No. 13 (35804)Document6 pagesQW-QAL-626 - (Rev-00) - Prod. and QC Process Flow Chart - Ventura Motor No. 13 (35804)Toso BatamNo ratings yet
- PWD ZP Wrd6000+ Previous - Year Mcqs With ExplanationDocument29 pagesPWD ZP Wrd6000+ Previous - Year Mcqs With ExplanationvishalNo ratings yet
- Computer Network, Unit 4Document20 pagesComputer Network, Unit 4shivaniNo ratings yet
- Aisc Standard HoleDocument2 pagesAisc Standard HoleMoe Oo HtunNo ratings yet
- Configuring Network ConnectivityDocument26 pagesConfiguring Network ConnectivityangelitoNo ratings yet
- Excel's Built-In FunctionsDocument21 pagesExcel's Built-In FunctionsJustin Aaron VirayNo ratings yet
- PD16B02HDocument4 pagesPD16B02HTravis HydzikNo ratings yet
- Annexure Step by Step Process Involved in The Ph.D. Semester RegistrationDocument1 pageAnnexure Step by Step Process Involved in The Ph.D. Semester RegistrationAnu GraphicsNo ratings yet
- Steam Turbines For CS PowerDocument6 pagesSteam Turbines For CS PowerPower PowerNo ratings yet
- What Is A Road MapDocument2 pagesWhat Is A Road MapShenivelChimChimNo ratings yet
- Audio Information and MediaDocument3 pagesAudio Information and MediaChia TanNo ratings yet
- S. No. Name Test/Lab Onsite DateDocument11 pagesS. No. Name Test/Lab Onsite Daterajat.telecomNo ratings yet
- Computers and Electronics in Agriculture: Konstantinos P. FerentinosDocument3 pagesComputers and Electronics in Agriculture: Konstantinos P. FerentinosCoffee pasteNo ratings yet
- PIX System Configuration enDocument32 pagesPIX System Configuration ensani priadiNo ratings yet