You might also like
- Antibiotic ConversionDocument9 pagesAntibiotic ConversionfabianNo ratings yet
- Paediatric DosesDocument2 pagesPaediatric DosesMichael AdjeiNo ratings yet
- Homeo Drug CompenDocument6 pagesHomeo Drug CompenSittie Nadia MangondatoNo ratings yet
- Antibiotic Treatment of Infection Due To Vibrio Vulnificus - UpToDateDocument2 pagesAntibiotic Treatment of Infection Due To Vibrio Vulnificus - UpToDateKevo VillagranNo ratings yet
- Pediatric Antibiotic DosingDocument7 pagesPediatric Antibiotic DosingAnonymous mm1yTelKNo ratings yet
- Drug Dosages in PediatricsDocument4 pagesDrug Dosages in Pediatricsmarry.as2012No ratings yet
- Dr. Ave - Anti ParasitesDocument44 pagesDr. Ave - Anti ParasitesDeanGrestamaNo ratings yet
- Finasteride: Analgesics (Non-Opioid) & AntipyreticsDocument5 pagesFinasteride: Analgesics (Non-Opioid) & AntipyreticsSarah Michelle NiduaNo ratings yet
- Nidua's Drug ChartDocument5 pagesNidua's Drug ChartSarah Michelle NiduaNo ratings yet
- Articol Engleza-1Document7 pagesArticol Engleza-1Miruna MiulescuNo ratings yet
- Pediatric DosesDocument5 pagesPediatric Dosesa2r91No ratings yet
- Degracia, John Noeh D. Drug StudyDocument15 pagesDegracia, John Noeh D. Drug StudyLenie DegraciaNo ratings yet
- Ivf: Therapeutics: Anti-Pyretics: PenicillinsDocument6 pagesIvf: Therapeutics: Anti-Pyretics: PenicillinsJenny CiNo ratings yet
- FormularyDocument5 pagesFormularyMichelle WongNo ratings yet
- Calpol Tablets Oral Suspension and Paediatric DropsDocument15 pagesCalpol Tablets Oral Suspension and Paediatric DropsAndrew PartridgeNo ratings yet
- FormulaDocument5 pagesFormulaEloiseBalasbasNo ratings yet
- Measles PHIDSPILDocument5 pagesMeasles PHIDSPILriczen mae vilaNo ratings yet
- Theraputic Agent in NeonateDocument7 pagesTheraputic Agent in Neonateد. محمد فريد الغنامNo ratings yet
- Analgesik/Pire Tik Dosis Sediaan Obat DOA OOA Drug Interaction Paracetamol IVDocument9 pagesAnalgesik/Pire Tik Dosis Sediaan Obat DOA OOA Drug Interaction Paracetamol IVNicole NgoNo ratings yet
- Amoxicillin 250 MG Capsules-Summary of Product CharacteristicsDocument65 pagesAmoxicillin 250 MG Capsules-Summary of Product CharacteristicsBrown and Burk UK Ltd100% (1)
- Route/Dosage: Concentration: Not To Exceed 10 Mg/ml. Do NotDocument2 pagesRoute/Dosage: Concentration: Not To Exceed 10 Mg/ml. Do NotMaria MargaritaNo ratings yet
- 05 Pharmacology PLE 2019 RatioDocument50 pages05 Pharmacology PLE 2019 RatioPatricia VillegasNo ratings yet
- INDICATIONS and ContraindicationsDocument2 pagesINDICATIONS and ContraindicationsKat SimmonsNo ratings yet
- Obat Dosis Obat: Pneumonia, Community-AcquiredDocument2 pagesObat Dosis Obat: Pneumonia, Community-Acquiredannisa shalihahNo ratings yet
- Dr. Anati Purwakanthi, MSC Departemen Farmakologi Fkik UnjaDocument40 pagesDr. Anati Purwakanthi, MSC Departemen Farmakologi Fkik Unjaanes tiraNo ratings yet
- Klasifikasi Nama Obat Kisaran Dosis Dan Dosis Maksimal/Hari Dewasa Anak Oral (MG) Iv/ Im Oral (MG/KG) Iv/ImDocument2 pagesKlasifikasi Nama Obat Kisaran Dosis Dan Dosis Maksimal/Hari Dewasa Anak Oral (MG) Iv/ Im Oral (MG/KG) Iv/ImKhairul AlvaroNo ratings yet
- NICU Drugs GuideDocument49 pagesNICU Drugs GuideArhanNo ratings yet
- Id 397 TeicoplaninDocument2 pagesId 397 TeicoplaninStacey WoodsNo ratings yet
- MPC Antidote ChartDocument1 pageMPC Antidote Chartogodothomas51No ratings yet
- Drug Choice For OmaDocument1 pageDrug Choice For Omapriskilas911No ratings yet
- Pediatric Drug Dosage - All in One PDFDocument15 pagesPediatric Drug Dosage - All in One PDFHuang Hasjim33% (9)
- Wound Infections: Common PathogensDocument1 pageWound Infections: Common PathogensAnonymous KGxzow5zxhNo ratings yet
- AntibiocardDocument25 pagesAntibiocardchildicuNo ratings yet
- Pediatic DosesDocument8 pagesPediatic Doseshailemariamgebrehiwot02No ratings yet
- Lampiran OM & FaringitisDocument6 pagesLampiran OM & FaringitisAdhinyDistiHelmiNo ratings yet
- Amoxicillin 125 MG 250 MG 5 ML Oral SuspensionDocument16 pagesAmoxicillin 125 MG 250 MG 5 ML Oral SuspensionAshrafNo ratings yet
- Levetiracetam Brand Indication Dosage Form Cost/Packing: Adult and Adolescent 16 Years 500mg BIDDocument4 pagesLevetiracetam Brand Indication Dosage Form Cost/Packing: Adult and Adolescent 16 Years 500mg BIDMark PradsNo ratings yet
- Effect DoseDocument30 pagesEffect DoseXyprus Darina VeloriaNo ratings yet
- Recommended Doses of Medications To Treat Children With An Acute Asthma ExacerbaDocument3 pagesRecommended Doses of Medications To Treat Children With An Acute Asthma Exacerbaمعاذ الشريفNo ratings yet
- Tamiflu Epar Product Information - enDocument118 pagesTamiflu Epar Product Information - enUmar AliNo ratings yet
- Acyclovir (Systemic) - Pediatric Drug Information - UpToDate PDFDocument34 pagesAcyclovir (Systemic) - Pediatric Drug Information - UpToDate PDFAndreea LupuNo ratings yet
- Common Pediatric MedicationsDocument1 pageCommon Pediatric MedicationsMilito KikamNo ratings yet
- Cilastati Imipenem Drug InfoDocument19 pagesCilastati Imipenem Drug InfoCosmina GeorgianaNo ratings yet
- Kumpulan Daftar ObatDocument6 pagesKumpulan Daftar ObatZega AgustianNo ratings yet
- CLACIDODocument22 pagesCLACIDOSergel CapsuleNo ratings yet
- Amoxicillin - Drug Information - UpToDateDocument47 pagesAmoxicillin - Drug Information - UpToDateMikaela lNo ratings yet
- Peptic Ulcer Disease DrugsDocument6 pagesPeptic Ulcer Disease DrugsApple MaeNo ratings yet
- Paediatric Dosage of Some Drugs-1Document45 pagesPaediatric Dosage of Some Drugs-1JaneNo ratings yet
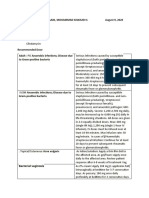
- D-6-12 Sanaani, Mohammad Khaisar H. August 9, 2020: Bacterial VaginosisDocument4 pagesD-6-12 Sanaani, Mohammad Khaisar H. August 9, 2020: Bacterial VaginosisKenMNo ratings yet
- Gentamycin Case Notes by SDocument3 pagesGentamycin Case Notes by SSharan SahotaNo ratings yet
- Antibiotic Guidelines For PediatricsDocument33 pagesAntibiotic Guidelines For PediatricsVarshini Tamil SelvanNo ratings yet
- CommedDocument3 pagesCommedFatee Kasim McrngnNo ratings yet
- Endometrialcarcinoma r0416 7941Document2 pagesEndometrialcarcinoma r0416 7941crisibarra911No ratings yet
- ANTIBIOTICSDocument51 pagesANTIBIOTICSamrharidi446No ratings yet
- Drugs For Paediatric UseDocument14 pagesDrugs For Paediatric Usefouza100% (1)
- Azithromycin Monograph - PaediatricDocument7 pagesAzithromycin Monograph - PaediatrictynNo ratings yet
- Drugs For Treatment of PCPDocument5 pagesDrugs For Treatment of PCPwennyoktavNo ratings yet
- (According To Alphabetical Order) : Community Acquired Meningitis (CAM)Document69 pages(According To Alphabetical Order) : Community Acquired Meningitis (CAM)Nuhiat NahreenNo ratings yet
- Concise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryFrom EverandConcise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryNo ratings yet
- Pharmacy Calculation Workbook: 250 Questions to Prepare for the NAPLEX and PTCB ExamFrom EverandPharmacy Calculation Workbook: 250 Questions to Prepare for the NAPLEX and PTCB ExamRating: 5 out of 5 stars5/5 (1)
- Drugs Associated With Isolated ThrombocytopeniaDocument4 pagesDrugs Associated With Isolated ThrombocytopeniaKhor Chin PooNo ratings yet
- Antibiotic Renal DoseDocument13 pagesAntibiotic Renal DoseKhor Chin PooNo ratings yet
- AntifungalDocument7 pagesAntifungalKhor Chin PooNo ratings yet
- Metabolic Consequences Different Perioperative Fluid Therapies in The Neonatal PeriodDocument6 pagesMetabolic Consequences Different Perioperative Fluid Therapies in The Neonatal PeriodKhor Chin PooNo ratings yet
- 501 1765 1 PBDocument7 pages501 1765 1 PBKhor Chin PooNo ratings yet
- A Systematic Review of Practice Surveys On Parenteral Nutrition For Preterm InfantsDocument5 pagesA Systematic Review of Practice Surveys On Parenteral Nutrition For Preterm InfantsKhor Chin PooNo ratings yet
- 47 TPNDocument7 pages47 TPNKhor Chin PooNo ratings yet
- Aminoglycoside & VancomycinDocument10 pagesAminoglycoside & VancomycinKhor Chin PooNo ratings yet
- 430 FullDocument6 pages430 FullKhor Chin PooNo ratings yet
- FDA Approves First Gene Therapy, Betibeglogene Autotemcel (Zynteglo), For Beta-ThalassemiaDocument3 pagesFDA Approves First Gene Therapy, Betibeglogene Autotemcel (Zynteglo), For Beta-ThalassemiaGiorgi PopiashviliNo ratings yet
- German Atv-Dvwk Rules and StandardsDocument25 pagesGerman Atv-Dvwk Rules and StandardsMehmet Emre Bastopcu100% (1)
- Business Plan 3.3Document2 pagesBusiness Plan 3.3Rojin TingabngabNo ratings yet
- The Magic DrumDocument185 pagesThe Magic Drumtanishgiri2012No ratings yet
- Origami Oso HormigueroDocument9 pagesOrigami Oso HormigueroRogelio CerdaNo ratings yet
- SimovertDocument41 pagesSimovertRamez YassaNo ratings yet
- Broken BondsDocument20 pagesBroken Bondsapi-316744816No ratings yet
- UTP Student Industrial ReportDocument50 pagesUTP Student Industrial ReportAnwar HalimNo ratings yet
- Project Scheduling and TrackingDocument47 pagesProject Scheduling and TrackingArun VinodhNo ratings yet
- ME Eng 8 Q1 0101 - SG - African History and LiteratureDocument13 pagesME Eng 8 Q1 0101 - SG - African History and Literaturerosary bersanoNo ratings yet
- Appendix - Pcmc2Document8 pagesAppendix - Pcmc2Siva PNo ratings yet
- ReadmeDocument3 pagesReadmedhgdhdjhsNo ratings yet
- Project - New Restuarant Management System The Grill HouseDocument24 pagesProject - New Restuarant Management System The Grill HouseMayank Mahajan100% (3)
- Presentation 11Document14 pagesPresentation 11stellabrown535No ratings yet
- Objective & Scope of ProjectDocument8 pagesObjective & Scope of ProjectPraveen SehgalNo ratings yet
- PLC Laboratory Activity 2Document3 pagesPLC Laboratory Activity 2Kate AlindajaoNo ratings yet
- Ron Kangas - IoanDocument11 pagesRon Kangas - IoanBogdan SoptereanNo ratings yet
- Revenue and Expenditure AuditDocument38 pagesRevenue and Expenditure AuditPavitra MohanNo ratings yet
- Carriage RequirementsDocument63 pagesCarriage RequirementsFred GrosfilerNo ratings yet
- Rule 113 114Document7 pagesRule 113 114Shaila GonzalesNo ratings yet
- C C C C: "P P P P PDocument25 pagesC C C C: "P P P P PShalu Dua KatyalNo ratings yet
- Unit 16 - Monitoring, Review and Audit by Allan WatsonDocument29 pagesUnit 16 - Monitoring, Review and Audit by Allan WatsonLuqman OsmanNo ratings yet
- Tetralogy of FallotDocument8 pagesTetralogy of FallotHillary Faye FernandezNo ratings yet
- g6 - AFA - Q1 - Module 6 - Week 6 FOR TEACHERDocument23 pagesg6 - AFA - Q1 - Module 6 - Week 6 FOR TEACHERPrincess Nicole LugtuNo ratings yet
- Service Manual: SV01-NHX40AX03-01E NHX4000 MSX-853 Axis Adjustment Procedure of Z-Axis Zero Return PositionDocument5 pagesService Manual: SV01-NHX40AX03-01E NHX4000 MSX-853 Axis Adjustment Procedure of Z-Axis Zero Return Positionmahdi elmay100% (3)
- Mcom Sem 4 Project FinalDocument70 pagesMcom Sem 4 Project Finallaxmi iyer75% (4)
- Ito Na Talaga Yung FinalDocument22 pagesIto Na Talaga Yung FinalJonas Gian Miguel MadarangNo ratings yet
- C - Amarjit Singh So Bhura SinghDocument5 pagesC - Amarjit Singh So Bhura SinghRohit JindalNo ratings yet
- B. Geoinformatics PDFDocument77 pagesB. Geoinformatics PDFmchakra720% (1)
- RSA - Brand - Guidelines - 2019 2Document79 pagesRSA - Brand - Guidelines - 2019 2Gigi's DelightNo ratings yet