Pearson Edexcel International GCSE
(9-1) Business Student Book - eBook
Visit to download the full and correct content document:
https://ebooksecure.com/download/pearson-edexcel-international-gcse-9-1-business-
student-book-ebook-pdf/
Another random document with
no related content on Scribd:
“Still, we must remember how singularly, of late years, the knowledge of the
introduction of cholera by persons coming from infected districts has increased, and
how very striking are the instances of this kind already recorded in several works on
influenza.
“In some cases, again, isolation or seclusion of a community, as in prisons, has given
immunity; or at least that community has not been attacked.”
The great rapidity of spread has caused even in 1918 some temporary doubt as to the
contagiousness of the disease. Thus, Zinsser wrote:
“The opinion of direct and indirect transmission from man to man is also well
supported by a detailed study of the epidemiology of individual outbreaks. In our own
experience with epidemics such as those at Chaumont, Baccarat and other places, the
suddenness with which the malady attacked large numbers of people at almost one and
the same time, caused me at first to be exceedingly skeptical of accepting transmission
by contact as the only means of conveyance. We considered food and insect transmission
as possibilities, and tried our best to find grounds for involving such agencies. But in
every case we were forced to return to the conclusion that direct and indirect contact
between men came nearest to doing justice to all observed facts.”
There have been many examples reported from personal experience to show that
influenza is transmitted from man to man. Two objections, however, have had to be met,
before this view was generally accepted. First, it has been claimed by some that the
disease spread more rapidly from an assumed focus than individuals could travel, and
second, that instances were on record of cases occurring spontaneously in isolated
communities. Yet a third argument formerly raised against the contagious character of
the disease was the claim that it broke out in mass attacks, that large numbers became ill
on the same day without the occurrence of isolated antecedent cases. The splendid work
of epidemiologists following the 1889 epidemic appears to have answered all of these
objections. Many, such as Leichtenstern, have gone into great detail on this subject. In
fact, at that time this was the question of greatest importance. Today we assume the
correctness of the hypothesis, and pass on to consideration of other subjects of more
recent development. We will, therefore, review very hurriedly some of the evidence
quoted to prove that influenza is transmitted only from man to man and only by human
intercourse.
Isolated places.—Has it ever been shown that individuals completely isolated from
communication with communities where influenza is present have, during an epidemic,
developed the disease? Leichtenstern, after a comprehensive review, concludes as
follows: “We have not a single example on record where influenza has attacked
individuals in completely isolated localities, as on mountain tops and mountain passes.
Study of this has been undertaken in Switzerland by F. Schmid. The same has been true
of ships at sea, as has been shown chiefly from the English Marine Reports. There have
been reports of influenza occurring in mid-ocean and particularly in the earlier
epidemics, but the information has been insufficient.”
Parkes at even an earlier period observed: “I cannot but consider that we require
better evidence of ships being attacked in mid-ocean. In some of the quoted instances
the ships had been at a port either known to be infected or in which influenza was really
present, although it had not become epidemic. As we are ignorant of the exact period of
incubation some men may have been infected before sailing.”
Critical investigation into stories of spontaneous infection in isolated localities such as
ships at sea and island lighthouses will quite invariably demonstrate that these popular
reports have been distortions of the actual facts. One or two examples will suffice.
Abbott records an example: “An impression having gained some credence that influenza
had appeared on board the squadron of naval vessels which sailed from Boston in
December, 1889, while on their course across the Atlantic and before their arrival in
Europe, a letter was addressed by the writer to the Bureau of Medicine and Surgery of
the United States Navy for information upon this point, to which a reply was received, as
follows:
“The ‘Chicago,’ ‘Boston,’ ‘Atlanta’ and ‘Yorktown’ left Boston December 7, 1889, for
Lisbon, Portugal. The first three arrived at Lisbon on December 21st without having
touched at any port en route. The ‘Yorktown’ arrived at that port December 23d, having,
stopped about twenty-four hours at Fayal, Azores.... Influenza first appeared on the
‘Chicago’ December 23d, on the ‘Boston’ December 28th, on the ‘Atlanta’ December
30th and on the ‘Yorktown’ December 28th.
“Influenza was prevailing in Lisbon at the date of arrival of the squadron.”
In March, 1920, the author was notified of a somewhat similar story which he
undertook to trace. The results show well the inaccuracy of verbal transmission through
several individuals. A letter was first sent to the Quarantine Officer at Portland, Maine:
“It has been reported to us that in a lighthouse just outside of Portland, Maine, there has
been a rather interesting prank played by influenza. We are told that three men and one
woman live in the lighthouse; that during the 1918 influenza epidemic the woman
contracted the disease while none of the men became sick, and that in the present
epidemic all three of the men became sick with the disease and the woman remained
well. It was claimed that they had had no communication with the mainland for some
time before the men became ill,” etc.
The reply was as follows: “I have inquired of the Light House Inspector’s office in
Portland and they know of no stations to which the terms of your inquiry would apply.
“At the Boon Island station, there are three keepers with families. At the Half Way
Rock station, there are three keepers but no woman. The Inspector does not seem to
know of any station where there are three men and one woman.”
A second letter, sent to the Inspector of Lighthouses at Portland brought corroborative
information:
“The Boon Island Light Station was stricken by this epidemic in the following manner:
The keeper, his wife and five children were all stricken, the keeper himself having had
the hardest battle, having apparently been subject to same while ashore in Portsmouth,
N. H. after provisions, supplies, etc. The 2d assistant’s wife and two children were also
stricken, but the 2d assistant, himself, and the 1st assistant keeper did not contract the
malady in spite of the fact that they were all confined on a small island working together
at the station.
“During the year 1920 none of the keepers or their families, consisting of thirteen in
number, were affected. The Halfway Rock Light Station where three keepers are
employed did not contract this malady either in the years 1918 or 1920.
“For your information I might add that during the inspection trip in the months of
January, February and March, 1920, all of the light stations in this district were visited,
and it was found that they were all enjoying good health and had not been visited by the
epidemic, with the possible exception of three stations which are located either on the
mainland or close to where the keeper or his family were able to visit the nearby cities or
towns.”
Although it has not been shown that completely isolated places have been visited by
the disease, there is abundant evidence that such places have remained influenza free as
long as the isolation has remained complete. Islands and lighthouses, which have not
been in communication with the mainland, individuals living isolated on mountain tops,
and ships at sea remained free from influenza even in the presence of a pandemic, as
long as they did not come into communication with individuals sick with the disease.
The following places remained free from influenza throughout the 1889 epidemic: the
Isle of Man, several of the islands of the West Indies, particularly the Bahamas, Granada
and St. Lucia, also the British Honduras, British Guiana, and the Seychelle Islands.
Even in 1918, when the paths of commerce reached nearly every portion of the world,
we have examples of relative immunity of isolated places. Thus we know that the
Esquimaux were attacked late in the course of the pandemic, and we have the statement
of Barthélemy who traveled in 1919 to some of the oasis towns of the Sahara Desert, and
there discovered that there had not only been no influenza up to that time, but also that
they had not even heard of the pandemic.
Another type of isolated place is the closed institution. As early as 1709, Lancisi
remarked that the prisons of the Inquisition in Rome remained free from influenza.
Twenty-one prisons in Germany in 1889–90 remained entirely free from the disease.
This was true of 39 prisons in England, some of which were in cities where the epidemic
was most extensive. Linroth, who observed this same phenomenon in Sweden, makes
the wise remark that, “the influenza conquers more easily the space of 500 to 1,000
kilometers than it does the small barrier made by a prison wall.” A convent in
Charlottenburg housing one hundred women remained entirely free during the 1889–90
epidemic.
As a rule institutions of this sort have been unable to maintain a complete quarantine
throughout the period of an epidemic, and the relative immunity has been demonstrated
more in late invasions, at a time when the restrictions have become somewhat lax. Thus,
in 1918, Winslow and Rogers, report that in an orphan asylum in New Haven,
Connecticut, which had completely escaped during the month of October when the
epidemic was at its height, one of the Sisters and the priest in charge came down with
influenza about December 15th. By the 27th of December 127 cases had occurred in the
institution within twenty-four hours, and by January 7th there had been 424 cases, with
seven deaths out of a total population of 464. The probable source of the sudden
outbreak of December 27th seems to have been the Sister first affected who, when
convalescent, resumed her duties in the kitchen, which included the inspection and
handling of the milk given out to the children.
Crowd gatherings.—Yet another phenomenon which would lead us to conclude that
human intercourse is the most potent factor in the transmission of influenza is the fact
that there is frequently a high increase in the influenza rate following crowd gatherings.
Parkes observed long ago that persons in overcrowded habitations, particularly in some
epidemics, suffered especially, and several instances are on record of a large school or a
barracks being first attacked and the disease prevailing there for some days, before it
became prevalent in the towns around.
In England, the weekly market played an important role in the spread of the disease in
1889. One frequently saw such reports as that: “The first case of influenza was a man
who went to London daily.” Or, “All the earliest cases were men going to London daily,
while their wives and families were later affected.”
In the epidemics at San Quentin Prison, it was noted that apices of incidence usually
occurred on Tuesday and Wednesday. During the first epidemic it was these days of the
second and third weeks. Stanley sees a direct connection between this fact and the fact
that every Sunday morning large groups of the men were crowded together in a
comparatively small auditorium where they saw moving pictures. On Sunday, October
20th, they sought to eliminate this source of spread by having a band concert in the open
air, but the prisoners crowded around the band and were loud in their cheers, and on the
following day there was a large increase in hospital admissions.
On November 24th after the second epidemic had apparently ceased the picture
shows were again started after having been closed for over six weeks. The following
Tuesday and Wednesday twenty-four well defined new cases were admitted to the
hospital. On Thanksgiving Day there was a field meet between the various departments
of the prison. About 200 prisoners took active part, while 1,600 prisoners were
spectators. The meet was held in the open air, but the prisoners were closely packed and
they cheered and yelled. For the three days following this celebration there were 9, 5 and
8 patients admitted respectively.
In discussing the recrudescence of influenza in Boston in November and December,
Woodward remarks as follows:
“Whether or not it may be more than a succession of coincidences it is certainly of
interest to note that the November outbreak of influenza showed itself three days after
the Peace Day celebration on November 12th, when the streets, eating places and public
conveyances were jammed with crowds; that the December epidemic began to manifest
itself after the Thanksgiving holiday, with its family re-unions and visiting; and that
reported cases mounted rapidly during the period of Christmas shopping, reaching a
maximum a week after the holiday.” That this may have been a coincidence is indicated
by the fact that, according to reports by Pearl and others this was not consistently true in
other large cities.
Dr. Meredith Davies records the case of a hostel in Wales accommodating 200
students. Infection was introduced on October 19th on the occasion of a dance attended
by some students from an infected institution in the neighborhood. Four cases occurred
on the 20th and within the short space of five days seventy-nine students out of the 200
were attacked.
Parsons found numerous similar examples in the epidemic of 1889. In 1918 it was
frequently observed that among American Soldiers in France, those troops quartered in
barracks suffered a much more rapid spread of the disease than those billetted out
among the houses of the towns.
Mass attack.—Another argument formerly raised against the contagious character
was the claim that it broke out in mass attack, and large numbers became ill on the same
day without the occurrence of isolated antecedent cases. The first cases of such epidemic
diseases as the plague and small pox became a matter of record because of the
accompanying high mortality, while in influenza, with its relatively low death rate the
record usually begins only after a comparatively large mass of individuals have been
attacked.
Watson in 1847 observed as follows: “Although the general descent of the malady is,
as I have said, very sudden and diffused, scattered cases of it, like the first droppings of a
thunder shower, have usually been remembered as having preceded it. The disorder is
most violent at the commencement of the visitation; then its severity abates; and the
epidemic is mostly over in about six weeks. Yet the morbific influence would seem to
have a longer duration. In a given place nearly all the inhabitants who are susceptible of
the distemper suffer it within that period, or become proof against its power. But
strangers, who, after that period, arrive from uninfected places have not, apparently, the
same immunity.”
Parkes in 1876 observed that, “When the disease enters a town it has occasionally
attacked numbers of the inhabitants almost simultaneously. But more frequently its
course is somewhat slower; it attacks a few families first and then in a few days rapidly
spreads; the accounts of thousands of persons being at once attacked at the onset of the
disease are chiefly taken from the older records, in which the suddenness of the
outbreak is exaggerated. Frequently, perhaps always, in a great city the outbreak is made
up by a number of localized attacks, certain streets or districts being more affected than
others, or being for a time solely affected, and in this way it successively passes to
different parts of the city. It has generally occurred in a great city before appearing in the
smaller towns and villages round it and sometimes these towns, though in the
neighborhood, have not been invaded for some weeks.
“In some cases and perhaps a large number, it breaks out after persons ill with
influenza have arrived from infected places.
“The decline in any great town is less rapid than its rise, and usually occupies from
four to six weeks, or sometimes longer.”
Detailed studies of the Munich epidemic of 1889 and numerous similar studies of the
recent epidemic, which will be referred to later, have shown a period of two or three
weeks of steadily increasing numbers of cases before the height of the epidemic was
reached.
Droplet infection and spread through inanimate objects.—The actual mode of spread
of the virus of influenza from one individual to another is unknown. The more generally
accepted explanation is that the infecting agent leaves the body through the respiratory
tract, usually in the spray of coughing or talking; contagion is by droplet infection, as is
sometimes the case in other respiratory infections. Thorne and others have called
attention to the capillary congestion of the conjunctivae very early in the disease. They
suggest that possibly the mucous membrane of the eye is the site of infection.
There has recently been considerable discussion concerning the spread of influenza
through inanimate objects.
Leichtenstern reviews the reports of 1889–93 in which influenza was supposed to
have been transmitted through wares, merchandise and other inanimate objects. He
concluded that the evidence in all of the cases cited was insufficient for conclusive proof.
Such an example was the supposed importation of the disease in goods sent from Russia
to the Grands Magazins du Louvre at Paris. In one day 100 people became ill and in a
few more 500 were sick with influenza. The explanation was that the germs had been
imported in goods sent from Russia to the store. Detailed investigation showed that this
could not have been the case because no goods had been received from Russia for a
period of three years. Another example is that of one of the two winter caretakers at the
St. Gothard Hospice. One of the two men went down into the valley where he purchased
supplies. Ten days after his return the man who had remained in the Hospice fell ill with
influenza while his comrade remained well. It was stated that influenza was introduced
into Basel by goods shipped to that place from the Magazins du Louvre in Paris. The first
case occurred in a man who had been working at unpacking these goods.
Lynch and Cumming believe that droplet infection plays but a minor role in the
spread of sputum-borne diseases, but that insanitary methods of washing dishes and
eating utensils was the chief cause for the high rates of “sputum-borne” infections both
in army and civilian life in 1918. They found that among 31,000 troops eating from
tableware which was cleaned by kitchen police, the influenza rate was 51 per 1,000,
while among 35,000 eating from mess kits which each individual washed himself the
rate was 252 per 1,000. “Eighty-four per cent. of the cases occurred among those whose
hands were contaminated by washing their own eating utensils.”
Among 17,236 employees of hotels, restaurants and department stores, who ate from
machine washed dishes, there occurred 349 cases of influenza, while among 4,175 who
ate from hand washed dishes there were 429 cases. The rate was but 20 per 1,000 in the
former, while in the latter group it reached 103 per 1,000. Here again the chances of
infection between the two groups were as one is to five.
These authors have records covering 252,186 individuals in scattered institutions in
the United States. Among those eating from machine washed dishes the rate was 108 per
1,000 while those eating from hand washed dishes suffered at the rate of 324 per 1,000.
The ratio was 1 to 3 between the two groups. Seventy-five per cent. of the cases occurred
in that group which ate from dishes not disinfected with boiling water. They do not state
the number of individuals in each of the two groups.
Lynch and Cumming claim that in the act of coughing only a few organisms are
expelled from the mouth, rarely over 1,500, and conclude that transmission by direct
contact through the air route but rarely, if ever, takes place. While about 1,500
organisms are expelled onto the floor by an act of coughing, a sterile glove wiped across
the lips may pick up nearly 2,000,000 organisms. Such organisms may be readily
transferred to inanimate objects which are handled by many people.
Hemolytic streptococci and pneumococci may be isolated with great regularity from
the hands of carriers or patients, from table ware, inanimate objects touched by these
patients, and from floor dust. Diphtheria and tubercle bacilli have been isolated from the
hands and eating utensils of patients. The average count of a large number of restaurant
dishwater specimens was 4,000,000 bacteria per c.c. The temperature of this water
averaged 43° C. and the dishes were practically never scalded. The water was often so
highly polluted, “that the dishes are more highly contaminated after they are washed
than before washing begins. The spoon or fork is often freer from organisms just after
being used by the restaurant patron than when taken from the restaurant’s polluted dish
water.”
Major John S. Billings, epidemiologist at Camp Custer, reported that one of the larger
organizations did not properly observe the regulation requiring that all mess kits and
table equipment be properly sterilized. The disease appeared early and spread unusually
rapidly in this particular organization.
In summarizing the subject of transmission through utensils, we may say that the
evidence is suggestive but inconclusive. It is possible, even probable, that this is one
mode of transmission. That it is the most important has not been proved. Lynch and
Cumming do not take into consideration that the regiments with more sanitary methods
of cleansing the dishes are apt to be those regiments with more sanitary habits
throughout their daily routine. Those restaurants using mechanical dish washers are
usually the cleaner restaurants.
Pontano in Italy is quoted by the Office International d’Hygiène Publique as having
observed in his epidemiological study that there was a constant connection between the
living conditions and the severity of the complications. Notable differences were
observed in neighboring houses according to the hygienic conditions of the various
households.
Healthy carriers and convalescents.—Leichtenstern, who apparently accepted the
Pfeiffer bacillus as the cause of influenza, did not believe that the disease could be
transmitted by healthy carriers. He based this assumption on the statement, made by
Pfeiffer, that the influenza bacillus was only found in acute influenza cases. In the past
few years it has been abundantly shown, however, that the influenza bacillus can and
does exist on the mucous membranes of healthy individuals.
The outbreak in an orphan asylum in New Haven has been previously described.
There the probable source of the sharp outbreak of December 27th seemed to be the
sister who, on convalescence, resumed her duties in the kitchen. There she inspected
and handled the milk served to the children. This suggests the possibility of infection
being propagated by convalescents and by food.
At present we do not know whether or not a patient remains infectious after the acute
symptoms have subsided; we are ignorant as to whether a convalescent patient can
transmit the disease; and we are not certain whether the organism found in healthy
carriers is virulent or not. The information at hand strongly indicates that apparently
healthy individuals may transmit the infection, but the wide distribution of the disease,
with multiple possible sources of infection for each individual, and the relative
insusceptibility of experimentally exposed individuals has made it impossible so far to
answer these questions satisfactorily.
General Manner of Spread in Individual Localities.
Having discussed the mode of propagation of influenza among individuals we will
follow the disease as it attacks one person after another in a community and study the
epidemiologic picture, drawn no longer with the individual as a unit, but with the
community as the unit.
We must here distinguish between a primary epidemic, the first wave of a progressing
pandemic, and the secondary type in which may be grouped those large or small
recurrences which light up for a period of one to three or more years after the primary
wave.
Primary type of epidemic.—One of the first important statistical studies on this
subject was that of P. Friedrich who charted the influenza morbidity in Munich between
the months of December, 1889, and February, 1890. Similar observations have been
made by Parsons, Raats, Linroth, and H. Schmid, following the 1889 epidemic.
Between the occurrence of the first known case of influenza and the time of the first
very definite increase in influenza incidence in a community, which interval may be
termed the invasion period, there is as a rule two weeks. During this period, of course,
more and more cases are occurring, but remain usually sufficiently isolated to attract no
public notice. From this point the epidemic develops very rapidly and reaches its peak,
usually within two or at most three weeks. In another two or three weeks the incidence
has fallen away nearly to normal. The epidemic period comprises from four to six weeks,
or, including the invasion period, an entire duration of six to eight weeks. This is the
picture produced in a community by a primary uncomplicated epidemic of influenza.
Greenwood well describes the salient features of a primary epidemic as “first a rapid and
quasi-symmetrical evolution, and second, a frequency closely concentrated around the
maximum.” In other words the duration is short, the rise to a peak rapid, and the
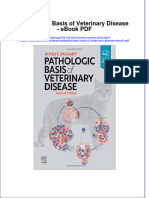
subsequent fall equally rapid. He showed that in the July and August, 1918 epidemic in
Great Britain nearly 80 per cent. of the total incidence in the localities studied was
grouped within three weeks time. His curve corresponds so well with that of the Munich
epidemic that he is able to superimpose them (Chart I). The rapid rise to a peak, almost
explosive in character, more characteristic of this disease than of any other, is to be
explained by the high degree of invasiveness of the organism, by the short period of
incubation, by the fact that many of the sick continue at their work, thus spreading the
disease, and by the non-immunity of large masses of people, together with the fact that
the transmission of a respiratory infection is accomplished much more easily than is any
other type of infection.
The author holds that the infrequency of immunity is a most important factor in the
production of this type of outbreak. The mode of transmission of influenza is the same
as that of other respiratory diseases. The infectivity is probably no greater than that of
measles, although that indeed is relatively great. The means of transmission are
presumably the same in each. Were we able to develop an immunity for influenza of as
high degree and permanence as we possess against measles, pandemics of influenza
would disappear. We wish to emphasize that the primary type of curve is a phenomenon
not peculiar to influenza, but that under certain circumstances it may be found in other
infectious diseases, and that it would be found more frequently in the other diseases if
the immunity developed against them was of as short duration as it appears to be
against influenza. If, for example, measles were to break out in a large group of
individuals, none of whom had had the disease, the type of curve would be the same. We
will produce evidence supporting our theory under another subject. Of course, other
factors such as short incubation period and unusual opportunities for spread through
mildly ill individuals play a not unimportant role.
CHART I.
The curves of incidence of influenza in
Munich, and of deaths in London during
the 1889 and subsequent epidemics.
(Greenwood.)
Secondary type of epidemic.—There is a decided difference
between the curve of a primary wave as it appears in the onward rush
of a new pandemic and that of a secondary wave occurring at a
greater or less interval following the primary spread. A secondary
epidemic affects, according to Greenwood, a relatively small
proportion of the population, is slower in reaching its maximum, and
thereafter declines slowly and irregularly, more slowly than it
increases. The distribution of the curve is less symmetrical and there
is less concentration around the maximum. A secondary epidemic
may be characterized by a much higher fatality than a primary one.
We believe that the configuration of a secondary type of wave is
due chiefly although not entirely to a certain degree of residual
immunity in a large number of individuals remaining from the first
spread. There is a striking similarity between Chart I and Chart
XXVIII, the latter showing the measles incidence in epidemics
among rural or chiefly non-immune troops in the United States
army. Chart XXIX shows a similar epidemic among urban or chiefly
immune individuals. Here the curves correspond more to those of a
secondary type of influenza epidemic. Thus we see that, in the
absence of immunity, other infectious diseases may produce the
primary type of curve, and that this curve is not a feature of influenza
alone.
A striking difference between the two types of waves of influenza is
the uniformity and relative constancy of the primary type as
contrasted to the great variation in the secondary type. The story of
the first spread of influenza in one community is usually similar to
that of its spread in any other community. Certain exceptions will be
alluded to later. But in the case of recurrent epidemics we may find
them more severe or much milder; we may find that they attack a
large number of individuals or a very few; we may even find an entire
absence of recurrent epidemics in certain communities. The primary
curves are relatively uniform; the secondary curves are variable.
Between 1889 and 1894 in England there were four epidemics. The
first was primary, symmetrical, and lasted between December and
February, 1889–90. The second was asymmetrical and much more
fatal in the localities studied by Greenwood. It occurred in the spring
and summer of 1891. There was a third epidemic in the autumn and
winter of 1891–92 and a fourth occurred from November, 1893 to
January, 1894. The third epidemic, according to Greenwood, showed
some tendency to revert to the primary type in respect to symmetry,
while the fatality rate partook of the character of a secondary
epidemic.
Creighton writes: “That which chiefly distinguishes the influenza
of the end of the nineteenth century from all other invasions of the
disease is the revival of the epidemic in three successive seasons, the
first recurrence having been more fatal than the original outbreak,
and the second recurrence more fatal (in London at least) than the
first. The closest scrutiny of the old records, including the series of
weekly bills of mortality issued by the parish clerks of London for
nearly two hundred years, discovers no such recurrences of influenza
on the great scale in successive seasons.”
Greenwood, who has studied this subject in great detail in
England, discusses Creighton’s remarks as follows: “He would be a
bold man who challenged the accuracy of Creighton upon a point of
historical scholarship, and I have only to suggest that there are faint
indications of increased mortality in years following primary
epidemics of influenza prior to the nineteenth century. Thus 1675
was a year of primary epidemic influenza, fully described in
Sydenham’s Observationes Medicae.
“The nature of the succeeding constitutions is not clear, but the
deaths ‘within the bills’ for 1676 were considerably more numerous
than in 1675, although smallpox, fever and ‘griping of the guts’ were
noticeably less fatal.
“In the English Responsoria (1, 54) the epidemic constitution of
1679 is described as a recurrence of that of 1675—that is, as having
the features of primary epidemic influenza. In the five following
years intermittents prevailed, and in one (1684) the mortality much
exceeded that of 1679, although the deaths from smallpox were
fewer. Again, a hundred years later, in 1782, there was a famous
summer epidemic of influenza in London which gave rise to much
discussion. The London mortalities in 1782 and 1783 were, however,
almost equal, when the smallpox deaths (which were nearly three
times as numerous in 1783 as in 1782) are subtracted from the total
mortality of each year.
“Whether these vague indications are sufficient to permit of our
thinking that the epidemic constitution of 1889–94 was not entirely
unprecedented is disputable. But the contrast of the latter period
with the preceding single epidemic of 1847–48 is striking; that was a
primary epidemic without important sequelae.
“We have now to consider whether our experience this year is
concordant with that of the early nineties, a reversion to the earlier
type, or a new phenomenon.”
After comparing the 1889 curves with those for the July, 1918,
outbreak in England, Greenwood concludes: “I believe that the
evidence just presented establishes a substantial identity between the
summer outbreak of 1918 and the primary wave of 1889–90. We do
not need to appeal to any new factor arising out of the war to account
for it.
“I next consider the secondary epidemic which we are now
experiencing (October, 1918). Evidently our knowledge of the events
in 1891 would lead us to feel no surprise at the emergence of a
secondary wave, although we could not be sure that the precedent of
1847 would not be followed.
“The summer epidemic of 1918 in the Royal Air Force included
nearly 80 per cent. of the total incidence within the three weeks
containing the maximum, and the Munich epidemic included just
over 80 per cent. within the same limits. Now if the current epidemic
has reached its maximum, not more than 65 per cent. of the
incidence will probably be so concentrated, and the duration will
therefore be longer than in the summer; if, as suggested by the ratio
of the last two ordinates, the maximum is not yet attained, then the
quota of the three first weeks is likely to be still smaller and the
complete duration still longer.
“The diagram of factory sickness leads to the same inference,
which is that, from the standpoint of prevalence, the present is a
typical secondary epidemic, congruent with that of 1891.
“It appears, then, that the origin of the summer epidemic must be
explained upon such epidemiological principles as will account for
the primary wave of 1889–90, that the current outbreak is in pari
materia with that of 1891, its excessive mortality being mainly due to
the accident of season, aided by the special circumstances of
overcrowding and fuel shortage which are due to the war. In a word,
this is not essentially a war epidemic.”
Wutzdorff found that in some towns, particularly in North
Germany, the 1891–1892 wave was almost as extensive as that of
1889–90 had been in other places, but that in general the morbidity
in Germany was much lower. He bases these conclusions on a study
of the extent of crowding in the hospitals in the two years, on
statistics of government physicians, etc.
In Europe the recurrent epidemics of 1891 increased as a rule very
gradually, developed slowly, reached their high point frequently after
many weeks, and as gradually decreased. The epidemic duration in
the winter of 1891–92 lasted four or five months. The morbidity in
spite of the longer duration was decidedly less. This is very different
from the explosive appearance of 1889 when the peak was reached in
fourteen days and the whole epidemic had been completed in six to
eight weeks. There were some exceptions to this rule, as in Yorkshire,
England, where the epidemic broke out suddenly between the 11th
and 13th of April, 1891, had reached its peak after ten days, and for
another twenty days declined. Especially interesting was Sheffield,
where the first spread began gradually and ran a slow course, while
the second epidemic of 1891 began explosively, lasted a short time
and declined rapidly, but showed a significantly greater mortality
than that of 1889.
The experiences in various communities in the United States have
been not unlike those described for European cities. Abbott in
describing the successive epidemics in Massachusetts remarked that
the 1889–90 spread manifested itself by a sudden rise in the
mortality from influenza and pneumonia, beginning about December
20th and culminating in the middle week of January, thereafter
falling off quite suddenly in February to about the usual rate for
these diseases. The second epidemic two years later began with a
more gradual rise in October and November and then increased
sharply in December, continued for nearly three weeks at its
maximum in January, and declined nearly as sharply as in the
previous epidemic two years before.
Winslow and Rogers who have studied the 1918 epidemic as it
affected the various towns of Connecticut observed that the outbreak
in a given community generally occupied a period of from six to eight
weeks, and was steep and abrupt in communities which were badly
hit, flatter and more gently sloping in those which escaped lightly.
Also the outbreak was more severe in communities receiving the
infection early than in those later affected.
Mortality curves.—Pearl has studied the epidemic constitution of
influenza in forty-two of the large cities of the United States. He has
plotted the annual death rate per 1,000 population from all causes in
each week, from the week ended July 6, 1918, up to January 1, 1919,
and observed a very distinct difference in the type of curve for deaths
from all causes during the epidemic period in the various cities.
These differences have been chiefly in respect to the severity and
suddenness with which they were attacked. Thus Albany, Boston,
Baltimore, Dayton and Philadelphia show an initial explosive
outbreak of great force, while Atlanta, Indianapolis, Grand Rapids,
Milwaukee and Minneapolis exhibit a much slower and milder
increase of the mortality rate. In Albany and Baltimore the curve of
the first epidemic outbreak rises to a peak and declines at about the
same rate. In Cleveland and St. Paul, on the other hand, the rate of
ascent to the peak is very rapid, while the decline is slow and long
drawn out.
Some of the cities, such as Albany, show but a single well defined
peak in the mortality curve. Others, such as Boston, New Orleans
and San Francisco show two peaks; while still others, like Louisville,
show three well marked peaks.
Usually the first was the highest and the second and third were
progressively lower. Milwaukee and St. Louis, on the other hand,
showed second peaks higher than the first. The usual phenomenon,
however, was a large first wave followed by smaller ones.
The highest, or maximum peak rate of mortality during the
epidemic varied greatly, from 31.6 per 1,000 in the case of Grand
Rapids, to 158.3 per 1,000 in the case of Philadelphia.
The death rates which were of the most frequent occurrence were,
generally speaking, rates below 70 per 1,000 per week.
The date of the week in which the maximum peak rate occurred
was earliest in Boston and Cambridge, where it occurred October
5th, and latest in Grand Rapids, Milwaukee and St. Louis (December
14th). Thirty-one of the 40 cities studied had attained the peak rate
of mortality prior to November 2d. In the case of Milwaukee and St.
Louis the maximum peak was the second peak, whereas in Grand
Rapids it was the first peak that was so late. Sixty-five per cent. of the
40 cities showed two distinct peaks in the mortality curve, while 15
per cent. had one peak, and 8 or 20 per cent. had three peaks.
“It appears clearly that there was a definite tendency for the two-
peak cities to fall into two groups in respect of the time elapsing
between first and second peaks. About a third of them had the
second mortality peak around eight weeks after the first peak. The
remaining two-thirds had the second peak, on the average, about
thirteen weeks after the first. The three-peak curves had the second
peak on an average 7.1 ± 0.3 weeks after the first, and the third peak
on an average 13.1 ± 0.3 weeks after the second. The cycle in the
epidemic waves would therefore appear to be nearly a multiple of
seven weeks rather than the ten weeks tentatively deduced from the
dates of peaks. There the process of averaging obscured the true
relations.”
Duration of explosive outbreak.—The range of the duration of the
first outbreak of epidemic mortality is great, varying from five weeks
in Richmond, Virginia, to twenty-three weeks in Atlanta, Georgia.
Twenty of the cities, one-half the total number, showed a duration of
ten weeks or less, while in the other half the duration was eleven
weeks or more. The mean duration of epidemic mortality in the first
outbreak was 11.90 ± 0.55 weeks. The ascending limb of mortality
rate was rapid in nearly all cities. The descending limb was usually
slower. In 34 of the 40 cities it required four weeks or less time for
the mortality rate to pass from normal to its epidemic peak. But in
only half as many (17) of the cities did the rate come down from its
peak to normal again in a period of four weeks or less. The mean
time from normal mortality rate to peak was 3.90 ± 0.21 weeks. The
mean time from peak mortality rate to normal was 8.00 ± 0.50
weeks. Thus it took about twice as many weeks for the mortality
curve to come back from its peak to normal, as were required for the
increase from normal to peak at the beginning of the explosion. This
is on the average. The ascending limb occupied about a month and
the descending limb two months.
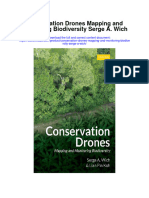
Pearl’s curves which have been copied in this report (Charts II to
VII) enable us to follow his conclusions. Pearl offers a partial
explanation for the variations in the different cities. There can be no
doubt but what many factors play a role in the causation of these
variations, and it is to be regretted that up to the present no statistics
for smaller, more homogeneous communities have as yet been
reported which could be compared with Pearl’s excellent work on the
large cities of the country. Were his work supplemented by records
from smaller towns in which the varying factors are less numerous,
in which there is less occupational variation, additional conclusions
could probably be reached. The unfortunate feature is that as a rule
statistics from the smaller cities and towns are less reliable.
From a detailed mathematical study of influenza in 39 of our
largest cities, done chiefly by the means of multiple correlation, with
the hope of being able to explain the differences in the epidemic
curves of weekly mortality in the various cities, Pearl concludes as
follows:
“The general conclusion to which we come from an examination of
the correlation data assembled to this point is that these four general
demographic factors, density of population, geographical position,
age distribution of population, and rate of recent growth in
population, have practically nothing to do, either severally or
collectively, with bringing about those differences between the
several cities in respect to explosiveness of the outbreak of epidemic
mortality in which we are interested. Significantly causal or
differentiating factors must be sought elsewhere.”
CHART II.
Death rates from all causes by weeks in
certain large cities of the United States
during the winter of 1918–19. (Pearl.)
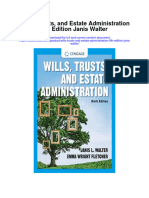
CHART III.
Death rates from all causes by weeks in
certain large cities of the United States
during the winter of 1918–19. (Pearl.)
CHART IV.
Death rates from all causes by weeks in
certain large cities of the United States
during the winter of 1918–19. (Pearl.)
You might also like
- The Spanish Influenza Pandemic of 1918: How the US Reacted: Efforts Made to Combat and Subdue the Disease in Luzerne County, PennsylvaniaFrom EverandThe Spanish Influenza Pandemic of 1918: How the US Reacted: Efforts Made to Combat and Subdue the Disease in Luzerne County, PennsylvaniaNo ratings yet
- The Spanish Flu Pandemic: Efforts Made to Combat and Subdue the Disease in Luzerne County, PennsylvaniaFrom EverandThe Spanish Flu Pandemic: Efforts Made to Combat and Subdue the Disease in Luzerne County, PennsylvaniaNo ratings yet
- Ebook Cognitive Psychology 7Th Ed PDF Full Chapter PDFDocument67 pagesEbook Cognitive Psychology 7Th Ed PDF Full Chapter PDFchristopher.jenkins207100% (26)
- Ebook Translation As A Science Translation As An Art 2E A Practical Approach PDF Full Chapter PDFDocument67 pagesEbook Translation As A Science Translation As An Art 2E A Practical Approach PDF Full Chapter PDFmark.althoff457100% (28)
- Ebook Pearson Edexcel International Gcse 9 1 Economics Student Book PDF Full Chapter PDFDocument67 pagesEbook Pearson Edexcel International Gcse 9 1 Economics Student Book PDF Full Chapter PDFester.lingberg332100% (29)
- Ebook Pearson Chemistry Foundation 2012 Student Edition PDF Full Chapter PDFDocument67 pagesEbook Pearson Chemistry Foundation 2012 Student Edition PDF Full Chapter PDFester.lingberg332100% (27)
- Filedate - 270download Ebook Transportation A Global Supply Chain Perspective PDF Full Chapter PDFDocument67 pagesFiledate - 270download Ebook Transportation A Global Supply Chain Perspective PDF Full Chapter PDFmark.althoff457100% (30)
- Ebook Handbook On Opium History and Basis of Opioids in Therapeutics PDF Full Chapter PDFDocument67 pagesEbook Handbook On Opium History and Basis of Opioids in Therapeutics PDF Full Chapter PDFforest.gertelman418100% (23)
- Ebook Pavement Design Materials Analysis and Highways PDF Full Chapter PDFDocument67 pagesEbook Pavement Design Materials Analysis and Highways PDF Full Chapter PDFester.lingberg332100% (28)
- Ebook Cognitive Psychology 2E PDF Full Chapter PDFDocument67 pagesEbook Cognitive Psychology 2E PDF Full Chapter PDFchristopher.jenkins207100% (28)
- Ebook Peak Performance Success in College and Beyond 11Th Edition PDF Full Chapter PDFDocument67 pagesEbook Peak Performance Success in College and Beyond 11Th Edition PDF Full Chapter PDFester.lingberg332100% (24)
- Ebook Handbook of The Psychology of Aging PDF Full Chapter PDFDocument67 pagesEbook Handbook of The Psychology of Aging PDF Full Chapter PDFforest.gertelman418100% (27)
- Ebook Handbook of Structural Heart Interventions PDF Full Chapter PDFDocument67 pagesEbook Handbook of Structural Heart Interventions PDF Full Chapter PDFforest.gertelman418100% (27)
- Ebook Pathologic Basis of Veterinary Disease PDF Full Chapter PDFDocument67 pagesEbook Pathologic Basis of Veterinary Disease PDF Full Chapter PDFester.lingberg332100% (27)
- Ebook Cognitive Psychology Connecting Mind Research and Everyday Experience PDF Full Chapter PDFDocument67 pagesEbook Cognitive Psychology Connecting Mind Research and Everyday Experience PDF Full Chapter PDFchristopher.jenkins207100% (29)
- Ebook Cohens Comprehensive Thoracic Anesthesia PDF Full Chapter PDFDocument67 pagesEbook Cohens Comprehensive Thoracic Anesthesia PDF Full Chapter PDFchristopher.jenkins207100% (26)
- The Horn of Africa Diasporas in Italy An Oral 1St Edition Gabriele Proglio Full ChapterDocument67 pagesThe Horn of Africa Diasporas in Italy An Oral 1St Edition Gabriele Proglio Full Chapterlloyd.leos558100% (10)
- Ebook Transition Metal Catalyzed Benzofuran Synthesis PDF Full Chapter PDFDocument67 pagesEbook Transition Metal Catalyzed Benzofuran Synthesis PDF Full Chapter PDFdonald.winkle699100% (29)
- Dental Anatomy Coloring Book 4Th Edition Margaret J Fehrenbach Full ChapterDocument67 pagesDental Anatomy Coloring Book 4Th Edition Margaret J Fehrenbach Full Chapterlouise.butler839100% (13)
- Ebook Transforms and Partial Differential Equations PDF Full Chapter PDFDocument67 pagesEbook Transforms and Partial Differential Equations PDF Full Chapter PDFdonald.winkle699100% (26)
- Hematology Basic Principles and Practice Eighth Edition Ronald Hoffman Full ChapterDocument67 pagesHematology Basic Principles and Practice Eighth Edition Ronald Hoffman Full Chapterbeatrice.corney182100% (11)
- Transcriptomic Profiling and Novel Insights Into The Effect of Ag Ablation On Gonad Development in Macrobrachium Rosenbergii - Ebook PDFDocument36 pagesTranscriptomic Profiling and Novel Insights Into The Effect of Ag Ablation On Gonad Development in Macrobrachium Rosenbergii - Ebook PDFdonald.winkle699100% (29)
- Digital Intimate Publics and Social Media 1St Ed Edition Amy Shields Dobson Full ChapterDocument67 pagesDigital Intimate Publics and Social Media 1St Ed Edition Amy Shields Dobson Full Chapteradolfo.milliken178100% (12)
- Deniable Contact Back Channel Negotiation in Northern Ireland Niall O Dochartaigh Full ChapterDocument67 pagesDeniable Contact Back Channel Negotiation in Northern Ireland Niall O Dochartaigh Full Chapterlouise.butler839100% (12)
- Conservation Drones Mapping and Monitoring Biodiversity Serge A Wich Full ChapterDocument67 pagesConservation Drones Mapping and Monitoring Biodiversity Serge A Wich Full Chapterroger.betschart467100% (6)
- The Little Guide To Getting Your Book Published Simple Steps To Success John Bond Full ChapterDocument67 pagesThe Little Guide To Getting Your Book Published Simple Steps To Success John Bond Full Chapterlou.linares859100% (14)
- Detective Book Club Mystery Omnibus November 1973 Eden Full ChapterDocument51 pagesDetective Book Club Mystery Omnibus November 1973 Eden Full Chapterevan.bowling905100% (4)
- Ebook The Muscular System Manual The Skeletal Muscles of The Human Body PDF Full Chapter PDFDocument67 pagesEbook The Muscular System Manual The Skeletal Muscles of The Human Body PDF Full Chapter PDFrobert.vann805100% (28)
- Ebook Clinical Procedures For Ocular Examination PDF Full Chapter PDFDocument67 pagesEbook Clinical Procedures For Ocular Examination PDF Full Chapter PDFluz.mendoza998100% (30)
- Role Playing Games of Japan Transcultural Dynamics and Orderings 1St Ed Edition Bjorn Ole Kamm All ChapterDocument67 pagesRole Playing Games of Japan Transcultural Dynamics and Orderings 1St Ed Edition Bjorn Ole Kamm All Chapterlloyd.bradley120100% (7)
- Ebook Clinical Reasoning in The Health Professions 4Th Ed PDF Full Chapter PDFDocument67 pagesEbook Clinical Reasoning in The Health Professions 4Th Ed PDF Full Chapter PDFluz.mendoza998100% (27)
- Ebook Transformations Women Gender and Psychology PDF Full Chapter PDFDocument67 pagesEbook Transformations Women Gender and Psychology PDF Full Chapter PDFdonald.winkle699100% (25)
- The New Oxford Handbook of Economic Geography Gordon L Clark Full ChapterDocument67 pagesThe New Oxford Handbook of Economic Geography Gordon L Clark Full Chapterpamela.stanley399100% (7)
- Machine Vision Inspection Systems Vol 1 Image Processing Concepts Malarvel M Ed Full ChapterDocument55 pagesMachine Vision Inspection Systems Vol 1 Image Processing Concepts Malarvel M Ed Full Chaptermaria.wilford563100% (4)
- Global Health Humanity and The Covid 19 Pandemic Philosophical and Sociological Challenges and Imperatives Francis Egbokhare Full ChapterDocument52 pagesGlobal Health Humanity and The Covid 19 Pandemic Philosophical and Sociological Challenges and Imperatives Francis Egbokhare Full Chapterolivia.mohan574100% (8)
- Helping Men Recover A Program For Treating Addiction Cjs Workbook 2Nd Edition Stephanie S Covington Full ChapterDocument67 pagesHelping Men Recover A Program For Treating Addiction Cjs Workbook 2Nd Edition Stephanie S Covington Full Chapterbeatrice.corney182100% (14)
- Wills Trusts and Estate Administration Mindtap Course List 9Th Edition Janis Walter All ChapterDocument67 pagesWills Trusts and Estate Administration Mindtap Course List 9Th Edition Janis Walter All Chapterchristina.brown369100% (10)
- The Mentoring Manual Your Step by Step Guide To Being A Better Mentor Julie Starr Full ChapterDocument67 pagesThe Mentoring Manual Your Step by Step Guide To Being A Better Mentor Julie Starr Full Chapterandrea.davis76583% (6)
- The House of Broken Bricks Fiona Williams Full ChapterDocument67 pagesThe House of Broken Bricks Fiona Williams Full Chapterlloyd.leos558100% (12)
- Real Estate Principles A Value Approach 6Th Edition David C Ling All ChapterDocument67 pagesReal Estate Principles A Value Approach 6Th Edition David C Ling All Chapterdonna.chavis420100% (15)
- Oswaal Cbse Sample Question Paper For Term 2 Class 10 Social Science Book For 2022 Exam Oswaal Editorial Board Download PDF ChapterDocument52 pagesOswaal Cbse Sample Question Paper For Term 2 Class 10 Social Science Book For 2022 Exam Oswaal Editorial Board Download PDF Chapterrichard.willman763100% (4)
- After Injury A Historical Anatomy of Forgiveness Resentment and Apology Ashraf H A Rushdy Full ChapterDocument51 pagesAfter Injury A Historical Anatomy of Forgiveness Resentment and Apology Ashraf H A Rushdy Full Chaptergregory.king174100% (5)
- Wills Trusts and Estate Administration 9Th Edition Janis Walter All ChapterDocument67 pagesWills Trusts and Estate Administration 9Th Edition Janis Walter All Chapterchristina.brown369100% (14)
- Understanding Human Behavior A Guide For Health Care Professionals Mindtap Course List 10Th Edition Alyson Honeycutt All ChapterDocument68 pagesUnderstanding Human Behavior A Guide For Health Care Professionals Mindtap Course List 10Th Edition Alyson Honeycutt All Chapterbrittany.ylonen552100% (4)
- Global Environmental Sustainability: Case Studies and Analysis of The United Nations' Journey Toward Sustainable Development Choy Yee KeongDocument48 pagesGlobal Environmental Sustainability: Case Studies and Analysis of The United Nations' Journey Toward Sustainable Development Choy Yee Keongolivia.mohan574100% (7)
- Explorations Introduction To Astronomy 8Th Edition Arny Test Bank PDFDocument25 pagesExplorations Introduction To Astronomy 8Th Edition Arny Test Bank PDFedwin.potter616100% (16)
- Formative Modernities in The Early Modern Atlantic and Beyond Identities Polities and Glocal Economies Veronika Hyden Hanscho Full ChapterDocument68 pagesFormative Modernities in The Early Modern Atlantic and Beyond Identities Polities and Glocal Economies Veronika Hyden Hanscho Full Chaptermichael.fabbri667100% (5)
- Ebook The Neuroicu Board Review PDF Full Chapter PDFDocument67 pagesEbook The Neuroicu Board Review PDF Full Chapter PDFrobert.vann805100% (27)
- Solution Manual For Introduction To Veterinary Science 3Rd Edition Lawhead Baker 1319013384 9781111542795 Full Chapter PDFDocument32 pagesSolution Manual For Introduction To Veterinary Science 3Rd Edition Lawhead Baker 1319013384 9781111542795 Full Chapter PDFlatarsha.soriano420100% (17)
- Digital Inequalities in The Global South 1St Ed Edition Massimo Ragnedda Full ChapterDocument49 pagesDigital Inequalities in The Global South 1St Ed Edition Massimo Ragnedda Full Chapteradolfo.milliken178100% (16)
- The Metalogicon of John Salisbury Daniel D Mcgarry Full ChapterDocument67 pagesThe Metalogicon of John Salisbury Daniel D Mcgarry Full Chapterandrea.davis765100% (7)
- Modern Principles of Economics 3Rd Edition Cowen Solutions Manual Full Chapter PDFDocument31 pagesModern Principles of Economics 3Rd Edition Cowen Solutions Manual Full Chapter PDFbilly.koenitzer727100% (11)
- Ebook Groups Process and Practice PDF Full Chapter PDFDocument67 pagesEbook Groups Process and Practice PDF Full Chapter PDFkathleen.lloyd406100% (27)
- Inheritance and Innovation in A Colonial Language Towards A Usage Based Account of French Guianese Creole 1St Edition William Jennings Full ChapterDocument68 pagesInheritance and Innovation in A Colonial Language Towards A Usage Based Account of French Guianese Creole 1St Edition William Jennings Full Chapterdana.williams472100% (5)
- Full Download Book Biomass Biofuels Biochemicals Microbial Fermentation of Biowastes PDFDocument41 pagesFull Download Book Biomass Biofuels Biochemicals Microbial Fermentation of Biowastes PDFjerome.ruiz660100% (15)
- The Spanish Flu Pandemic of 1918Document5 pagesThe Spanish Flu Pandemic of 1918jellNo ratings yet
- Findlay, G. The First Recognized Epidemic of Yellow Fever PDFDocument12 pagesFindlay, G. The First Recognized Epidemic of Yellow Fever PDFJean SegataNo ratings yet
- Black Death-ArticleDocument4 pagesBlack Death-ArticleAdrien BaziretNo ratings yet
- Spanish Flu ThesisDocument5 pagesSpanish Flu ThesisSomeoneToWriteMyPaperForMeCanada100% (2)
- Alfred W.mccann - Starving AmericaDocument282 pagesAlfred W.mccann - Starving Americaannedorival6718No ratings yet
- HSCI130 Tutorial Exercise - Incidence & Prevalence ANSWER KEYDocument4 pagesHSCI130 Tutorial Exercise - Incidence & Prevalence ANSWER KEYarurojo100% (1)
- Ampicillin 2Document1 pageAmpicillin 2Kristine YoungNo ratings yet
- Anuj Subedi: Certificate of AchievementDocument2 pagesAnuj Subedi: Certificate of AchievementAnuj SubediNo ratings yet
- 4 Effective Ways To Prevent COVID-19Document2 pages4 Effective Ways To Prevent COVID-19bhuiyan1No ratings yet
- Hand-Foot-Mouth DiseaseDocument28 pagesHand-Foot-Mouth Diseasebrillniks100% (2)
- Department of Health and Human Services SubmissionDocument85 pagesDepartment of Health and Human Services SubmissionMathewDunckleyNo ratings yet
- Association and CausationDocument16 pagesAssociation and CausationnyangaraNo ratings yet
- Body System ChecklistDocument8 pagesBody System Checklistapi-421876369No ratings yet
- Parasitic Zoonoses and Diagnostics For Dogs Dr.Document3 pagesParasitic Zoonoses and Diagnostics For Dogs Dr.pundaipundaiNo ratings yet
- Cuneyt Alper MD, Charles Bluestone MD, Margaretha Casselbrant, Joseph Dohar MD, Ellen Mandel MD - Advanced Therapy of Otitis Media (2003, PMPH Usa)Document576 pagesCuneyt Alper MD, Charles Bluestone MD, Margaretha Casselbrant, Joseph Dohar MD, Ellen Mandel MD - Advanced Therapy of Otitis Media (2003, PMPH Usa)Carmen-BadeaNo ratings yet
- UNCC300 Assesment TAsk 2Document2 pagesUNCC300 Assesment TAsk 2Spandan DahalNo ratings yet
- ECPE All-Star Practice Tests New Cloze TestDocument13 pagesECPE All-Star Practice Tests New Cloze Testsiana_shNo ratings yet
- NlecDocument2 pagesNlecJocelyn TabudlongNo ratings yet
- Neurology 2014 BrouwerDocument10 pagesNeurology 2014 BrouwerAndrea Cayufilo CarmonaNo ratings yet
- SiddhaDocument4 pagesSiddhaStephin MNo ratings yet
- Tippu Sultan Cover Story in AM - July 2012 FullDocument44 pagesTippu Sultan Cover Story in AM - July 2012 FullHarikumar NairNo ratings yet
- Baldacchino Et Al 2013 Stomoxys Tramsmisión EnfermedadesDocument13 pagesBaldacchino Et Al 2013 Stomoxys Tramsmisión EnfermedadesjuanNo ratings yet
- NCP PTBDocument9 pagesNCP PTBecbarticanNo ratings yet
- 01 - History of PlumbingDocument1 page01 - History of PlumbingJefferson Kevin LerioNo ratings yet
- The Worst Mistake in The History of The Human Race - by Jared DiamondDocument4 pagesThe Worst Mistake in The History of The Human Race - by Jared DiamondwhychooseoneNo ratings yet
- Omsk KomplikasiDocument10 pagesOmsk KomplikasiYudwari Adhicha Nuredis HarahapNo ratings yet
- John CarnevaleDocument8 pagesJohn Carnevaleapi-209693106No ratings yet
- UntitledDocument60 pagesUntitledoutdash2No ratings yet
- 2000a 2014 PDFDocument4 pages2000a 2014 PDFAl-Emran HossainNo ratings yet
- DH Health Assessment FormDocument3 pagesDH Health Assessment FormRayceNo ratings yet
- Final Portion Size Control and Nutrition Related Cronic Disease 1Document16 pagesFinal Portion Size Control and Nutrition Related Cronic Disease 1api-302598263No ratings yet
- Differential Leukocyte Count:: The Types of LeukocytesDocument4 pagesDifferential Leukocyte Count:: The Types of LeukocytesSuandiNo ratings yet
- Strategies For Sustainable DevelopmentDocument3 pagesStrategies For Sustainable DevelopmentzinebNo ratings yet
- Biology Investigatory Project (Advanced)Document27 pagesBiology Investigatory Project (Advanced)Yogi Arya75% (4)