You might also like
- PPP Reading Test 6 Parts BC Question PaperDocument16 pagesPPP Reading Test 6 Parts BC Question PaperJaisy Martin100% (3)
- Reading Test 5 - Necrotizing FascilitisDocument8 pagesReading Test 5 - Necrotizing FascilitisOlive GroupNo ratings yet
- Reading Sample Test 5 - Reading Part BC Question PaperDocument16 pagesReading Sample Test 5 - Reading Part BC Question PaperNanda NandaNo ratings yet
- Practice Test 2 Reading Part BDocument5 pagesPractice Test 2 Reading Part BkholiooNo ratings yet
- Oet R - SarsDocument16 pagesOet R - SarsVic Kwan100% (1)
- Reading Sample Test 1 Question Paper Part BCDocument14 pagesReading Sample Test 1 Question Paper Part BCvidyaNo ratings yet
- ReadingTest Question Paper Part B CDocument16 pagesReadingTest Question Paper Part B CkholiooNo ratings yet
- CRT Exam Review Guide Chapter 9Document9 pagesCRT Exam Review Guide Chapter 9Dharlyn MungcalNo ratings yet
- PPP Reading Test 7 Parts BC Question PaperDocument16 pagesPPP Reading Test 7 Parts BC Question PaperhaffizmoradNo ratings yet
- Reading Sample Test 1 Question Paper Part BCDocument16 pagesReading Sample Test 1 Question Paper Part BCpratim deyNo ratings yet
- June 2009 Nursing Practice 1Document9 pagesJune 2009 Nursing Practice 1Karl Gabriel BonifacioNo ratings yet
- Board Exam Compilation Book 2Document163 pagesBoard Exam Compilation Book 2Aaron Cy Untalan100% (6)
- Care of The Older Adult-SAS 1Document5 pagesCare of The Older Adult-SAS 1Gia Lourdes Camille AustriaNo ratings yet
- Reading Sub-Test - Question Paper: Parts B & CDocument16 pagesReading Sub-Test - Question Paper: Parts B & CShyju Paul100% (1)
- Iilt File 13Document23 pagesIilt File 13Rosmin AnsuNo ratings yet
- NP 1Document22 pagesNP 1June DumdumayaNo ratings yet
- MOCK Read BC PDFDocument16 pagesMOCK Read BC PDFfaysal83% (6)
- Ignatavicius: Medical-Surgical Nursing, 9th EditionDocument5 pagesIgnatavicius: Medical-Surgical Nursing, 9th Editionfunky goodNo ratings yet
- Occupational English Test Oet Reading Part BC Test 04Document16 pagesOccupational English Test Oet Reading Part BC Test 04AndreaNo ratings yet
- Oxygen QuizDocument22 pagesOxygen Quizracalsarahjane50% (2)
- DEC 2007-NPT 3-Questions and RationaleDocument20 pagesDEC 2007-NPT 3-Questions and RationaleRoy SalvadorNo ratings yet
- Reading Sub-Test: Part ADocument17 pagesReading Sub-Test: Part AVijayalakshmi Narayanaswami78% (9)
- NLE - Practice TestsDocument25 pagesNLE - Practice TestsBen0% (1)
- Wa0011.Document10 pagesWa0011.SojiNo ratings yet
- Nursing Fundamentals Questions With RationaleDocument2 pagesNursing Fundamentals Questions With Rationalemae7777No ratings yet
- UntitledDocument20 pagesUntitledstuffednurse100% (1)
- A Guide To Performing Quality Assured Diagnostic SpirometryDocument28 pagesA Guide To Performing Quality Assured Diagnostic SpirometryLaura MoiseNo ratings yet
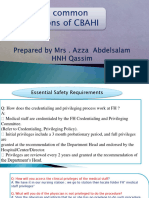
- Mostcommonquestionsofcbahi Azza 230211125221 89d97424Document58 pagesMostcommonquestionsofcbahi Azza 230211125221 89d97424amal.jaberNo ratings yet
- OET 2 Reading Test 10 Part BDocument4 pagesOET 2 Reading Test 10 Part BAlice ChirilaNo ratings yet
- Care of The Older Adult - SAS 3Document4 pagesCare of The Older Adult - SAS 3Gia Lourdes Camille AustriaNo ratings yet
- Acr Practice Parameter For The Performance of Fluoroscopic Contrast Enema Examination in AdultsDocument8 pagesAcr Practice Parameter For The Performance of Fluoroscopic Contrast Enema Examination in AdultsHercules RianiNo ratings yet
- Board Exam Compilation Book 2 SampleDocument11 pagesBoard Exam Compilation Book 2 SampleElizabella Henrietta TanaquilNo ratings yet
- Chapter 30: Health Assessment and Physical Examination: Test BankDocument23 pagesChapter 30: Health Assessment and Physical Examination: Test BankNurse UtopiaNo ratings yet
- Pharmacology For The Primary Care Provider 4Th Edition Edmunds Test Bank Full Chapter PDFDocument26 pagesPharmacology For The Primary Care Provider 4Th Edition Edmunds Test Bank Full Chapter PDFCodyDavistgny100% (7)
- Concepts For Nursing Practice Giddens 1st Edition Test BankDocument5 pagesConcepts For Nursing Practice Giddens 1st Edition Test Bankjoshuamorrisosqbfrtijk100% (34)
- Fundamentals of Nursing QuestionsDocument74 pagesFundamentals of Nursing QuestionsGillie Brun Lucero89% (9)
- FREE NLE REVIEW Fundies and OthersDocument40 pagesFREE NLE REVIEW Fundies and OthersAngel Lopez100% (1)
- Ebook PDF Brunner Suddarths Handbook of Laboratory and Diagnostic Tests Third Edition PDF Docx Full Chapter Chapter ScribdDocument41 pagesEbook PDF Brunner Suddarths Handbook of Laboratory and Diagnostic Tests Third Edition PDF Docx Full Chapter Chapter Scribdangela.talaga591100% (17)
- Acute Care Day - Respiratory SCENARIO - The Patient With Acute Asthma Notes For The Instructor - Not Volunteered To StudentsDocument10 pagesAcute Care Day - Respiratory SCENARIO - The Patient With Acute Asthma Notes For The Instructor - Not Volunteered To StudentsNomzwakhe KgwaleNo ratings yet
- Board Exam Compilation Book 2 SampleDocument10 pagesBoard Exam Compilation Book 2 SampleebookwholesellerNo ratings yet
- NCM 109 Skills Lab Day 2 CBG22Document20 pagesNCM 109 Skills Lab Day 2 CBG22Joseph DusichNo ratings yet
- FTC SCRIPT O2 ADDocument2 pagesFTC SCRIPT O2 ADJUSTIN ALZATENo ratings yet
- Focus Charting 2Document65 pagesFocus Charting 2Ella Caro100% (1)
- Federal Register / Vol. 69, No. 219 / Monday, November 15, 2004 / Rules and RegulationsDocument50 pagesFederal Register / Vol. 69, No. 219 / Monday, November 15, 2004 / Rules and RegulationsEdward BlackNo ratings yet
- Reading Sample Test 1 Question Paper Part BCDocument16 pagesReading Sample Test 1 Question Paper Part BCSusan HsiaoNo ratings yet
- Wa0009.Document11 pagesWa0009.SojiNo ratings yet
- Study MaterialDocument30 pagesStudy MaterialDivya AggarwalNo ratings yet
- Scholarship ExamDocument16 pagesScholarship ExamRicky Vanguardia IIINo ratings yet
- IPSGDocument16 pagesIPSGNyimas Milka Ayu NabilaNo ratings yet
- Test Bank For Medical Surgical Nursing Patient Centered Collaborative Care 7th Edition IgnataviciusDocument9 pagesTest Bank For Medical Surgical Nursing Patient Centered Collaborative Care 7th Edition IgnataviciusM Syaiful Islam43% (7)
- Quiz 3Document13 pagesQuiz 3Chora BaguiyacNo ratings yet
- You Are Caring For A Patient With An NG Feeding TubeDocument2 pagesYou Are Caring For A Patient With An NG Feeding TubeWen Silver100% (1)
- RT ConsultDocument5 pagesRT ConsultRick Frea100% (2)
- #29 LEAN in The Lab 2Document5 pages#29 LEAN in The Lab 2asclswisconsinNo ratings yet
- 1Document8 pages1Tyson Easo JonesNo ratings yet
- Nle Pre Board June 2008 Npt1-Questions and RationaleDocument25 pagesNle Pre Board June 2008 Npt1-Questions and RationaleAna Marie Besa Battung-ZalunNo ratings yet
- Lumbar PunctureDocument5 pagesLumbar Puncturesetanpikulan100% (1)
- Laboratory Assessment of Nutritional Status: Bridging Theory & PracticeFrom EverandLaboratory Assessment of Nutritional Status: Bridging Theory & PracticeRating: 1 out of 5 stars1/5 (1)
- Questions and Answers for the Specialty Recruitment AssessmentFrom EverandQuestions and Answers for the Specialty Recruitment AssessmentRating: 2 out of 5 stars2/5 (5)
- CRQs and SBAs for the Final FRCA: Questions and detailed answersFrom EverandCRQs and SBAs for the Final FRCA: Questions and detailed answersNo ratings yet
- Listening Test 8 QPDocument12 pagesListening Test 8 QPkimNo ratings yet
- Reading Test 10 (With Answers)Document17 pagesReading Test 10 (With Answers)kimNo ratings yet
- Overweight and Obese Children Reading Oet NoteDocument16 pagesOverweight and Obese Children Reading Oet NoteHarel Hevin100% (4)
- Writing Test 4Document5 pagesWriting Test 4kimNo ratings yet
- ADHDDocument14 pagesADHDPrsh Sanna PaudlNo ratings yet
- Test 3 Reading Part A Answer KeyDocument2 pagesTest 3 Reading Part A Answer KeykimNo ratings yet
- OET Listening Test Question PaperDocument10 pagesOET Listening Test Question PaperkimNo ratings yet
- Pharmacovigilance - KhimyaDocument22 pagesPharmacovigilance - KhimyakimNo ratings yet
- Induction and Training Road-Map: GenpactDocument27 pagesInduction and Training Road-Map: GenpactShrey KanungoNo ratings yet
- 90 + 100 + 5 - 7. 5 Tens, 3 Hundreds, 8 Ones - 8. 400 + 1000 + 20 + 8 - 9. 5 Hundreds, 6 Tens, 9 Ones - 10. 1 Hundred, 1 Thousands, 3 OnesDocument2 pages90 + 100 + 5 - 7. 5 Tens, 3 Hundreds, 8 Ones - 8. 400 + 1000 + 20 + 8 - 9. 5 Hundreds, 6 Tens, 9 Ones - 10. 1 Hundred, 1 Thousands, 3 OnesLorna HerillaNo ratings yet
- Habeas CorpusDocument67 pagesHabeas CorpusButch AmbataliNo ratings yet
- SAP Manufacturing Implementation Architecture-1Document17 pagesSAP Manufacturing Implementation Architecture-1andriesbuterNo ratings yet
- First Language English (Oral Endorsement)Document58 pagesFirst Language English (Oral Endorsement)sheesNo ratings yet
- How To Change The Default Displayed Category in Point of Sale - OdooDocument4 pagesHow To Change The Default Displayed Category in Point of Sale - OdooDenaNo ratings yet
- Design Scenario Chapter 5Document6 pagesDesign Scenario Chapter 5jtrillossNo ratings yet
- Unit 2 - Chapter 2Document20 pagesUnit 2 - Chapter 2Dennise Kate CabiedesNo ratings yet
- Lirik KoreaDocument6 pagesLirik KoreaSabrina Winyard ChrisNo ratings yet
- 7 P's of McDonaldsDocument11 pages7 P's of McDonaldsdd1684100% (4)
- Resolution No. 1433Document2 pagesResolution No. 1433MA. DIVINA LAPURANo ratings yet
- Soni Musicae Diato K2 enDocument2 pagesSoni Musicae Diato K2 enknoNo ratings yet
- Courtney Loper-ResumeDocument2 pagesCourtney Loper-Resumeapi-354618234No ratings yet
- English IODocument6 pagesEnglish IOAarav MathurNo ratings yet
- Forrester Hybrid Integration PlatformDocument17 pagesForrester Hybrid Integration PlatformrtNo ratings yet
- Department of Education: Supervisory Report School/District: Cacawan High SchoolDocument17 pagesDepartment of Education: Supervisory Report School/District: Cacawan High SchoolMaze JasminNo ratings yet
- Distribution of BBT EbooksDocument7 pagesDistribution of BBT EbooksAleksandr N ValentinaNo ratings yet
- WEF GLF BrochureDocument12 pagesWEF GLF BrochureDibyajyoti NathNo ratings yet
- Supplementary Cause List - 16.10.2023Document7 pagesSupplementary Cause List - 16.10.2023Aamir BhatNo ratings yet
- Axie Infinity Reviewer - by MhonDocument29 pagesAxie Infinity Reviewer - by MhonGodisGood AlltheTime100% (2)
- Searchinger Et Al Nature 2018Document4 pagesSearchinger Et Al Nature 2018Bjart HoltsmarkNo ratings yet
- How To Write SpecificationsDocument9 pagesHow To Write SpecificationsLeilani ManalaysayNo ratings yet
- Tatanka Oyate 2 EngDocument3 pagesTatanka Oyate 2 EngdesiNo ratings yet
- Cantilever Slab Beam Design For TorsionDocument17 pagesCantilever Slab Beam Design For TorsionNikhil100% (1)
- Pamrex - Manhole CoversDocument6 pagesPamrex - Manhole CoversZivadin LukicNo ratings yet
- Willis, D. - Visualizing Political StruggleDocument11 pagesWillis, D. - Visualizing Political StruggleAndreea Mitreanu100% (3)
- Abhimanshree SampleDocument4 pagesAbhimanshree SampleMandar KurkureNo ratings yet
- HOME ECO (Decision Making 1-3)Document3 pagesHOME ECO (Decision Making 1-3)Ruth Belle HolgadoNo ratings yet
- 2021 06 WJU Circus Fanfare NOV DECDocument28 pages2021 06 WJU Circus Fanfare NOV DECDwarven SniperNo ratings yet
- Roman Empire Revived TheoryDocument173 pagesRoman Empire Revived TheoryBrenoliNo ratings yet