You might also like
- Smith L (2017) Nursing Times 113: 12, 20-23Document59 pagesSmith L (2017) Nursing Times 113: 12, 20-23Derick RanaNo ratings yet
- Letter of ProfessionalismDocument1 pageLetter of ProfessionalismDerick RanaNo ratings yet
- INFORMED CONSENT FOR HIV TESTINGDocument2 pagesINFORMED CONSENT FOR HIV TESTINGMangchaaLaguna MilkTea83% (6)
- Question On IV FluidsDocument1 pageQuestion On IV FluidsDerick RanaNo ratings yet
- Diabetes Mellitus: Assessment Diagnosis Planning Intervention Rationale EvaluationDocument12 pagesDiabetes Mellitus: Assessment Diagnosis Planning Intervention Rationale EvaluationDerick RanaNo ratings yet
- Diabetes Nursing EducationDocument4 pagesDiabetes Nursing EducationDerick RanaNo ratings yet
- Ic-01-040 Infection Control in Dental ClinicDocument11 pagesIc-01-040 Infection Control in Dental ClinicDerick RanaNo ratings yet
- Process Step DischargeDocument3 pagesProcess Step DischargeDerick RanaNo ratings yet
- Diabetes Nursing Education and PracticeDocument34 pagesDiabetes Nursing Education and PracticeDerick RanaNo ratings yet
- Ic-01-047 Infection Control in Operating RoomDocument13 pagesIc-01-047 Infection Control in Operating RoomDerick RanaNo ratings yet
- Linen Needs To Be Accounted For LaundryDocument1 pageLinen Needs To Be Accounted For LaundryDerick RanaNo ratings yet
- Abortion WorkflowDocument1 pageAbortion WorkflowDerick RanaNo ratings yet
- Ic-01-042 Infection Control in Emergency RoomDocument13 pagesIc-01-042 Infection Control in Emergency RoomDerick RanaNo ratings yet
- Policies and Procedures for Infection ControlDocument9 pagesPolicies and Procedures for Infection ControlDerick RanaNo ratings yet
- Ic-01-048 Infection Control in Pediatric Intensive Care UnitDocument6 pagesIc-01-048 Infection Control in Pediatric Intensive Care UnitDerick RanaNo ratings yet
- Ic-01-047 Infection Control in Operating RoomDocument13 pagesIc-01-047 Infection Control in Operating RoomDerick RanaNo ratings yet
- Ic-01-049 Infection Control in Clinical EngineeringDocument4 pagesIc-01-049 Infection Control in Clinical EngineeringDerick RanaNo ratings yet
- Ic-01-040 Infection Control in Dental ClinicDocument11 pagesIc-01-040 Infection Control in Dental ClinicDerick RanaNo ratings yet
- Policies and Procedures for Infection ControlDocument9 pagesPolicies and Procedures for Infection ControlDerick RanaNo ratings yet
- Ic-01-041 Infection Control in DialysisDocument15 pagesIc-01-041 Infection Control in DialysisDerick RanaNo ratings yet
- Ic-01-048 Infection Control in Pediatric Intensive Care UnitDocument6 pagesIc-01-048 Infection Control in Pediatric Intensive Care UnitDerick RanaNo ratings yet
- Critical Care Notes BookDocument142 pagesCritical Care Notes BookDerick RanaNo ratings yet
- Ic-01-039 Infection Control in Adult Intensive Care UnitDocument7 pagesIc-01-039 Infection Control in Adult Intensive Care UnitDerick RanaNo ratings yet
- Caring for Dementia PatientsDocument4 pagesCaring for Dementia PatientsDerick RanaNo ratings yet
- Recruitment Checklist: Security Forces Hospital ProgramDocument4 pagesRecruitment Checklist: Security Forces Hospital ProgramDerick RanaNo ratings yet
- Ic-01-039 Infection Control in Adult Intensive Care UnitDocument7 pagesIc-01-039 Infection Control in Adult Intensive Care UnitDerick RanaNo ratings yet
- Smith L (2017) Nursing Times 113: 12, 20-23Document59 pagesSmith L (2017) Nursing Times 113: 12, 20-23Derick RanaNo ratings yet
- Nursing Fluids and ElectrolytesDocument14 pagesNursing Fluids and Electrolytesaga1028100% (18)
- Emergency NursingDocument5 pagesEmergency NursingDerick RanaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
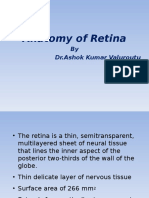
- Anatomy of Retina: by DR - Ashok Kumar ValuroutuDocument49 pagesAnatomy of Retina: by DR - Ashok Kumar ValuroutuanamariaboariuNo ratings yet
- GenEd (Aug 22, 2022)Document34 pagesGenEd (Aug 22, 2022)Maylyn ShishidoNo ratings yet
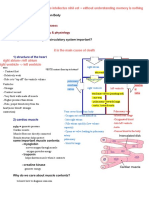
- 10.2 Circulatory System: Group 2Document15 pages10.2 Circulatory System: Group 2DANISTTA A/P LOGARAJAH MoeNo ratings yet
- P.E Answer KeyDocument3 pagesP.E Answer KeyAustinly Bermejo67% (6)
- Manual Advance First AidDocument127 pagesManual Advance First AidLee Khai ChienNo ratings yet
- Korean Hand Therapy KHT Syllabus PDFDocument15 pagesKorean Hand Therapy KHT Syllabus PDFAurora Alina Bujor-FlueranNo ratings yet
- LESSON 7 - CAPILLARY PUNCTURE EQUIPMENT AND PROCEDUREDocument2 pagesLESSON 7 - CAPILLARY PUNCTURE EQUIPMENT AND PROCEDUREkhakimagdalenaNo ratings yet
- 1st Periodic Exam g9Document3 pages1st Periodic Exam g9Vincent Franciz T. FernandezNo ratings yet
- Correlation Between Pregnancy Outcome and PlacentalDocument5 pagesCorrelation Between Pregnancy Outcome and PlacentalnskhldNo ratings yet
- Smoking and Its EffectsDocument28 pagesSmoking and Its EffectsXEDGER09No ratings yet
- Biology C - Lesson 1 - Circulatory SystemDocument46 pagesBiology C - Lesson 1 - Circulatory SystemMuhammad Azrie0% (1)
- Fertilization and Implantation ProcessDocument16 pagesFertilization and Implantation ProcessIgnacio FelicityNo ratings yet
- 0610 s17 Ms 41Document12 pages0610 s17 Ms 41pkrajenpillaygmailcomNo ratings yet
- Edoc - Pub Switchwords CodebookDocument113 pagesEdoc - Pub Switchwords CodebookARCHANNAA100% (1)
- High Altitude Anaesthesia PDFDocument7 pagesHigh Altitude Anaesthesia PDFK.krishna PriyaNo ratings yet
- Exercise Physiology NotesDocument41 pagesExercise Physiology Notesstarlight9394100% (1)
- Word Part ReviewDocument6 pagesWord Part ReviewRanee ToNo ratings yet
- KISS Maintaining A BalanceDocument32 pagesKISS Maintaining A BalanceL50% (2)
- Kami Export - Cardiovascular System Lecture Outline 1st PeriodDocument16 pagesKami Export - Cardiovascular System Lecture Outline 1st PeriodJada NovakNo ratings yet
- General Heart Diagram, Handout Heart Diagram, Vessels HandoutDocument4 pagesGeneral Heart Diagram, Handout Heart Diagram, Vessels HandoutJNo ratings yet
- Ebook Ebook PDF Principles of Human Physiology 6th Edition PDFDocument41 pagesEbook Ebook PDF Principles of Human Physiology 6th Edition PDFdonita.nichols650100% (35)
- Circulatory System Class 5Document20 pagesCirculatory System Class 5zoey9099747888No ratings yet
- Intra Aortic Balloon CounterpulsationDocument39 pagesIntra Aortic Balloon Counterpulsationmerin sunilNo ratings yet
- Intravenous MonitorDocument39 pagesIntravenous MonitorGeogrina WatsonNo ratings yet
- GEAS Problems 1Document7 pagesGEAS Problems 1Jayson CorpuzNo ratings yet
- Every Day Science Part 2 PDFDocument68 pagesEvery Day Science Part 2 PDFSadam GillalNo ratings yet
- Anatomy and Physiology Nails E-BookDocument22 pagesAnatomy and Physiology Nails E-BookdzemamejaNo ratings yet
- Vital Signs Vital Signs: Importance: ImportanceDocument6 pagesVital Signs Vital Signs: Importance: ImportanceTyron KristianNo ratings yet
- Chapter 1: Transport: Prepared By: Ling Mei TengDocument21 pagesChapter 1: Transport: Prepared By: Ling Mei TengJuliet LingNo ratings yet
- Circulatory System Gizmo - 5 Mark TestDocument3 pagesCirculatory System Gizmo - 5 Mark TestDhruv VmNo ratings yet