You might also like
- Corona VirusDocument27 pagesCorona Viruspardhaja.vaishnaviNo ratings yet
- Coronavirus ResearchDocument6 pagesCoronavirus ResearchSandra IglesiasNo ratings yet
- Patho Finaly 2 PaperDocument34 pagesPatho Finaly 2 PaperOlivia JagroopNo ratings yet
- COVID-19: UM Icrob Iolog yDocument50 pagesCOVID-19: UM Icrob Iolog yJana AbdulrahimNo ratings yet
- COVID-19: Shahid Afreed MDocument10 pagesCOVID-19: Shahid Afreed MArdra SRNo ratings yet
- COVIDDocument7 pagesCOVIDSky AgtarapNo ratings yet
- Rafaela Macatangay Mid Term ProjectDocument2 pagesRafaela Macatangay Mid Term ProjectAlmirah H. AliNo ratings yet
- Picornaviridae & Adenoviridae - Raja Pardomuan HarahapDocument63 pagesPicornaviridae & Adenoviridae - Raja Pardomuan HarahapM. RamazaliNo ratings yet
- (COVID - 19) : Chapter 1 - Introduction To World PandamicDocument21 pages(COVID - 19) : Chapter 1 - Introduction To World PandamicKAUSHLESH CHOUDHARYNo ratings yet
- Viral Infection of The Respiratory SystemDocument18 pagesViral Infection of The Respiratory SystemAbdus SubhanNo ratings yet
- Sars Vs CovidDocument11 pagesSars Vs CovidYu Theng ChumNo ratings yet
- InfluenzaDocument43 pagesInfluenzaAdrul FauzanNo ratings yet
- Genomic Characterization of The 2019 Novel Human-Pathogenic Coronavirus Isolated From A Patient With Atypical Pneumonia After Visiting WuhanDocument18 pagesGenomic Characterization of The 2019 Novel Human-Pathogenic Coronavirus Isolated From A Patient With Atypical Pneumonia After Visiting WuhanMuhamad vero SyatiaNo ratings yet
- Virology Respiratory VirusesDocument6 pagesVirology Respiratory VirusesHisham ChomanyNo ratings yet
- Biology Investigatoy Project - 12Document14 pagesBiology Investigatoy Project - 12Skybro SuryaNo ratings yet
- New Microsoft Word DocumentDocument14 pagesNew Microsoft Word DocumentShravan ZoneNo ratings yet
- Viruses 2Document14 pagesViruses 2Cezar Alexander GuevaraNo ratings yet
- Negative Stranded RNA VirusesDocument47 pagesNegative Stranded RNA VirusesNovie Carla GayosaNo ratings yet
- A Presentation On Corona Virus: by MRMC-07, Batch: BDocument42 pagesA Presentation On Corona Virus: by MRMC-07, Batch: BTanjin novaNo ratings yet
- Severe Acute Respiratory Syndrome (SARS)Document9 pagesSevere Acute Respiratory Syndrome (SARS)Elenor AbrigoNo ratings yet
- Covid 19Document42 pagesCovid 19ok100% (3)
- Factsheet For Health Professionals On CoronavirusesDocument8 pagesFactsheet For Health Professionals On CoronavirusesTahir AliNo ratings yet
- Handouts SARS and Bird FluDocument6 pagesHandouts SARS and Bird FluChin ChinNo ratings yet
- Coronaviruses Perlman-and-McIntosh 155 PDFDocument12 pagesCoronaviruses Perlman-and-McIntosh 155 PDFVenkatesan DevendranNo ratings yet
- Comparative Analysis: Covid-19, H1N1, Sars-Cov, and Mers-CovDocument10 pagesComparative Analysis: Covid-19, H1N1, Sars-Cov, and Mers-CovEdelrose Lapitan100% (1)
- English Covid-19 Streinu AlexandruDocument14 pagesEnglish Covid-19 Streinu AlexandruGabriel Alexandru StreinuNo ratings yet
- What Is Coronavirus? The Different Types of CoronavirusesDocument9 pagesWhat Is Coronavirus? The Different Types of Coronavirusesashley bendanaNo ratings yet
- Covid 19Document15 pagesCovid 19Zubair GhouriNo ratings yet
- COVID-19 Infection: Origin, Transmission, and Characteristics of Human CoronavirusesDocument6 pagesCOVID-19 Infection: Origin, Transmission, and Characteristics of Human CoronavirusesmirakeNo ratings yet
- Features, Evaluation and Treatment Coronavirus (COVID-19)Document19 pagesFeatures, Evaluation and Treatment Coronavirus (COVID-19)Prem Shankar GuptaNo ratings yet
- Background of The Problem: Sarbecovirus, OrthocoronavirinaeDocument16 pagesBackground of The Problem: Sarbecovirus, Orthocoronavirinaesamiza1122No ratings yet
- Croup - Clinical Features, Evaluation, and Diagnosis - UpToDateDocument43 pagesCroup - Clinical Features, Evaluation, and Diagnosis - UpToDateRafaela BassettiNo ratings yet
- Viral InfectionDocument35 pagesViral Infectionanushka guptaNo ratings yet
- 4A - Group 1 - Adenoviridae & CoronaviridaeDocument41 pages4A - Group 1 - Adenoviridae & CoronaviridaeLowella Rose C. DonguinesNo ratings yet
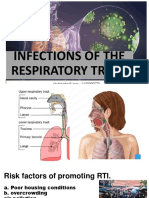
- INFECTIONS OF THE RESPIRATORY TRACT AND G CompleteDocument39 pagesINFECTIONS OF THE RESPIRATORY TRACT AND G CompleteShekaina SumagangNo ratings yet
- Coronavirus CVDocument126 pagesCoronavirus CVShourendranath MondalNo ratings yet
- Corona Virus PresentationDocument29 pagesCorona Virus PresentationUmer naeemNo ratings yet
- COVID-19 LEGACY: SARS-CoV-2 clinical trials, vaccines trials and bioethicsFrom EverandCOVID-19 LEGACY: SARS-CoV-2 clinical trials, vaccines trials and bioethicsNo ratings yet
- Corona ParamyxoviridaeDocument41 pagesCorona Paramyxoviridaeshikha yadavNo ratings yet
- Coronavirus & COVID-19Document62 pagesCoronavirus & COVID-19Prajwal Rao KNo ratings yet
- Covid 19 NeetDocument4 pagesCovid 19 NeetDipangkar SarkarNo ratings yet
- Corona VirusesDocument61 pagesCorona VirusesNaing Lin SoeNo ratings yet
- Corona VDocument56 pagesCorona VAhmed ElsawafNo ratings yet
- Coping with COVID-19: Practical and Efficient Ways on How to Prevent, Prepare, and Protect You and Your Family from the Wuhan Coronavirus (Covid N95, nCoV-2019, SARS-CoV 2, 2020 Outbreak)From EverandCoping with COVID-19: Practical and Efficient Ways on How to Prevent, Prepare, and Protect You and Your Family from the Wuhan Coronavirus (Covid N95, nCoV-2019, SARS-CoV 2, 2020 Outbreak)No ratings yet
- 16.science and Technology 3 Target - Prelims - 2020Document46 pages16.science and Technology 3 Target - Prelims - 2020naseerNo ratings yet
- 10 1016@j Oraloncology 2020 104821Document4 pages10 1016@j Oraloncology 2020 104821khamilatusyNo ratings yet
- Covid 19Document9 pagesCovid 19Ishita AhlawatNo ratings yet
- Novel Corona VirusDocument12 pagesNovel Corona VirusJasper Pagalan MartinezNo ratings yet
- Favipiravir 071120Document55 pagesFavipiravir 071120w5bwmbfrtwNo ratings yet
- 4A Group 3 Orthomyxoviridae, PoxviridaeDocument46 pages4A Group 3 Orthomyxoviridae, PoxviridaeLowella Rose C. DonguinesNo ratings yet
- Diagnosis and treatment of various types of coronavirus pneumonia of Sars disease and respiratory infectious diseases, and research on the source of infection of animal coronavirus pneumonia (Fang Ruida) Davis. KDocument39 pagesDiagnosis and treatment of various types of coronavirus pneumonia of Sars disease and respiratory infectious diseases, and research on the source of infection of animal coronavirus pneumonia (Fang Ruida) Davis. Kweld AdonisNo ratings yet
- Sample Coronavirus WorksheetsDocument9 pagesSample Coronavirus WorksheetsMyriam PitrelliNo ratings yet
- Novel Corona Virus (COVID-19)Document8 pagesNovel Corona Virus (COVID-19)Mohammad M Omar100% (1)
- COVID-19 Infection: Origin, Transmission, and Characteristics of Human CoronavirusesDocument10 pagesCOVID-19 Infection: Origin, Transmission, and Characteristics of Human CoronavirusesVeronicaNo ratings yet
- RNA Non Enveloped VirusesDocument35 pagesRNA Non Enveloped VirusesRPh Krishna Chandra JagritNo ratings yet
- Quality AssuranceDocument16 pagesQuality AssuranceArlyn MarcelinoNo ratings yet
- Updated Rubrics 2023 PDFDocument6 pagesUpdated Rubrics 2023 PDFArlyn MarcelinoNo ratings yet
- RLE DR CASES MarcelinoDocument8 pagesRLE DR CASES MarcelinoArlyn MarcelinoNo ratings yet
- Nursing Disaster1stDocument11 pagesNursing Disaster1stArlyn MarcelinoNo ratings yet
- Rle or Cases FormatDocument4 pagesRle or Cases FormatArlyn MarcelinoNo ratings yet
- NCMB418 Pet 2223Document2 pagesNCMB418 Pet 2223Arlyn MarcelinoNo ratings yet
- Week 8 CU 7 DN-M2-CU7 School Mitigation and Preparedness, Evaluation-2 - 1460360581 PDFDocument9 pagesWeek 8 CU 7 DN-M2-CU7 School Mitigation and Preparedness, Evaluation-2 - 1460360581 PDFArlyn MarcelinoNo ratings yet
- BioethicsDocument1 pageBioethicsArlyn MarcelinoNo ratings yet
- Eval Team Email and CertDocument1 pageEval Team Email and CertArlyn MarcelinoNo ratings yet
- Eval Team Email and CertDocument1 pageEval Team Email and CertArlyn MarcelinoNo ratings yet
- BioethicsDocument1 pageBioethicsArlyn MarcelinoNo ratings yet
- Jeffrey C. LucendoDocument2 pagesJeffrey C. LucendoArlyn MarcelinoNo ratings yet
- Untitled DocumentDocument2 pagesUntitled DocumentArlyn MarcelinoNo ratings yet
- Jeffrey C. LucendoDocument2 pagesJeffrey C. LucendoArlyn MarcelinoNo ratings yet
- Jeffrey C. LucendoDocument2 pagesJeffrey C. LucendoArlyn MarcelinoNo ratings yet
- BembemDocument2 pagesBembemArlyn MarcelinoNo ratings yet
- Jeffrey C. LucendoDocument2 pagesJeffrey C. LucendoArlyn MarcelinoNo ratings yet
- Jeffrey C. LucendoDocument2 pagesJeffrey C. LucendoArlyn MarcelinoNo ratings yet
- BioethicsDocument1 pageBioethicsArlyn MarcelinoNo ratings yet
- BembemDocument2 pagesBembemArlyn MarcelinoNo ratings yet
- BioethicsDocument1 pageBioethicsArlyn MarcelinoNo ratings yet
- BioethicsDocument1 pageBioethicsArlyn MarcelinoNo ratings yet
- Jeffrey C. LucendoDocument2 pagesJeffrey C. LucendoArlyn MarcelinoNo ratings yet
- BioethicsDocument1 pageBioethicsArlyn MarcelinoNo ratings yet
- BembemDocument2 pagesBembemArlyn MarcelinoNo ratings yet
- Jeffrey C. LucendoDocument2 pagesJeffrey C. LucendoArlyn MarcelinoNo ratings yet
- Tcwd111 Activity #4: BARONIA, Michael Jayron A. BSN2Y2-4SDocument1 pageTcwd111 Activity #4: BARONIA, Michael Jayron A. BSN2Y2-4SArlyn MarcelinoNo ratings yet
- Peds CardioDocument160 pagesPeds CardioArlyn MarcelinoNo ratings yet
- Pediatric NursingDocument291 pagesPediatric NursingArlyn MarcelinoNo ratings yet
- Family Survey From Emilyn Prieto: Arlyn Marcelino BSN 2Y1-4SDocument4 pagesFamily Survey From Emilyn Prieto: Arlyn Marcelino BSN 2Y1-4SArlyn MarcelinoNo ratings yet
- RNA VirusesDocument404 pagesRNA VirusesSisayNo ratings yet
- E ColiDocument2 pagesE ColiCamila Jackelyne Núñez SilvaNo ratings yet
- Brain InfectionDocument61 pagesBrain Infectionmanisha paikarayNo ratings yet
- 6075 Article Text 42975 1 10 20220630Document14 pages6075 Article Text 42975 1 10 20220630Laborat MenurNo ratings yet
- Objectives of Infection ControlDocument34 pagesObjectives of Infection ControlMoh Yousif100% (1)
- Argumentative PaperDocument4 pagesArgumentative PaperSamantha BugayongNo ratings yet
- Verify Gov SGDocument3 pagesVerify Gov SGWei Xi TeeNo ratings yet
- Principles of Antibiotic Formulary Selection For P&T Committees 1Document3 pagesPrinciples of Antibiotic Formulary Selection For P&T Committees 1madengNo ratings yet
- Research Title ProposalDocument15 pagesResearch Title ProposalLacangan, Thea YvonneNo ratings yet
- Communicable Disease NursingDocument44 pagesCommunicable Disease NursingFreeNursingNotes100% (17)
- Vaccination 710428115244Document1 pageVaccination 710428115244arleesyaNo ratings yet
- 7 Tips To Reduce Risk of CancerDocument2 pages7 Tips To Reduce Risk of Cancerjubilla mondanoNo ratings yet
- WHO Risk Assessment Template - Annex2Document7 pagesWHO Risk Assessment Template - Annex2Chester KyleNo ratings yet
- FILARIASISDocument57 pagesFILARIASISadekayo100% (6)
- Acquired Immune Deficiency Syndrome or Acquired Immunodeficiency Syndrome (AIDS) Is A Disease of The Human Immune System Caused byDocument7 pagesAcquired Immune Deficiency Syndrome or Acquired Immunodeficiency Syndrome (AIDS) Is A Disease of The Human Immune System Caused byAdrian MallarNo ratings yet
- Farmakologi Obat Kusta Dan Antiparasit 2015Document84 pagesFarmakologi Obat Kusta Dan Antiparasit 2015Alex FerdinandNo ratings yet
- HivDocument24 pagesHivLaxman KannaNo ratings yet
- Pediatric Community-Acquired Pneumonia: Nelson 20 EdDocument43 pagesPediatric Community-Acquired Pneumonia: Nelson 20 EdRazel Kinette AzotesNo ratings yet
- Chapter 1 (Causes For Dengue Outbreak)Document7 pagesChapter 1 (Causes For Dengue Outbreak)Miss WindamNo ratings yet
- Brief History of ImmunologyDocument5 pagesBrief History of Immunologyella SyNo ratings yet
- SACMC - 19052020 - Slides For MoHmediabriefingDocument21 pagesSACMC - 19052020 - Slides For MoHmediabriefingBranko Brkic93% (15)
- DiphtheriaDocument18 pagesDiphtheriaShishir ShresthaNo ratings yet
- Dengue, Leptospirosis, Malaria, InfluenzeDocument89 pagesDengue, Leptospirosis, Malaria, Influenzesarguss14100% (5)
- Pemodelan SistemDocument4 pagesPemodelan Sistembagus satyaNo ratings yet
- Quiz Public HealthDocument26 pagesQuiz Public HealthMedShare89% (27)
- Varicella-Zoster VaccineDocument14 pagesVaricella-Zoster VaccineftmahzahraNo ratings yet
- TEST I. Multiple Choice: Choose The Correct Answer and Write Only The Letter Before The NumberDocument2 pagesTEST I. Multiple Choice: Choose The Correct Answer and Write Only The Letter Before The Numberkanne100% (1)
- Tuberculosis VaccineDocument15 pagesTuberculosis Vaccinesatheeshpharma6No ratings yet
- Malaria Treatment Guideline 2012Document38 pagesMalaria Treatment Guideline 2012van_cristiano100% (3)
- MPX Social Gatherings Safer Sex-508Document2 pagesMPX Social Gatherings Safer Sex-508WDIV/ClickOnDetroitNo ratings yet