You might also like
- Epidemiology for Canadian Students: Principles, Methods and Critical AppraisalFrom EverandEpidemiology for Canadian Students: Principles, Methods and Critical AppraisalRating: 1 out of 5 stars1/5 (1)
- Cohort Study DesignDocument34 pagesCohort Study DesignErmiasNo ratings yet
- Cohort, 2007 StudyDocument46 pagesCohort, 2007 StudyUsman HamzaNo ratings yet
- Cohort Study 2 & 3Document28 pagesCohort Study 2 & 3Mongolian MutuNo ratings yet
- Research Methodolgy 2: Dr. Ahmed GhandourDocument29 pagesResearch Methodolgy 2: Dr. Ahmed Ghandourahmed tarekNo ratings yet
- Descriptive Study DesignDocument36 pagesDescriptive Study DesignAhmad ShalashNo ratings yet
- Analytic Epidemiology: By: Fisaha.H (Mphil)Document76 pagesAnalytic Epidemiology: By: Fisaha.H (Mphil)ruthNo ratings yet
- Cohort StudiesDocument110 pagesCohort StudiesArpita HalderNo ratings yet
- Cohort Study: Dr. Rahul Netragaonkar Associate ProfessorDocument37 pagesCohort Study: Dr. Rahul Netragaonkar Associate ProfessorRahul NetragaonkarNo ratings yet
- Epidemiologica L Studies: Epidemiology CHS234Document34 pagesEpidemiologica L Studies: Epidemiology CHS234اسامة محمد السيد رمضانNo ratings yet
- Epidemiological Methods: Prabha Krishnan, Year MSC Nursing, CNC, KKDDocument22 pagesEpidemiological Methods: Prabha Krishnan, Year MSC Nursing, CNC, KKDprabha krishnan100% (2)
- 2the Epidemiology-1Document37 pages2the Epidemiology-1محمد ربيعيNo ratings yet
- Epidemiology With Part 2 (Complete) 2Document59 pagesEpidemiology With Part 2 (Complete) 2nahNo ratings yet
- EpidemiologyDocument58 pagesEpidemiologyrebecca100% (4)
- Lecture 4 & 5. Epidemiological StudiesDocument58 pagesLecture 4 & 5. Epidemiological StudiesHaneen Al-HajjNo ratings yet
- Introduction PDFDocument29 pagesIntroduction PDFhadin khanNo ratings yet
- Cohort StudyDocument44 pagesCohort StudyShaimaa AbdulkadirNo ratings yet
- Cohort Studies 2022Document80 pagesCohort Studies 2022Marwa AlhajAhmadNo ratings yet
- Epidemiology Approach and MethodsDocument50 pagesEpidemiology Approach and MethodsBen PhiriNo ratings yet
- Epidemiological Methodology & Medical StatisticsDocument10 pagesEpidemiological Methodology & Medical StatisticsDina Saad EskandereNo ratings yet
- Observational Study DesignDocument25 pagesObservational Study DesignlenyNo ratings yet
- Observation Designs in EpidemiologyDocument20 pagesObservation Designs in EpidemiologyChristian JeffersonNo ratings yet
- Metlit-10 Studi Kohort - Prof. Dr. Sudigdo S, SpA (K)Document56 pagesMetlit-10 Studi Kohort - Prof. Dr. Sudigdo S, SpA (K)Laurencia LenyNo ratings yet
- Cohort StudyDocument46 pagesCohort Studymirabel IvanaliNo ratings yet
- Lecture 7 Study DesignsDocument86 pagesLecture 7 Study DesignsKhalil UllahNo ratings yet
- Epidemiological Study DesignsDocument60 pagesEpidemiological Study DesignsAnn Hill100% (1)
- Descriptive StudiesDocument38 pagesDescriptive StudiesMai MaiNo ratings yet
- Observational Studies I: Case Report, Case Series, Cross Sectional and Ecological StudiesDocument39 pagesObservational Studies I: Case Report, Case Series, Cross Sectional and Ecological StudiesMayson BaliNo ratings yet
- Methods Used in EpidemologyDocument53 pagesMethods Used in EpidemologySameera banuNo ratings yet
- Cohort StudyDocument40 pagesCohort Studyபிரேம் குமார் ராஜாமணிNo ratings yet
- Study DesignsDocument166 pagesStudy DesignsIsmail QamarNo ratings yet
- Community Medicine: Cross-Sectional Studies (Prevalence Studies/ Surveys)Document5 pagesCommunity Medicine: Cross-Sectional Studies (Prevalence Studies/ Surveys)api-3829364No ratings yet
- Disease Overview PDFDocument24 pagesDisease Overview PDFMeshal NoorNo ratings yet
- Descriptive Studies - May 2020Document42 pagesDescriptive Studies - May 2020kelgroryNo ratings yet
- Introduction To EpiderminologyDocument27 pagesIntroduction To Epiderminologyoncolo10% (1)
- 0 - Lecture 2 - Public Health - Studydesgin - Assiut2Document56 pages0 - Lecture 2 - Public Health - Studydesgin - Assiut2Nariman SternNo ratings yet
- Cohort DesignDocument41 pagesCohort DesignHope EkwensiNo ratings yet
- Intro To StatisticsDocument11 pagesIntro To StatisticsVincent KimaniNo ratings yet
- Submodule4 Epid Exprtl-Stdies Ver1 8nov2018Document39 pagesSubmodule4 Epid Exprtl-Stdies Ver1 8nov2018Mery Grace Barillo DelectorNo ratings yet
- Cohort Study 2021Document34 pagesCohort Study 2021Muhammad BilalNo ratings yet
- Epidemiologi Penilaian Risiko Penyakit BagusDocument45 pagesEpidemiologi Penilaian Risiko Penyakit Bagusvionaswa amanda ariandriNo ratings yet
- 3) DejeneDocument157 pages3) DejeneFoyye Merga GudetaNo ratings yet
- DILSHAD - Study DesignsDocument48 pagesDILSHAD - Study DesignsAamir IjazNo ratings yet
- AMA 4351 Statistical EpidemiologyDocument72 pagesAMA 4351 Statistical EpidemiologyRobinson WambuaNo ratings yet
- Overview of Epidemiologic StudiesDocument85 pagesOverview of Epidemiologic StudiesNathnael GebNo ratings yet
- Introduction To Epidemiology & Public Health: Dr. Munibullah LecturerDocument22 pagesIntroduction To Epidemiology & Public Health: Dr. Munibullah LecturerIbrar Faisal0% (1)
- Advance Epi & Direct Acyclic GraphDocument14 pagesAdvance Epi & Direct Acyclic GraphPurnima VermaNo ratings yet
- Submodule4 Epid Exprmntl-StudiesDocument15 pagesSubmodule4 Epid Exprmntl-StudiesPowell TabogocNo ratings yet
- Chapter 4 Epidemiological StudiesDocument52 pagesChapter 4 Epidemiological StudiesEstiv W. StigNo ratings yet
- FAMILY & COMMUNITY MEDICINE Summary NoteDocument3 pagesFAMILY & COMMUNITY MEDICINE Summary NoteANGELICA ADVIENTONo ratings yet
- PHR211Public Health: EpidemiologyDocument59 pagesPHR211Public Health: EpidemiologyNuhu SibaNo ratings yet
- 8 CohortDocument41 pages8 CohortSalma AzeemNo ratings yet
- CohortDocument48 pagesCohortJoel BharathNo ratings yet
- I. Observational Designs: Subsequent Literature and Possibly On Clinical Practice.'Document3 pagesI. Observational Designs: Subsequent Literature and Possibly On Clinical Practice.'Mohamed MoustafaNo ratings yet
- Basic EpidemiologyDocument16 pagesBasic EpidemiologyNeil Victor Ongco PajugotNo ratings yet
- Complete Notes STATSDocument16 pagesComplete Notes STATSsilvestre bolosNo ratings yet
- Study DesignDocument3 pagesStudy Designmusa onyango obuyaNo ratings yet
- Community MedicineDocument7 pagesCommunity Medicineapi-3829364No ratings yet
- Aula 1 TRNSV 290523Document44 pagesAula 1 TRNSV 290523Germaine Ingabire YengoNo ratings yet
- Organozatinal Buyer Behavior Chapter Case Block-2 Ch.9Document11 pagesOrganozatinal Buyer Behavior Chapter Case Block-2 Ch.9v_ratNo ratings yet
- Case Demand Measurement and Forecasting Block-2 Ch.4Document3 pagesCase Demand Measurement and Forecasting Block-2 Ch.4v_ratNo ratings yet
- Case On Brand Management Block-3 Ch.15Document3 pagesCase On Brand Management Block-3 Ch.15v_ratNo ratings yet
- Marketing Research Chapter Case Block-2 Ch.5Document4 pagesMarketing Research Chapter Case Block-2 Ch.5v_rat0% (1)
- Kingfisher Airlines Service Marketing Block-3 Ch.12Document4 pagesKingfisher Airlines Service Marketing Block-3 Ch.12nit_kharcheNo ratings yet
- Case Study Block-1 Ch. 1 PDFDocument2 pagesCase Study Block-1 Ch. 1 PDFv_ratNo ratings yet
- Case in Marketing Environment Block-2 Ch.6Document3 pagesCase in Marketing Environment Block-2 Ch.6v_ratNo ratings yet
- The Selection of Essential MedicinesDocument6 pagesThe Selection of Essential MedicinesJoseph Antonio A. GomezNo ratings yet
- of E-Aushadi FinalDocument48 pagesof E-Aushadi Finalv_ratNo ratings yet
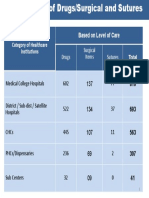
- Category of Healthcare Institutions Based On Level of Care: Drugs Surgical Items SuturesDocument1 pageCategory of Healthcare Institutions Based On Level of Care: Drugs Surgical Items Suturesv_ratNo ratings yet
- Globalization, TRIPS and Access To Pharmaceuticals: in Global TradeDocument6 pagesGlobalization, TRIPS and Access To Pharmaceuticals: in Global Tradev_ratNo ratings yet
- Equitable Access To Essential Medicines: A Framework For Collective ActionDocument6 pagesEquitable Access To Essential Medicines: A Framework For Collective Actionv_ratNo ratings yet
- RUM July 2011Document2 pagesRUM July 2011v_ratNo ratings yet
- Access To Quality Medicines: Rajasthan Model: "Reaching The Unreached"Document7 pagesAccess To Quality Medicines: Rajasthan Model: "Reaching The Unreached"v_ratNo ratings yet
- Drugs Store Management: Dr. Nirmal GurbaniDocument94 pagesDrugs Store Management: Dr. Nirmal Gurbaniv_ratNo ratings yet
- Day 8 Inventory ManagementDocument56 pagesDay 8 Inventory Managementv_ratNo ratings yet
- Quantification of Health Commodities - RMNCH SupplementDocument173 pagesQuantification of Health Commodities - RMNCH Supplementv_ratNo ratings yet
- Routine Immunization Immunization Handbook For Medical OfficersDocument200 pagesRoutine Immunization Immunization Handbook For Medical Officersubaid21100% (1)
- Inv. Mgt. Procurement & DistributionDocument78 pagesInv. Mgt. Procurement & Distributionv_ratNo ratings yet
- Logistics HandbookDocument174 pagesLogistics HandbookNeel KanthNo ratings yet
- UNFPA RFQ QA Framework - Low - V11Document32 pagesUNFPA RFQ QA Framework - Low - V11v_ratNo ratings yet
- Day 4 - CQI in Stores ManagementDocument8 pagesDay 4 - CQI in Stores Managementv_ratNo ratings yet
- Day 3 - Equipment Disposal, Audit, T&DDocument35 pagesDay 3 - Equipment Disposal, Audit, T&Dv_ratNo ratings yet
- A Strategic Essential in Healthcare Systems OutsourcingDocument22 pagesA Strategic Essential in Healthcare Systems Outsourcingv_ratNo ratings yet
- Day 4 - ReliabilityDocument11 pagesDay 4 - Reliabilityv_ratNo ratings yet
- Day 2 - Equipment Preventive MaintenanceDocument29 pagesDay 2 - Equipment Preventive Maintenancev_ratNo ratings yet
- Day 1 - Equipment-Mohan-1Document22 pagesDay 1 - Equipment-Mohan-1v_ratNo ratings yet
- Day 4 - CQI in Stores ManagementDocument8 pagesDay 4 - CQI in Stores Managementv_ratNo ratings yet
- Logistics Management Information Systems (LMIS)Document25 pagesLogistics Management Information Systems (LMIS)v_ratNo ratings yet
- Ias 19Document41 pagesIas 19mohedNo ratings yet
- Utility Indifference Curves For RiskDocument3 pagesUtility Indifference Curves For RiskAmit GuptaNo ratings yet
- Customer DataDocument18 pagesCustomer Datawidya615No ratings yet
- Data - Q1 (Version 1)Document15 pagesData - Q1 (Version 1)baselzayied23No ratings yet
- MSC TextbookDocument70 pagesMSC TextbookNguyễn Thanh VũNo ratings yet
- Stats Chap 1 TheoryDocument11 pagesStats Chap 1 TheoryNeejan JackNo ratings yet
- Overview Manajemen Risiko - DikonversiDocument27 pagesOverview Manajemen Risiko - DikonversiKusnadi CilukNo ratings yet
- Influential ObservationDocument4 pagesInfluential Observationsophia787No ratings yet
- Insurance Brokers in MumbaiDocument8 pagesInsurance Brokers in MumbaiAbhishek MoreNo ratings yet
- Logistic RegressionDocument8 pagesLogistic RegressionBeatriz RodriguesNo ratings yet
- Stats Modeling The World 4th Edition Bock Test BankDocument48 pagesStats Modeling The World 4th Edition Bock Test Bankselinaanhon9a100% (24)
- Biostatistics - Part 8A - DR - Vennila JDocument22 pagesBiostatistics - Part 8A - DR - Vennila JIts AnythingNo ratings yet
- Ref Ni Term PaperDocument2 pagesRef Ni Term PaperqwertyNo ratings yet
- Demographic Changein India Isthe Country Preparedforthe ChallengesDocument21 pagesDemographic Changein India Isthe Country Preparedforthe ChallengesRiju PrasadNo ratings yet
- 33 Annual Giro Convention: Hilton Vienna Hotel, Am StadtparkDocument32 pages33 Annual Giro Convention: Hilton Vienna Hotel, Am Stadtparkskywalk189No ratings yet
- Materi 5.1-Inference in Simple Linear RegressionDocument15 pagesMateri 5.1-Inference in Simple Linear RegressionarismansyahNo ratings yet
- Biostatistics PSM RecordDocument18 pagesBiostatistics PSM Record76zw5n4pppNo ratings yet
- Exam HandbookDocument102 pagesExam HandbookSyed AmeenNo ratings yet
- Top Reasons Why The Retirement Age Be Lowered From 60 To 56Document4 pagesTop Reasons Why The Retirement Age Be Lowered From 60 To 56Lea UnderscoreNo ratings yet
- Capm From CcapmDocument3 pagesCapm From CcapmNigelT.LeeNo ratings yet
- Master's Degrees: Bayes Business School (Formerly Cass)Document22 pagesMaster's Degrees: Bayes Business School (Formerly Cass)saksham sondhiNo ratings yet
- Topic Presentation 7Document58 pagesTopic Presentation 7Mary ThereseNo ratings yet
- Econometrics - Qualitative Response ModelsDocument17 pagesEconometrics - Qualitative Response ModelsalvarezxpatriciaNo ratings yet
- Mathematics of Investments - Ordinary Simple AnnuitiesDocument2 pagesMathematics of Investments - Ordinary Simple AnnuitiesBrando MoloNo ratings yet
- Vital StatisticsDocument14 pagesVital StatisticsLikith GNo ratings yet
- Materi Dokter Bayu TGL 9 Juli 2020Document53 pagesMateri Dokter Bayu TGL 9 Juli 2020humaira noorNo ratings yet
- MEABF Plan Design Scenarios - September 6, 2016Document8 pagesMEABF Plan Design Scenarios - September 6, 2016The Daily LineNo ratings yet
- TMV Practice Questions SolutionsDocument20 pagesTMV Practice Questions SolutionsSnehNo ratings yet
- ERM and QRM in Life InsuranceDocument236 pagesERM and QRM in Life InsuranceLoic MawetNo ratings yet
- Lesson 6.2 Correlation and Regression Analysis Final EditionDocument8 pagesLesson 6.2 Correlation and Regression Analysis Final EditionJeline Flor EugenioNo ratings yet