You might also like
- Community Based RehabilitationDocument11 pagesCommunity Based RehabilitationDebipriya Mistry75% (4)
- Community Based RehabilitationDocument13 pagesCommunity Based RehabilitationBabita Dhruw50% (2)
- Community Based Rehabilitation (CBR) : ArticipationDocument6 pagesCommunity Based Rehabilitation (CBR) : ArticipationPooja YadavNo ratings yet
- Extension Services and Mobile UnitsDocument27 pagesExtension Services and Mobile UnitsNaveen Kumar100% (2)
- 1 National District Level Rehabilitation Programm BPT Final Year PDFDocument9 pages1 National District Level Rehabilitation Programm BPT Final Year PDFChihual Murdia100% (5)
- Need For CBRDocument28 pagesNeed For CBRNaveen Kumar100% (1)
- History of CBRDocument15 pagesHistory of CBRkim100% (3)
- District Disability Rehabilitation CentreDocument22 pagesDistrict Disability Rehabilitation Centreshodhganga100% (4)
- Community Based Rehabilitation PDFDocument2 pagesCommunity Based Rehabilitation PDFJoey17% (6)
- Members of CBR TeamDocument14 pagesMembers of CBR TeamJeffery Samuel100% (4)
- Brachial Plexus InjuriesDocument32 pagesBrachial Plexus InjuriesFatima yasin50% (2)
- Difference Between Institution Based and Community Based RehabilitationDocument2 pagesDifference Between Institution Based and Community Based Rehabilitationshruti95% (22)
- Industrial TherapyDocument29 pagesIndustrial TherapyMalu100% (1)
- Lec 9 Trick MovementsDocument19 pagesLec 9 Trick MovementsBhargav69% (13)
- CBR and Multidisciplinary Approach-Definition, Models of Multidisciplinary CBR, Recent AdvancesDocument29 pagesCBR and Multidisciplinary Approach-Definition, Models of Multidisciplinary CBR, Recent Advancesmayuri zanwar100% (1)
- CBR InformationDocument24 pagesCBR Informationamitesh_mpthNo ratings yet
- Community Based RehabilitationDocument8 pagesCommunity Based RehabilitationNaveen Kumar100% (1)
- Disability EvaluationDocument11 pagesDisability Evaluationramhariphysio63% (8)
- Scope of Physiotherapy Practice in Community and HealthDocument34 pagesScope of Physiotherapy Practice in Community and Healthtafela67% (6)
- Physiotherapy in General Surgical ConditionDocument7 pagesPhysiotherapy in General Surgical Conditionprofpt98100% (8)
- Extension Services and Mobile Health UnitDocument23 pagesExtension Services and Mobile Health UnitKandi IssayaNo ratings yet
- The Guiding Principles of CBRDocument5 pagesThe Guiding Principles of CBRLadylyn BrazaNo ratings yet
- Community Based Rehabilitation of Persons With DisabilitiesDocument234 pagesCommunity Based Rehabilitation of Persons With DisabilitiesDr. meghna jain68% (19)
- Motor Relearning ProgramDocument10 pagesMotor Relearning ProgramjalykAmazing75% (4)
- Re Education of MusclesDocument41 pagesRe Education of MusclesMohamed Magdy El Meligie0% (3)
- Spinal Cord Injury - Physical Therapy ManagementDocument86 pagesSpinal Cord Injury - Physical Therapy Managementphysiovipin96% (70)
- Ommunity Ased EhabilitationDocument43 pagesOmmunity Ased Ehabilitationbipinarora100% (3)
- Physiotherapy Management of Vascular DisordersDocument55 pagesPhysiotherapy Management of Vascular DisordersAkheel AhammedNo ratings yet
- The Role of Physiotherapy in RehabilitationDocument5 pagesThe Role of Physiotherapy in Rehabilitationari_alianiNo ratings yet
- The Indian Association of Physiotherapists - IAP Constitutions PDFDocument17 pagesThe Indian Association of Physiotherapists - IAP Constitutions PDFHasan Rahman100% (1)
- Tendon Transfers - RehabilitationDocument4 pagesTendon Transfers - RehabilitationPankaj Malik100% (4)
- Rood's ApproachDocument11 pagesRood's ApproachRajveer100% (1)
- Clinical Decision Making in Electrotherapeutics and Safety ConsiderationsDocument87 pagesClinical Decision Making in Electrotherapeutics and Safety Considerationsmayuri zanwar100% (1)
- Motor Relearning Programme: Prepared by Mohammad Bin Afsar JanDocument11 pagesMotor Relearning Programme: Prepared by Mohammad Bin Afsar Jankashmala afzal100% (1)
- Roods ApproachDocument23 pagesRoods ApproachyigoNo ratings yet
- Community and Government RoleDocument47 pagesCommunity and Government RoleBasayya SwamyNo ratings yet
- Principles of MRPDocument24 pagesPrinciples of MRPShriya100% (1)
- Vojta TherapyDocument4 pagesVojta TherapyPrashu Jain100% (1)
- Role of Social Workers in RehabilitationDocument45 pagesRole of Social Workers in RehabilitationPatie N Tome100% (2)
- Mat ActivitiesDocument20 pagesMat Activitiesmuthuu60% (5)
- PepDocument8 pagesPepUdayakrishnan P Kanhangad100% (1)
- FG TestDocument24 pagesFG TestIndira Naidu Boddapati83% (29)
- Traumatic Brain Injury Physiotherapy AssessmentDocument20 pagesTraumatic Brain Injury Physiotherapy AssessmentNithin Nair100% (1)
- Rebox CurrentsDocument38 pagesRebox CurrentsProtantagonist75% (4)
- Cyclo ThermDocument24 pagesCyclo ThermProtantagonist91% (11)
- Faradic Foot BathDocument1 pageFaradic Foot BathJohn Ribu Parampil70% (10)
- Model Test Paper For MPT Entrance ExaminationsDocument4 pagesModel Test Paper For MPT Entrance Examinationspratik231081% (26)
- Neurological Physiotherapy Evaluation FormDocument13 pagesNeurological Physiotherapy Evaluation FormShruti100% (10)
- Sumibikovobe Joint Structure and Function by Cynthia Norkin PDF Download PagutaxegokagDocument4 pagesSumibikovobe Joint Structure and Function by Cynthia Norkin PDF Download Pagutaxegokagrock star100% (1)
- Physiotherapy in DermatologyDocument18 pagesPhysiotherapy in DermatologyPraisy Roy67% (3)
- Active MovementsDocument32 pagesActive MovementsFaiqa Sheikh100% (1)
- Lec 9active & Passive InsufficiencyDocument32 pagesLec 9active & Passive InsufficiencySajida Bibi Noonari75% (4)
- PT Management of Restrictive Lung DiseaseDocument16 pagesPT Management of Restrictive Lung DiseaseSiva Shanmugam25% (4)
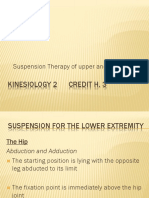
- Suspension Therapy of Upper and Lower LimbDocument23 pagesSuspension Therapy of Upper and Lower LimbM Farrukh shahzad100% (6)
- INTRO To CBR-1Document35 pagesINTRO To CBR-1EmanNo ratings yet
- Health Promotion For Elders in Nicaragua A Community-Based Rehabilitation ApproachDocument2 pagesHealth Promotion For Elders in Nicaragua A Community-Based Rehabilitation ApproachBhavaniNo ratings yet
- Desc - CBRPDocument1 pageDesc - CBRPAsyed Silayan ZaportizaNo ratings yet
- Community-Based Rehabilitation (CBR) : By, Abhishek Verma M.Sc. NSG II YrDocument34 pagesCommunity-Based Rehabilitation (CBR) : By, Abhishek Verma M.Sc. NSG II YrAbhishek VermaNo ratings yet
- Jessy CBRDocument10 pagesJessy CBRberocan jescaNo ratings yet
- Community Based Rehabilitation ProgramDocument13 pagesCommunity Based Rehabilitation ProgramProserfina MagdadaroNo ratings yet
- Tennis ElbowDocument6 pagesTennis ElbowAkshay BangadNo ratings yet
- Chest Physiotherapy For Mechanical Ventilation PatientDocument6 pagesChest Physiotherapy For Mechanical Ventilation PatientAkshay BangadNo ratings yet
- Exercise in DiabetesDocument77 pagesExercise in DiabetesAkshay BangadNo ratings yet
- Osteoarthritis: A Holistic Approach: Andrew Barr and Philip G ConaghanDocument3 pagesOsteoarthritis: A Holistic Approach: Andrew Barr and Philip G ConaghanAkshay BangadNo ratings yet
- CBR Strategies (Ankita 2)Document25 pagesCBR Strategies (Ankita 2)Akshay BangadNo ratings yet
- Evaluation of Aerobic CapacityDocument20 pagesEvaluation of Aerobic CapacityAkshay BangadNo ratings yet
- Balance and Falls in ElderlyDocument36 pagesBalance and Falls in ElderlyAkshay BangadNo ratings yet
- Ergonomics: Pallavi WakodeDocument49 pagesErgonomics: Pallavi WakodeAkshay BangadNo ratings yet
- Ergonomics of Lifting and HandlingDocument70 pagesErgonomics of Lifting and HandlingAkshay BangadNo ratings yet
- CHN (All Questions and Scenario Put Into Your Mind That You Are Currently at The Community Doing Health Teaching)Document2 pagesCHN (All Questions and Scenario Put Into Your Mind That You Are Currently at The Community Doing Health Teaching)Vincent AmitNo ratings yet
- Ams PHC Mop FinalDocument77 pagesAms PHC Mop FinalCNCMH LOONNo ratings yet
- India BlockCDocument13 pagesIndia BlockCArvin O-CaféNo ratings yet
- Health Care Services in IndiaDocument53 pagesHealth Care Services in Indiasasmita nayak100% (1)
- Primary Care (PC) and Primary Health Care (PHC) : What Is The Difference?Document3 pagesPrimary Care (PC) and Primary Health Care (PHC) : What Is The Difference?keshyaNo ratings yet
- Health Care System in PakistanDocument20 pagesHealth Care System in PakistanSobia50% (2)
- CHN 2 SET A (Key Answers)Document7 pagesCHN 2 SET A (Key Answers)Marie Ordonia de Pona100% (1)
- Primary Health Care in IndiaDocument11 pagesPrimary Health Care in IndiaKailash NagarNo ratings yet
- 5 Year PlanDocument61 pages5 Year PlanNeethu Vincent50% (2)
- NCM 210 LECT - Primary Health CareDocument7 pagesNCM 210 LECT - Primary Health CareLYRIZZA LEA BHEA DESIATANo ratings yet
- Handouts CHNDocument23 pagesHandouts CHNJames Eugene CaasiNo ratings yet
- CHN Review NotesDocument10 pagesCHN Review NotesCerezo, Cherrieus Ann C.No ratings yet
- CHN Reviewer - BulletsDocument2 pagesCHN Reviewer - BulletsYan Vencer100% (1)
- (Original Article) Assessment of The Role of Community Health Volunteers in Delivering Primary Health Care in Manila, The PhilippinesDocument11 pages(Original Article) Assessment of The Role of Community Health Volunteers in Delivering Primary Health Care in Manila, The Philippinesalfeo AlfecheNo ratings yet
- Case Study OlfuDocument34 pagesCase Study OlfuElaine Joy O. ApostolNo ratings yet
- Pamantasan NG Cabuyao: College of NursingDocument78 pagesPamantasan NG Cabuyao: College of NursingissaiahnicolleNo ratings yet
- Foundations To Health Care ReviewerDocument14 pagesFoundations To Health Care Reviewergabrielle annNo ratings yet
- Vision 18Document1 pageVision 18rajanivkNo ratings yet
- Ideal Hospital Realisation and Maintenance Framework Manual 2018Document262 pagesIdeal Hospital Realisation and Maintenance Framework Manual 2018Finger Tladi100% (1)
- Unit Iv: Community Health Nursing Approaches, Concepts and Roles and Responsibilities of Nursing PersonnelDocument17 pagesUnit Iv: Community Health Nursing Approaches, Concepts and Roles and Responsibilities of Nursing Personnelkles insgkkNo ratings yet
- Board of Nursing New SyllabusDocument10 pagesBoard of Nursing New SyllabuswilbertantoninoNo ratings yet
- Lecture 2 - Primary Health CareDocument5 pagesLecture 2 - Primary Health CareAlannes AndalNo ratings yet
- CHN ReviewerDocument13 pagesCHN ReviewerCrizle Ellen BalbinNo ratings yet
- Primary Health CareDocument41 pagesPrimary Health CareKailash NagarNo ratings yet
- Primary Health Centre ReportDocument12 pagesPrimary Health Centre ReportAkshay H.100% (1)
- Transform Primary Health CareDocument80 pagesTransform Primary Health CareMohammed Siraj100% (1)
- English For Nurse 2019Document151 pagesEnglish For Nurse 2019TriianaaNo ratings yet
- CHN Lec Finals ReviewerDocument23 pagesCHN Lec Finals ReviewerMarron Jane GanoticeNo ratings yet
- National Rural Health Mission: State of Public HealthDocument15 pagesNational Rural Health Mission: State of Public HealthPreeti DagarNo ratings yet
- 2023 NCM 104 Coursepack 2Document53 pages2023 NCM 104 Coursepack 2russel pagadorNo ratings yet