You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Case Study OsteoporosisDocument17 pagesCase Study Osteoporosistarikeops50% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Osteonecrosis JawDocument13 pagesOsteonecrosis JawtarikeopsNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Effect of Fat Mass On Bone Mineral Density in Postmenopausal WomenDocument29 pagesEffect of Fat Mass On Bone Mineral Density in Postmenopausal WomentarikeopsNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Osteoporosis Diagnosis 2Document8 pagesOsteoporosis Diagnosis 2tarikeopsNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Risk FcatorsDocument56 pagesRisk FcatorstarikeopsNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Perc. Pantalar FusionDocument78 pagesPerc. Pantalar FusiontarikeopsNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- OsteoDocument36 pagesOsteotarikeopsNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Femeroacetabular Impingement (FAI) A Precursor of Hip OsteoarthritisDocument69 pagesFemeroacetabular Impingement (FAI) A Precursor of Hip OsteoarthritistarikeopsNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Osteoporosis and Osteoarthritis 2011 ConferenceDocument39 pagesOsteoporosis and Osteoarthritis 2011 ConferencetarikeopsNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Osteopoorosis Cairo April 2011 v1Document33 pagesOsteopoorosis Cairo April 2011 v1tarikeopsNo ratings yet
- 1-Dr. Samir El BadawyDocument83 pages1-Dr. Samir El BadawytarikeopsNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- BroshureDocument3 pagesBroshuretarikeopsNo ratings yet
- Osteoarthritis and Osteoporosis 2Document38 pagesOsteoarthritis and Osteoporosis 2tarikeopsNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Targeted Therapies in Osteoarthritis.: by Prof. Samir ElbadawyDocument70 pagesTargeted Therapies in Osteoarthritis.: by Prof. Samir ElbadawytarikeopsNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
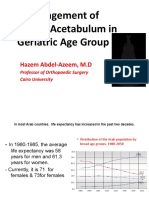
- Management of Fracture Acetabulum in Geriatric Age Group Saturday 12 15Document44 pagesManagement of Fracture Acetabulum in Geriatric Age Group Saturday 12 15tarikeopsNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- شهادةDocument52 pagesشهادةtarikeopsNo ratings yet
- Women Health: Theory & Practice The GapDocument57 pagesWomen Health: Theory & Practice The GaptarikeopsNo ratings yet
- Radio Logical Assessment of OA FinalDocument60 pagesRadio Logical Assessment of OA FinaltarikeopsNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Health Believes and OsteoporosisDocument31 pagesHealth Believes and OsteoporosistarikeopsNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- ورقة تقديمDocument3 pagesورقة تقديمtarikeopsNo ratings yet
- Post Menopausal Osteoporosis in Egypt DR RashedDocument24 pagesPost Menopausal Osteoporosis in Egypt DR RashedtarikeopsNo ratings yet
- Program 2011Document4 pagesProgram 2011tarikeopsNo ratings yet
- Osteoporosis Prevention DR Moh HasanDocument22 pagesOsteoporosis Prevention DR Moh HasantarikeopsNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Icivics MontesquieuDocument3 pagesIcivics Montesquieuapi-32806152578% (9)
- Docshare - Tips Upstream Advanced c1 Test BookletDocument3 pagesDocshare - Tips Upstream Advanced c1 Test BookletCosmin OaieNo ratings yet
- Filters SlideDocument17 pagesFilters SlideEmmanuel OkoroNo ratings yet
- Sampling Strategies For Heterogeneous WastesDocument18 pagesSampling Strategies For Heterogeneous Wastesmohammed karasnehNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- YCAP 7 Steps PosterDocument1 pageYCAP 7 Steps PosterSohila AmrNo ratings yet
- Javier Guzman v. City of Cranston, 812 F.2d 24, 1st Cir. (1987)Document4 pagesJavier Guzman v. City of Cranston, 812 F.2d 24, 1st Cir. (1987)Scribd Government DocsNo ratings yet
- Midterm Examination: General MathematicsDocument5 pagesMidterm Examination: General MathematicsJenalyn CardanoNo ratings yet
- Ruchika Project ReportDocument28 pagesRuchika Project Reportnavdeep2309No ratings yet
- Derivative Analysis HW1Document3 pagesDerivative Analysis HW1RahulSatijaNo ratings yet
- Module 1 Lesson 1 Activity and Analysis: Special Needs EducationDocument2 pagesModule 1 Lesson 1 Activity and Analysis: Special Needs EducationShalyn ArimaoNo ratings yet
- Technology in EducationDocument3 pagesTechnology in EducationDinesh MadhavanNo ratings yet
- Academic Calendar 2019-20 Odd Semester PDFDocument1 pageAcademic Calendar 2019-20 Odd Semester PDFPiyush ManwaniNo ratings yet
- Grade 3 MathematicsDocument3 pagesGrade 3 Mathematicsailaine grace alapNo ratings yet
- Gein, EdDocument10 pagesGein, Edpetru_k1No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Revised Market Making Agreement 31.03Document13 pagesRevised Market Making Agreement 31.03Bhavin SagarNo ratings yet
- Demonstration MethodDocument16 pagesDemonstration Methodfrankie aguirreNo ratings yet
- Per User Guide and Logbook2Document76 pagesPer User Guide and Logbook2Anthony LawNo ratings yet
- Quiz Simple Present Simple For Elementary To Pre-IntermediateDocument2 pagesQuiz Simple Present Simple For Elementary To Pre-IntermediateLoreinNo ratings yet
- The Divine Liturgy Syro Malankara ChurchDocument4 pagesThe Divine Liturgy Syro Malankara ChurchGian Marco TallutoNo ratings yet
- Compilation 2Document28 pagesCompilation 2Smit KhambholjaNo ratings yet
- NyirabahireS Chapter5 PDFDocument7 pagesNyirabahireS Chapter5 PDFAndrew AsimNo ratings yet
- LAAG4 Elementary Row Operations-3Document14 pagesLAAG4 Elementary Row Operations-3Kamran AliNo ratings yet
- Introduction To Consumer Behavior: by Dr. Kevin Lance JonesDocument18 pagesIntroduction To Consumer Behavior: by Dr. Kevin Lance JonesCorey PageNo ratings yet
- TENSES ExerciseDocument28 pagesTENSES ExerciseKhanh PhamNo ratings yet
- Alien Cicatrix II (Part 02 of 03) - The CloningDocument4 pagesAlien Cicatrix II (Part 02 of 03) - The CloningC.O.M.A research -stopalienabduction-No ratings yet
- Advanced Finite Element Model of Tsing Ma Bridge For Structural Health MonitoringDocument32 pagesAdvanced Finite Element Model of Tsing Ma Bridge For Structural Health MonitoringZhang ChaodongNo ratings yet
- Muslimah's Handbook of PurityDocument60 pagesMuslimah's Handbook of PurityMuadh KhanNo ratings yet
- MATH3161 MATH5165 T1 2023 OutlineDocument10 pagesMATH3161 MATH5165 T1 2023 OutlineDouglusNo ratings yet
- I. Revised Penal Code (RPC) and Related Special Laws: Riminal AWDocument11 pagesI. Revised Penal Code (RPC) and Related Special Laws: Riminal AWMc Vharn CatreNo ratings yet
- Thompson VarelaDocument18 pagesThompson VarelaGiannis NinosNo ratings yet
- The House at Pooh Corner - Winnie-the-Pooh Book #4 - UnabridgedFrom EverandThe House at Pooh Corner - Winnie-the-Pooh Book #4 - UnabridgedRating: 4.5 out of 5 stars4.5/5 (5)
- The Importance of Being Earnest: Classic Tales EditionFrom EverandThe Importance of Being Earnest: Classic Tales EditionRating: 4.5 out of 5 stars4.5/5 (44)
- You Can't Joke About That: Why Everything Is Funny, Nothing Is Sacred, and We're All in This TogetherFrom EverandYou Can't Joke About That: Why Everything Is Funny, Nothing Is Sacred, and We're All in This TogetherNo ratings yet