You might also like
- Holistic Medicine PDFDocument117 pagesHolistic Medicine PDFGaurav Bhaskar100% (1)
- Forces Affecting OBDocument6 pagesForces Affecting OBShashank BundelNo ratings yet
- Nursiing Management WR. Whole PackageDocument24 pagesNursiing Management WR. Whole Packageeyna30No ratings yet
- Nurses Ethical Considerations in A Pandemic or Other EmergencyDocument12 pagesNurses Ethical Considerations in A Pandemic or Other EmergencydavidNo ratings yet
- Protein Energy MalnutritionDocument44 pagesProtein Energy Malnutritionokwadha simionNo ratings yet
- Decision MakingDocument20 pagesDecision MakingAshutosh SinghNo ratings yet
- Prepared by Dr. Anees Alsaadi: CMT-P R4Document50 pagesPrepared by Dr. Anees Alsaadi: CMT-P R4Tayyba AzharNo ratings yet
- Management by Objectives (MBO)Document3 pagesManagement by Objectives (MBO)santhoshcmf50% (2)
- 2017 HELPER Guidelines PDFDocument79 pages2017 HELPER Guidelines PDFJames E BeyNo ratings yet
- Theories of ManagementDocument9 pagesTheories of Managementbaby100% (1)
- Expanded Program On ImmunizationDocument7 pagesExpanded Program On ImmunizationGLadys Gegare100% (1)
- Concept of HealthDocument20 pagesConcept of HealthMOZAIDNo ratings yet
- Child in The Family and Community RevisedDocument22 pagesChild in The Family and Community Revisedokwadha simionNo ratings yet
- Neonatal Sepsis LectureDocument142 pagesNeonatal Sepsis Lectureokwadha simion0% (1)
- Perinatal Asphyxia - Outline of Pathophysiology and Recent Trends in ManagementDocument31 pagesPerinatal Asphyxia - Outline of Pathophysiology and Recent Trends in Managementokwadha simionNo ratings yet
- BudgetDocument12 pagesBudgetDr. Jayesh PatidarNo ratings yet
- M.pharm SyllabusDocument47 pagesM.pharm SyllabustusharphaleNo ratings yet
- Chapter 23 Managing Quality and RiskDocument7 pagesChapter 23 Managing Quality and RiskLorene Reynolds100% (1)
- Health Care Delivery SystemDocument8 pagesHealth Care Delivery Systemnimila gopiNo ratings yet
- Organizing:, RN, Man ProfessorDocument68 pagesOrganizing:, RN, Man Professorailyn pinedaNo ratings yet
- Individual Growth and DevelopmentDocument23 pagesIndividual Growth and DevelopmentSujatha J Jayabal100% (1)
- Fundamentals of Health Services Administration (2)Document29 pagesFundamentals of Health Services Administration (2)Munashe MupereriNo ratings yet
- A Training Program in Community-Directed Intervention To Improve Access To Essential Health Services Training GuideDocument48 pagesA Training Program in Community-Directed Intervention To Improve Access To Essential Health Services Training GuideBushra AlMakaleh100% (1)
- 6 Decision MakingDocument28 pages6 Decision MakingMajd MustafaNo ratings yet
- Characteristics of EmotionsDocument9 pagesCharacteristics of EmotionsMANICANo ratings yet
- Importance of Effective Communication in Interpersonal RelationshipsDocument12 pagesImportance of Effective Communication in Interpersonal RelationshipsThe Shining100% (1)
- 20160316142348planning Commission and Niti AayogDocument17 pages20160316142348planning Commission and Niti AayogPavithra MurugesanNo ratings yet
- Health Promotion and EducationDocument75 pagesHealth Promotion and EducationDaniel DubeNo ratings yet
- Management by Objectives & Role Play: Presented By: Mridul AggarwalDocument16 pagesManagement by Objectives & Role Play: Presented By: Mridul Aggarwaladihind100% (1)
- Aseptic Technique ChecklistDocument11 pagesAseptic Technique ChecklistAsiah IsmailNo ratings yet
- Budgeting in Health Care System in IndiaDocument16 pagesBudgeting in Health Care System in IndiaABINASHNo ratings yet
- Fourteen Principles of Administration by Henri FayolDocument2 pagesFourteen Principles of Administration by Henri FayolanushavergheseNo ratings yet
- History of NursingDocument3 pagesHistory of NursingMark ClarenceNo ratings yet
- Kotebe Metropolitan University Menelik Ii Medical and Healthscience CollegeDocument25 pagesKotebe Metropolitan University Menelik Ii Medical and Healthscience Collegezeyneb pinkNo ratings yet
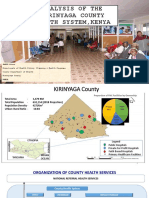
- Analysis of The Kirinyaga County Health System - Esbon - GakuuDocument18 pagesAnalysis of The Kirinyaga County Health System - Esbon - Gakuuesbon gakuu100% (1)
- NURSING MANAGEMENT AND ADMINISTRATION-feb2022Document42 pagesNURSING MANAGEMENT AND ADMINISTRATION-feb2022IGA ABRAHAM100% (1)
- Ageing Process and Physiological ChangesDocument23 pagesAgeing Process and Physiological ChangesAndreea MocanuNo ratings yet
- COPARDocument26 pagesCOPARCamz Canlas100% (1)
- Group BehaviourDocument15 pagesGroup BehaviourCg RajuNo ratings yet
- ProposalDocument22 pagesProposalbegosewNo ratings yet
- Introduction To NutritionDocument19 pagesIntroduction To Nutritionseanne kskwkwkaNo ratings yet
- Unit1 ManagementDocument24 pagesUnit1 ManagementAkshat KalaNo ratings yet
- Unit 12 CHNDocument12 pagesUnit 12 CHNadhikarisujataNo ratings yet
- Vijaya College of Nursing: Course Subject Unit Bio-Psycho Social PathophysiologyDocument3 pagesVijaya College of Nursing: Course Subject Unit Bio-Psycho Social PathophysiologyReshma Rinu50% (2)
- Planning (Management)Document8 pagesPlanning (Management)Sahil QaiserNo ratings yet
- NA 2 OrganizationDocument41 pagesNA 2 OrganizationAbilain Tuazon LiwanagNo ratings yet
- Subject: Basics of HRM Assignment 4: (Solution)Document4 pagesSubject: Basics of HRM Assignment 4: (Solution)vishal sinhaNo ratings yet
- Management TheoryDocument15 pagesManagement TheoryMerin sunilNo ratings yet
- Primary Health CareDocument2 pagesPrimary Health CareShamsa RiazNo ratings yet
- The Code of Ethics For Registered Nurses in The PhilippinesDocument6 pagesThe Code of Ethics For Registered Nurses in The PhilippinesDarla SaulerNo ratings yet
- Resources For Human HealthDocument56 pagesResources For Human Healthnapema.educ4790No ratings yet
- Health Administration NewDocument10 pagesHealth Administration NewjessyNo ratings yet
- Universal Health Coverage of Bangladesh - Analysis Through The Framework of Alford's Theory of Structural Interests in Health Care PPT 28 PresentedDocument30 pagesUniversal Health Coverage of Bangladesh - Analysis Through The Framework of Alford's Theory of Structural Interests in Health Care PPT 28 PresentedRashed ShukornoNo ratings yet
- National Health PolicyDocument22 pagesNational Health PolicyAncy Varkey100% (2)
- Leadership Concept & TheoryDocument22 pagesLeadership Concept & TheoryJay PaulNo ratings yet
- Chapter 5 - Group DynamicsDocument7 pagesChapter 5 - Group DynamicsLord GrimNo ratings yet
- Leadership & MGTDocument128 pagesLeadership & MGTmutegeki nathanNo ratings yet
- Chapter 2 Approaches To EntrepreneurshipDocument3 pagesChapter 2 Approaches To EntrepreneurshiprajendrakumarNo ratings yet
- Paper Presentation - Doc NewDocument12 pagesPaper Presentation - Doc NewMontu DaveNo ratings yet
- Models of HealthDocument16 pagesModels of HealthCherry Ann Garcia DuranteNo ratings yet
- Department of Health Departmental Report 2008Document253 pagesDepartment of Health Departmental Report 2008Bren-RNo ratings yet
- Block Level Development PlanningDocument20 pagesBlock Level Development Planningyaswanth chowdaryNo ratings yet
- Head NursingDocument69 pagesHead NursingGrace JPNo ratings yet
- Jakarta DeclarationDocument20 pagesJakarta DeclarationBeesnu KhanalNo ratings yet
- Vaccines With Diluents How To Use ThemDocument1 pageVaccines With Diluents How To Use ThemMoinNo ratings yet
- Health Care Delivery SystemDocument75 pagesHealth Care Delivery SystemSudha YadavNo ratings yet
- Community Health A Complete Guide - 2020 EditionFrom EverandCommunity Health A Complete Guide - 2020 EditionRating: 5 out of 5 stars5/5 (1)
- Extended Program of ImmunizationDocument39 pagesExtended Program of ImmunizationJohn Go LiNo ratings yet
- Immunization: Mei Neni S Pediatric Dept. Faculty of Medicine, Gadjah Mada UniversityDocument35 pagesImmunization: Mei Neni S Pediatric Dept. Faculty of Medicine, Gadjah Mada UniversityadystiNo ratings yet
- Primary Level Care of TB 1Document27 pagesPrimary Level Care of TB 1okwadha simionNo ratings yet
- Market Visit ReportDocument10 pagesMarket Visit Reportokwadha simionNo ratings yet
- Child Health Epidemiology (Corrected)Document29 pagesChild Health Epidemiology (Corrected)okwadha simionNo ratings yet
- UN Convention On The Rights of ChildrenDocument70 pagesUN Convention On The Rights of Childrenokwadha simionNo ratings yet
- Malaria MB CHB January 2018-FinalDocument36 pagesMalaria MB CHB January 2018-Finalokwadha simionNo ratings yet
- Paul The ApostleDocument3 pagesPaul The Apostleokwadha simionNo ratings yet
- Primary Level Care of MalariaDocument26 pagesPrimary Level Care of Malariaokwadha simionNo ratings yet
- Market Visit Report XDocument12 pagesMarket Visit Report Xokwadha simionNo ratings yet
- Physical Examination: Prof. Ezekiel M. WafulaDocument19 pagesPhysical Examination: Prof. Ezekiel M. Wafulaokwadha simionNo ratings yet
- Pneumonia: Prof. Ezekiel M. WafulaDocument20 pagesPneumonia: Prof. Ezekiel M. Wafulaokwadha simion100% (1)
- Final Major Milestones During First Five Years of Life - GiDocument22 pagesFinal Major Milestones During First Five Years of Life - Giokwadha simionNo ratings yet
- Nephrotic Syndrome in Children: by Prof Grace W. Irimu (Mmed, PHD)Document46 pagesNephrotic Syndrome in Children: by Prof Grace W. Irimu (Mmed, PHD)okwadha simionNo ratings yet
- Pediatric Burn InjuriesDocument12 pagesPediatric Burn Injuriesokwadha simionNo ratings yet
- Kepi Vaccines (2) - Gi - 1Document30 pagesKepi Vaccines (2) - Gi - 1okwadha simionNo ratings yet
- Market Visit Report DraftDocument11 pagesMarket Visit Report Draftokwadha simion0% (1)
- Overview Common Dermatologic Problems in ChildrenDocument26 pagesOverview Common Dermatologic Problems in Childrenokwadha simionNo ratings yet
- Immunization Policy Guidline - Kenya 2013Document72 pagesImmunization Policy Guidline - Kenya 2013okwadha simionNo ratings yet
- Kangaroo Mother Care Kenya GuidelinesDocument48 pagesKangaroo Mother Care Kenya Guidelinesokwadha simionNo ratings yet
- Non Kepi Vaccines RevisedDocument28 pagesNon Kepi Vaccines Revisedokwadha simionNo ratings yet
- Hiv (1) - GI - 1-1Document28 pagesHiv (1) - GI - 1-1okwadha simionNo ratings yet
- Etat Module Kenya For Distance LearnersDocument242 pagesEtat Module Kenya For Distance Learnersokwadha simion100% (1)
- Malnutrition Morris Adams MDocument31 pagesMalnutrition Morris Adams Mokwadha simionNo ratings yet
- Low Birth Weight BabiesDocument17 pagesLow Birth Weight Babiesokwadha simionNo ratings yet
- Community Case Management: BY:Nathifa Abdi H31/34946/2013 and Busaidy Swafiya H31/2369/2012Document37 pagesCommunity Case Management: BY:Nathifa Abdi H31/34946/2013 and Busaidy Swafiya H31/2369/2012okwadha simionNo ratings yet
- ETAT 5th Year Undergrad Training November 27.2017Document2 pagesETAT 5th Year Undergrad Training November 27.2017okwadha simionNo ratings yet
- Dialogue Objective Data (050,054.057)Document5 pagesDialogue Objective Data (050,054.057)Lina DewiNo ratings yet
- 02 Provmeritlist r3Document1,156 pages02 Provmeritlist r3Yash MishraNo ratings yet
- Cmca Lec MidtermDocument43 pagesCmca Lec MidtermKate Onniel RimandoNo ratings yet
- Pediatric Research: Challenges and Innovative MeasuresDocument3 pagesPediatric Research: Challenges and Innovative MeasuresIJCIRAS Research PublicationNo ratings yet
- Read The Text Dialogue and Then Answer The Questions Carefully!Document1 pageRead The Text Dialogue and Then Answer The Questions Carefully!SMA PGRI KESAMBENNo ratings yet
- Steelman, Graling - 2013 - Top 10 Patient Safety Issues What More Can We DoDocument23 pagesSteelman, Graling - 2013 - Top 10 Patient Safety Issues What More Can We DoElNo ratings yet
- Ayurveda Medical BooksDocument66 pagesAyurveda Medical BooksHitu ParNo ratings yet
- Ctms For IcriDocument70 pagesCtms For IcrisomcologyNo ratings yet
- 48.pelvic RockingDocument6 pages48.pelvic RockingRani MarianaNo ratings yet
- Approach To The Cat With Upper Respiratory Tract Signs Slides 2023Document49 pagesApproach To The Cat With Upper Respiratory Tract Signs Slides 2023Fran G. KittsteinerNo ratings yet
- 1 s2.0 S1098301523000979 MainDocument8 pages1 s2.0 S1098301523000979 MainDiana AyuNo ratings yet
- Public Health Officers and Technicians Council, KenyaDocument2 pagesPublic Health Officers and Technicians Council, KenyaDanielNo ratings yet
- Filtek Supreme XTEDocument6 pagesFiltek Supreme XTEOral CareNo ratings yet
- Vaginal Vs C SectionDocument5 pagesVaginal Vs C Sectionapi-602766530No ratings yet
- Healing Following Implant Surgery: Osseous Healing-Early PhaseDocument2 pagesHealing Following Implant Surgery: Osseous Healing-Early PhaseUrjita PatilNo ratings yet
- Personal Hygiene For Food HandlersDocument3 pagesPersonal Hygiene For Food Handlersputri augustyaNo ratings yet
- 2011 Comtemporary Periodontal Surgery CPCCDocument193 pages2011 Comtemporary Periodontal Surgery CPCCwuhan lalalaNo ratings yet
- Case Scenario - PulmonaryDocument2 pagesCase Scenario - PulmonaryCHRISTINE JULIANENo ratings yet
- Emerging and Reemerging Diseases - Programs and Policies On Communicable DiseasesDocument34 pagesEmerging and Reemerging Diseases - Programs and Policies On Communicable DiseasesTim Dequillo100% (1)
- Obstetrics Cases by Caroline de CostaDocument9 pagesObstetrics Cases by Caroline de CostaJeffrey HingNo ratings yet
- Niculae Ciobanu, MD, FACP Joins Manhattan Cancer AssociatesDocument2 pagesNiculae Ciobanu, MD, FACP Joins Manhattan Cancer AssociatesPR.comNo ratings yet
- Xavier University - Ateneo de Cagayan College of Nursing S.Y. 2020-2021Document5 pagesXavier University - Ateneo de Cagayan College of Nursing S.Y. 2020-2021Dudil GoatNo ratings yet
- Typhon Group Procedures Skills TotalsDocument3 pagesTyphon Group Procedures Skills Totalsapi-642376263No ratings yet
- Q3 - Periodical Test HEALTHDocument2 pagesQ3 - Periodical Test HEALTHPrimalyn SupnadNo ratings yet
- A Rare Cause of Dysphagia - Compression of The Esophagus by An Anterior Cervical Osteophyte Due To Ankylosing SpondylitisDocument5 pagesA Rare Cause of Dysphagia - Compression of The Esophagus by An Anterior Cervical Osteophyte Due To Ankylosing SpondylitisEduardo Lima de Melo Jr.No ratings yet