You might also like
- Monastery of The Seven Rays - Year 1Document193 pagesMonastery of The Seven Rays - Year 1Lykathea Harmony Pax100% (5)
- Stroke: Intracranial Abnormalities With Hetal Verma, MDDocument30 pagesStroke: Intracranial Abnormalities With Hetal Verma, MDRawabi rawabi1997No ratings yet
- Arrhythmia For NursesDocument49 pagesArrhythmia For NursesRajesh T EapenNo ratings yet
- Anatomy of Forearm and Wrist - ppt1Document46 pagesAnatomy of Forearm and Wrist - ppt1Julian GordonNo ratings yet
- Six Minute Walk Test - : Nimisha B (MPT, Dyhe) Assisstant Professor Sacpms, MMC ModakkallurDocument16 pagesSix Minute Walk Test - : Nimisha B (MPT, Dyhe) Assisstant Professor Sacpms, MMC ModakkallurNimisha Balakrishnan100% (1)
- Reviewer-IN-FAR - Lecture Notes Financial Accounting and Reporting 1-10 Reviewer-IN-FAR - Lecture Notes Financial Accounting and Reporting 1-10Document4 pagesReviewer-IN-FAR - Lecture Notes Financial Accounting and Reporting 1-10 Reviewer-IN-FAR - Lecture Notes Financial Accounting and Reporting 1-10Jocelyn TejerosNo ratings yet
- Thyroglossal Duct Cysts, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandThyroglossal Duct Cysts, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Motor System: Three Types of Movement Generated by Motor SystemDocument10 pagesMotor System: Three Types of Movement Generated by Motor SystemVon Hippo100% (1)
- Categorization of Rabies Exposure HypertensionDocument2 pagesCategorization of Rabies Exposure HypertensionNikki ValerioNo ratings yet
- The Circulation: Blood Pressure RegulationDocument42 pagesThe Circulation: Blood Pressure RegulationLouis JinNo ratings yet
- Very Common Questions:-: PhysiologyDocument15 pagesVery Common Questions:-: PhysiologyJohn M. HemsworthNo ratings yet
- 2017 BMA Medical Book AwardsDocument45 pages2017 BMA Medical Book AwardsFerdinand Sta Ana Jr.No ratings yet
- Inhalational Anesthetics: Patigas, Requinta, ResuelloDocument88 pagesInhalational Anesthetics: Patigas, Requinta, Resuellosarguss140% (1)
- Pulmonary Artery HypertensionDocument21 pagesPulmonary Artery HypertensionAzizi Abd RahmanNo ratings yet
- Pass Critical Care Endocrine Frcem ResourcesDocument41 pagesPass Critical Care Endocrine Frcem ResourcesYoussef SaadNo ratings yet
- Head and Neck Anatomy and Ultrasound Correlation 2010Document9 pagesHead and Neck Anatomy and Ultrasound Correlation 2010Lucila BrañaNo ratings yet
- Achalasia: Department of MedicineDocument21 pagesAchalasia: Department of Medicinekyliever100% (1)
- Booklist For MedDocument16 pagesBooklist For Medngc1100% (1)
- Resp Physio SAQsDocument25 pagesResp Physio SAQsanaeshkl100% (1)
- Sonoanatomy of The Spine A Comprehensive Scanning Protocol From Cervical To Sacral RegionDocument9 pagesSonoanatomy of The Spine A Comprehensive Scanning Protocol From Cervical To Sacral Regionfajarrudy qimindraNo ratings yet
- An Overview of Therapeutic Plasma ExchangeDocument65 pagesAn Overview of Therapeutic Plasma ExchangesayednourNo ratings yet
- Anestesia Pediatrica 2015Document292 pagesAnestesia Pediatrica 2015Eloy BurdaNo ratings yet
- Sales & Distribution User ExitsDocument12 pagesSales & Distribution User ExitsRamesh Balaji100% (2)
- The Public Health System in Afghanistan: Current Issues: January 2002Document47 pagesThe Public Health System in Afghanistan: Current Issues: January 2002جاهد نبیل100% (1)
- Approach To Interstitial Lung Disease 1Document33 pagesApproach To Interstitial Lung Disease 1MichaelNo ratings yet
- Hwalla 2021 Dietary Management of ObesityDocument21 pagesHwalla 2021 Dietary Management of ObesityHugo Whysk LeonardoNo ratings yet
- Dr. Ashok Deorari - Non Invasive Ventilation Way Forward For IndiaDocument11 pagesDr. Ashok Deorari - Non Invasive Ventilation Way Forward For IndiaKalyan DamisettiNo ratings yet
- Veterinary Pharmacology 2016Document6 pagesVeterinary Pharmacology 2016Stephan StephanNo ratings yet
- 13 Terminology2016Document469 pages13 Terminology2016肖楚天No ratings yet
- NIST Fingerprint Testing StandardsDocument75 pagesNIST Fingerprint Testing StandardsCash Cash CashNo ratings yet
- UiA 33 Final Replacement Web 2Document80 pagesUiA 33 Final Replacement Web 2uzairNo ratings yet
- Case Study - Wal-Mart Failure in GermanyDocument5 pagesCase Study - Wal-Mart Failure in GermanyYasser SadekNo ratings yet
- IOM in Scoliosis TMHDocument75 pagesIOM in Scoliosis TMHtuanemgNo ratings yet
- Principle of UltrasoundDocument10 pagesPrinciple of UltrasoundRanveer SinghNo ratings yet
- Thyroid Disorders Testing AlgorithmDocument1 pageThyroid Disorders Testing AlgorithmkatNo ratings yet
- UltrasoundDocument26 pagesUltrasoundMoussab Damlaj100% (1)
- LAPTARE Copii Cu Patologie...Document8 pagesLAPTARE Copii Cu Patologie...Claudia KosztelnikNo ratings yet
- October 19, 2007 Marcia Spooner Pgy 1 Family MedicineDocument23 pagesOctober 19, 2007 Marcia Spooner Pgy 1 Family Medicinemary_chdhryNo ratings yet
- NEJM 2014 Fundamentals of Lung AuscultationDocument7 pagesNEJM 2014 Fundamentals of Lung AuscultationFelipe CeaNo ratings yet
- IDSA-ATS - Consensus Guidelines On The Management of CAP in AdultsDocument46 pagesIDSA-ATS - Consensus Guidelines On The Management of CAP in AdultscharliedelNo ratings yet
- Pirads V2Document64 pagesPirads V2ekowahyudiNo ratings yet
- Full Chapter Volpe S Neurology of The Newborn 7Th Edition Joseph J Volpe PDFDocument53 pagesFull Chapter Volpe S Neurology of The Newborn 7Th Edition Joseph J Volpe PDFdennis.davis980No ratings yet
- Basics Principles of RadiologyDocument55 pagesBasics Principles of RadiologyJunaedy HfNo ratings yet
- Internship Survival Guide NSHDocument36 pagesInternship Survival Guide NSHRichardNo ratings yet
- Difiores Atlas of Histology With Functional Correlations With Online Access 12th Ed PDFDocument6 pagesDifiores Atlas of Histology With Functional Correlations With Online Access 12th Ed PDFJackNo ratings yet
- Clinical Heart DiseaseDocument2 pagesClinical Heart DiseaselavanyaNo ratings yet
- Abdominal Incision1Document11 pagesAbdominal Incision1njoNo ratings yet
- Journal Reading PulmonologiDocument21 pagesJournal Reading PulmonologiGina ArianiNo ratings yet
- Respiratory Exam Checklist1sadsadDocument1 pageRespiratory Exam Checklist1sadsadDawoodAslamNo ratings yet
- Tendon TransfersDocument26 pagesTendon TransfersJohnny Wang100% (1)
- Mitral RegurgitationDocument10 pagesMitral RegurgitationWalter Saavedra YarlequeNo ratings yet
- 02 - Aims of Obstetric Critical Care ManagementDocument25 pages02 - Aims of Obstetric Critical Care ManagementAlberto Kenyo Riofrio PalaciosNo ratings yet
- Evolution in Screening For Down Syndrome: ReviewsDocument7 pagesEvolution in Screening For Down Syndrome: ReviewsMayada Osman100% (1)
- General Anaesthesia: Anaesthesia and Critical Care DeptDocument46 pagesGeneral Anaesthesia: Anaesthesia and Critical Care DeptAnonymous A2d5hUNeMiNo ratings yet
- Thyroid Function TestsDocument25 pagesThyroid Function TestsEva SinghNo ratings yet
- 9 Retinal DetachmentDocument6 pages9 Retinal DetachmentNinin Erdininsih ArNo ratings yet
- 2009432Document32 pages2009432Luis Alberto Letona QuispeNo ratings yet
- Ultrasound - A GuideDocument9 pagesUltrasound - A GuideDebasish KunduNo ratings yet
- ANAT2341 Embryology: Early and Systemic Development: School of Medical SciencesDocument8 pagesANAT2341 Embryology: Early and Systemic Development: School of Medical SciencesJimson EchaveNo ratings yet
- Diabetes Problem Based Learning PDFDocument6 pagesDiabetes Problem Based Learning PDFIfantri Pramana100% (1)
- Altered Mental StatusDocument151 pagesAltered Mental StatusbrentupdegraffNo ratings yet
- Neonatal Air Leak Syndrome and The Role Of.3Document9 pagesNeonatal Air Leak Syndrome and The Role Of.3Claudia KosztelnikNo ratings yet
- Mechanical Ventilation Guidelines SNSDocument8 pagesMechanical Ventilation Guidelines SNSClaudia KosztelnikNo ratings yet
- Imaging Findings in Cardiac Tamponade With EmphasiDocument18 pagesImaging Findings in Cardiac Tamponade With EmphasiClaudia KosztelnikNo ratings yet
- 03 - Special Clinical SituationsDocument32 pages03 - Special Clinical SituationsClaudia KosztelnikNo ratings yet
- User Guide: IBM Micromedex® Neofax® and PediatricsDocument57 pagesUser Guide: IBM Micromedex® Neofax® and PediatricsClaudia KosztelnikNo ratings yet
- 406ronmfrt0n7269301 PDFDocument5 pages406ronmfrt0n7269301 PDFClaudia KosztelnikNo ratings yet
- Evolution of NeonatologyDocument17 pagesEvolution of NeonatologyClaudia KosztelnikNo ratings yet
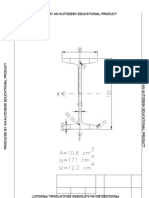
- Produced by An Autodesk Educational ProductDocument1 pageProduced by An Autodesk Educational ProductClaudia KosztelnikNo ratings yet
- High DoseDocument6 pagesHigh DoseClaudia KosztelnikNo ratings yet
- Citadels of Chaos by Cornelius Carl Veith 45Document214 pagesCitadels of Chaos by Cornelius Carl Veith 45joeycrackNo ratings yet
- My ResumeDocument8 pagesMy ResumeShaikh Mohd ShahbazNo ratings yet
- Applied Mechanics I - Fall 2013 PDFDocument4 pagesApplied Mechanics I - Fall 2013 PDFRajeshGupta100% (1)
- Cutting-Edge Fertilizer Know-How - at Your Disposal: Industrial SolutionsDocument12 pagesCutting-Edge Fertilizer Know-How - at Your Disposal: Industrial SolutionsRAMESHWAR VEDACHALAMNo ratings yet
- Improving Spectral Efficiency Using Generalized Frequency Division Multiplexing With Flexible Index ModulationDocument24 pagesImproving Spectral Efficiency Using Generalized Frequency Division Multiplexing With Flexible Index ModulationmerlineNo ratings yet
- Pioneer VSX 417Document52 pagesPioneer VSX 417cristakeNo ratings yet
- BS Iso Iec 29794-1-2009Document34 pagesBS Iso Iec 29794-1-2009Олег СоловьевNo ratings yet
- Introduction To Engineering Mechanics PDDocument21 pagesIntroduction To Engineering Mechanics PDReyzel Anne FaylognaNo ratings yet
- سلسلة المحاضرات الإليكترونية فى علم المساحة المحاضرة 3 المساحات وتقسيم الألأراضى Areas & Land subdivisionDocument48 pagesسلسلة المحاضرات الإليكترونية فى علم المساحة المحاضرة 3 المساحات وتقسيم الألأراضى Areas & Land subdivisionmahmoud abdelrahman67% (3)
- Technology For My Teacher ToolboxDocument5 pagesTechnology For My Teacher Toolboxapi-439444920No ratings yet
- Learning Hydroponics ReportDocument16 pagesLearning Hydroponics Reportszecke01No ratings yet
- Principles of ArtsDocument19 pagesPrinciples of ArtsMiles SerranoNo ratings yet
- Modul 1 Using Pronoun (Menggunakan Kata Ganti)Document3 pagesModul 1 Using Pronoun (Menggunakan Kata Ganti)syafira putriNo ratings yet
- City of Manila v. Coca-Cola BottlersDocument17 pagesCity of Manila v. Coca-Cola BottlersRo CheNo ratings yet
- Module D ZS4200 R4.0 Operator V1.01Document31 pagesModule D ZS4200 R4.0 Operator V1.01stefan63byNo ratings yet
- Final Exam Econ 2Document8 pagesFinal Exam Econ 2Ysabel Grace BelenNo ratings yet
- Wheeze in Children: Asthma Clinical Pathway: Departments of Emergency Medicine and PaediatricsDocument4 pagesWheeze in Children: Asthma Clinical Pathway: Departments of Emergency Medicine and Paediatricsscanutd100% (1)
- Tandem 4Document4 pagesTandem 4Abdul RazakNo ratings yet
- Daftar PustakaDocument3 pagesDaftar PustakafaizatinqisthimaulaNo ratings yet
- Pharmacology Block 1.3 - PharmacodynamicsDocument12 pagesPharmacology Block 1.3 - Pharmacodynamicsdaleng subNo ratings yet
- Tattle TaleDocument3 pagesTattle TaleFilipino ZinergyNo ratings yet
- Riverboat CasinosDocument4 pagesRiverboat CasinosAngela BrownNo ratings yet
- Aslam ResumeDocument2 pagesAslam ResumeBoopathi JothiNo ratings yet
- LEEP System 1000 Directions For UseeDocument24 pagesLEEP System 1000 Directions For UseeFernando CosciaNo ratings yet
- Product Info WISI-GT-31-W V3.0 enDocument2 pagesProduct Info WISI-GT-31-W V3.0 enDiego MattaNo ratings yet