You might also like
- Results CAPE 2019Document348 pagesResults CAPE 2019Bradlee Singh60% (5)
- American Board of Family Medicine: TTT SAMPLE TTTDocument72 pagesAmerican Board of Family Medicine: TTT SAMPLE TTTSalah Elbadawy100% (1)
- Concept Map On HyponatremiaDocument1 pageConcept Map On HyponatremiaNeil Alibangbang0% (1)
- Fluid Electrolyte Balances and ImbalanceDocument157 pagesFluid Electrolyte Balances and ImbalanceManisha Shakya0% (1)
- Fluids and Electrolytes-SeminarDocument119 pagesFluids and Electrolytes-Seminarنديم الباهليNo ratings yet
- MS - Fluids and ElectrolytesDocument6 pagesMS - Fluids and ElectrolytesJOHN LOYD CASTILLONo ratings yet
- 2 5463111801086427966Document13 pages2 5463111801086427966haidernadhem57No ratings yet
- Fluid PDFDocument93 pagesFluid PDFSandeep VermaNo ratings yet
- FluidelectrolytebalanceDocument87 pagesFluidelectrolytebalancePavi MuruganathanNo ratings yet
- CairanDocument60 pagesCairanHanum HanattaNo ratings yet
- Water and Electrolytes-Balance and ImbalanceDocument54 pagesWater and Electrolytes-Balance and ImbalanceAaQib BhatNo ratings yet
- Complete Metabolic PanelDocument12 pagesComplete Metabolic PanelimperiouxxNo ratings yet
- Fe Finals NotesDocument23 pagesFe Finals NoteshanhananicasNo ratings yet
- BODY Weight 100%: Balance/Imbalances & TherapyDocument11 pagesBODY Weight 100%: Balance/Imbalances & TherapyVictoria Castillo TamayoNo ratings yet
- ภาพถ่ายหน้าจอ 2564-11-26 เวลา 11.17.04Document59 pagesภาพถ่ายหน้าจอ 2564-11-26 เวลา 11.17.04CHULEEMAT KAEWDANGNo ratings yet
- Terapi Cairan Pada AnakDocument48 pagesTerapi Cairan Pada AnakAstri Novia RizqiNo ratings yet
- Electrolyte DisordersDocument29 pagesElectrolyte Disorderssanketh bhat.sNo ratings yet
- Nursing 75 Fluid and Electrolyte Exam 2Document6 pagesNursing 75 Fluid and Electrolyte Exam 2chubbygunny_29776413No ratings yet
- Fluid and Electrolyte Imbalance: NURS601: Fundamentals of Acute Nursing Practice DR Sara NapierDocument89 pagesFluid and Electrolyte Imbalance: NURS601: Fundamentals of Acute Nursing Practice DR Sara NapierFano AsiataNo ratings yet
- CC Lec Mod 3Document13 pagesCC Lec Mod 38wgmhh9ks9No ratings yet
- Disturbances in Water, Electrolyte and Acid-Base Balance: Dr. Njau.N.NDocument52 pagesDisturbances in Water, Electrolyte and Acid-Base Balance: Dr. Njau.N.NKeith OmwoyoNo ratings yet
- Electrolyte Disorders - 1Document29 pagesElectrolyte Disorders - 1sanketh bhat.sNo ratings yet
- Disorders of Water-Salt Metabolism: Prof. Oleksandr AtamanDocument35 pagesDisorders of Water-Salt Metabolism: Prof. Oleksandr AtamanZAKIA KHALID ALINo ratings yet
- Chap69 PDFDocument3 pagesChap69 PDFIkrar SyahmarNo ratings yet
- Common Electrolyte Disturbances and Management Edited 2023Document46 pagesCommon Electrolyte Disturbances and Management Edited 2023abdurabengNo ratings yet
- Electrolytes Slide 21Document111 pagesElectrolytes Slide 21Elaisha Mae C. CarsulaNo ratings yet
- Alteration in Fluid and Electrolyte ImbalanceDocument118 pagesAlteration in Fluid and Electrolyte ImbalanceRenuga SureshNo ratings yet
- Electrolytes LecDocument4 pagesElectrolytes LecMichelle San Miguel FeguroNo ratings yet
- Electrolytes To Phosphorus PPTsDocument99 pagesElectrolytes To Phosphorus PPTsMarvin SimbulanNo ratings yet
- Dasar - Dasar Terapi: Cairan Dan ElektrolitDocument60 pagesDasar - Dasar Terapi: Cairan Dan ElektrolitdedeNo ratings yet
- Fluid & Electrolyte 2Document47 pagesFluid & Electrolyte 2Worku KifleNo ratings yet
- FluidTx MaintenanceDocument22 pagesFluidTx MaintenanceJonathan IngramNo ratings yet
- Fluid Electrolyte Imbalance NvertedDocument111 pagesFluid Electrolyte Imbalance Nvertedchitrakshi khairnarNo ratings yet
- Renal Lecture 1aDocument34 pagesRenal Lecture 1atyhbbhhNo ratings yet
- Electrolytedisturbances 111102083753 Phpapp02Document137 pagesElectrolytedisturbances 111102083753 Phpapp02bobbyfildianNo ratings yet
- Fluid and ElectrolyteDocument57 pagesFluid and ElectrolyteJustin Ahorro-DionisioNo ratings yet
- Fluid and Electrolyte Balance in ICUDocument46 pagesFluid and Electrolyte Balance in ICUtapas_kbNo ratings yet
- Hypernatremia: Marielle Adey R. Magcawas BSN-3CDocument28 pagesHypernatremia: Marielle Adey R. Magcawas BSN-3CMarielle Adey Magcawas RNNo ratings yet
- Fluid and Elctrolyte Balance.... Power PointDocument40 pagesFluid and Elctrolyte Balance.... Power PointMarwan M.100% (1)
- Water and Sodium 2024 PDFDocument61 pagesWater and Sodium 2024 PDFMpho MosehlaNo ratings yet
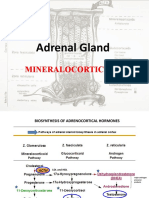
- Adrenal Gland by Dr. Rajnee IInd PartDocument30 pagesAdrenal Gland by Dr. Rajnee IInd Part9460106212No ratings yet
- HD B Braun For CNN TakersDocument6 pagesHD B Braun For CNN TakersWhimsey CipresNo ratings yet
- Balda Electrolyte DisbalanceDocument33 pagesBalda Electrolyte DisbalanceBaldandorj KhavalkhaanNo ratings yet
- Diagnosis and Management of Common Electrolyte DisordersDocument42 pagesDiagnosis and Management of Common Electrolyte DisorderspandeNo ratings yet
- Main Fluid and ElectrolyteDocument133 pagesMain Fluid and ElectrolyteMaria Charis Anne IndananNo ratings yet
- 3 Fluids and Electrolytes PPDocument112 pages3 Fluids and Electrolytes PPjcodoyNo ratings yet
- ELECTROLYTES Edited Semi Finals XDDocument52 pagesELECTROLYTES Edited Semi Finals XDzerachiel zephyrNo ratings yet
- Electrolytes Part 2Document54 pagesElectrolytes Part 2Vincent ReyesNo ratings yet
- Electrolytes Water Balance PH Balance Trace MetalsDocument21 pagesElectrolytes Water Balance PH Balance Trace MetalsJohn Kevin Carl SaligumbaNo ratings yet
- Electrolyte ImbalanceDocument79 pagesElectrolyte Imbalancemarauder_popNo ratings yet
- Fluid TherapyDocument36 pagesFluid TherapyAmin MasromNo ratings yet
- Composition of Fluid & ElectrolytesDocument33 pagesComposition of Fluid & ElectrolytesDwi SiregarNo ratings yet
- Fluid & Electrolytes: DR Win Min OoDocument55 pagesFluid & Electrolytes: DR Win Min OoBiomedical Science MyanmarNo ratings yet
- ElectrolytesDocument102 pagesElectrolytesveenatagsipNo ratings yet
- Chapter 29-Fluids and ElectrolytesDocument5 pagesChapter 29-Fluids and ElectrolytesCharlena LittleNo ratings yet
- Management Terapi CairanDocument60 pagesManagement Terapi CairanHayat Hamzah DawiNo ratings yet
- Dehydration PresentationDocument3 pagesDehydration PresentationAhsan KhanNo ratings yet
- CH 39 Acid-Base ElectrolyteDocument16 pagesCH 39 Acid-Base ElectrolyteJonathan EdieNo ratings yet
- Francis M. Albances, RN SPU Iloilo 2009Document126 pagesFrancis M. Albances, RN SPU Iloilo 2009Christian Lester Ramos PastorNo ratings yet
- Fluid & ElectrolyteDocument69 pagesFluid & ElectrolytePaul Ebenezer100% (1)
- Surgery YbDocument67 pagesSurgery YbTamirat geletaNo ratings yet
- Fast Facts: Pyruvatkinase-Mangel für Patienten und Angehörige: Eine seltene genetische Erkrankung der roten Blutkörperchen Informationen + Mitreden-Können = Bestmöglicher VerlaufFrom EverandFast Facts: Pyruvatkinase-Mangel für Patienten und Angehörige: Eine seltene genetische Erkrankung der roten Blutkörperchen Informationen + Mitreden-Können = Bestmöglicher VerlaufNo ratings yet
- DDCS Memo - Pathway For Addressing Concerns, Complaints and QuestionsDocument1 pageDDCS Memo - Pathway For Addressing Concerns, Complaints and QuestionsTheBoss 20No ratings yet
- Practicum Final Presentation Rubric 2018 April 03 ASDocument1 pagePracticum Final Presentation Rubric 2018 April 03 ASTheBoss 20No ratings yet
- Question Paper - Vetm 2002 - December - Final Examination - 2020-21Document10 pagesQuestion Paper - Vetm 2002 - December - Final Examination - 2020-21TheBoss 20No ratings yet
- Prof Akpaka - Antimicrobials - MoADocument33 pagesProf Akpaka - Antimicrobials - MoATheBoss 20No ratings yet
- Practicum Final RubricDocument2 pagesPracticum Final RubricTheBoss 20No ratings yet
- Psarocolius - Decumanus - Crested Oropendola or CornbirdDocument6 pagesPsarocolius - Decumanus - Crested Oropendola or CornbirdTheBoss 20No ratings yet
- Hoof AnatomyDocument19 pagesHoof AnatomyTheBoss 20No ratings yet
- Public Health RegulationsDocument12 pagesPublic Health RegulationsTheBoss 20No ratings yet
- Prof Akpaka - Transmission and PathogenesisDocument19 pagesProf Akpaka - Transmission and PathogenesisTheBoss 20No ratings yet
- Ns CR Ip T: The University of The West IndiesDocument2 pagesNs CR Ip T: The University of The West IndiesTheBoss 20No ratings yet
- Salary Relief Grant Final FillDocument4 pagesSalary Relief Grant Final FillTheBoss 20No ratings yet
- Question Paper - Vetm 2004 - Final Examination - 2020-21Document3 pagesQuestion Paper - Vetm 2004 - Final Examination - 2020-21TheBoss 20No ratings yet
- RegulationsDocument6 pagesRegulationsTheBoss 20No ratings yet
- Salary Relief Grant Final FillDocument4 pagesSalary Relief Grant Final FillTheBoss 20No ratings yet
- Revised VETM 2003 CA1 ResultsDocument1 pageRevised VETM 2003 CA1 ResultsTheBoss 20No ratings yet
- Semester II Course Listing - Year 1Document1 pageSemester II Course Listing - Year 1TheBoss 20No ratings yet
- Sectiond 816017350Document9 pagesSectiond 816017350TheBoss 20No ratings yet
- Sheep HandlingDocument12 pagesSheep HandlingTheBoss 20No ratings yet
- VETM 2005 Section B DECEMBER 2020 - Case Studies Each Answer Is Worth One (1) Mark Unless Otherwise StatedDocument9 pagesVETM 2005 Section B DECEMBER 2020 - Case Studies Each Answer Is Worth One (1) Mark Unless Otherwise StatedTheBoss 20No ratings yet
- Sample Extended Matching Questions (Emqs) (MDSC 1002, 1 Year Students)Document2 pagesSample Extended Matching Questions (Emqs) (MDSC 1002, 1 Year Students)TheBoss 20No ratings yet
- SCHOOL OF VETERINARY MEDICINE TIMETABLE Final (Yr 1)Document1 pageSCHOOL OF VETERINARY MEDICINE TIMETABLE Final (Yr 1)TheBoss 20No ratings yet
- Send Your Buddy Some OO DayDocument17 pagesSend Your Buddy Some OO DayTheBoss 20No ratings yet
- Spotter - MDSC 1002Document3 pagesSpotter - MDSC 1002TheBoss 20No ratings yet
- Special Arthrology of The ForelimbDocument37 pagesSpecial Arthrology of The ForelimbTheBoss 20No ratings yet
- Slide Bank - Mdsc1002haem.2017 2018Document16 pagesSlide Bank - Mdsc1002haem.2017 2018TheBoss 20No ratings yet
- Sibling Sexual Abuse: A Guide For ParentsDocument10 pagesSibling Sexual Abuse: A Guide For ParentsTheBoss 20100% (1)
- SGU SVM Zoetis Wellness Webinar The Human - Animal Bond Pets Provide Peace During A Pandemonium DR MobleyDocument1 pageSGU SVM Zoetis Wellness Webinar The Human - Animal Bond Pets Provide Peace During A Pandemonium DR MobleyTheBoss 20No ratings yet
- Spotter PrepDocument50 pagesSpotter PrepTheBoss 20No ratings yet
- Special Arthorology of The ForelimbDocument34 pagesSpecial Arthorology of The ForelimbTheBoss 20No ratings yet
- Predictor 6Document42 pagesPredictor 6Christine Ann GuinitaranNo ratings yet
- Recent Advances in The Management of Hypoxic-Ischemic Encephalopathy-IJPPDocument6 pagesRecent Advances in The Management of Hypoxic-Ischemic Encephalopathy-IJPPdrtgodeNo ratings yet
- Management of Electrolyte Emergencies: Emergency Medicine Board Review ManualDocument12 pagesManagement of Electrolyte Emergencies: Emergency Medicine Board Review ManualAnam FarooqNo ratings yet
- (1479683X - European Journal of Endocrinology) The Syndrome of Inappropriate Antidiuretic Hormone - Current and Future Management OptionsDocument6 pages(1479683X - European Journal of Endocrinology) The Syndrome of Inappropriate Antidiuretic Hormone - Current and Future Management OptionsYulius DonyNo ratings yet
- Understanding Head InjuryDocument254 pagesUnderstanding Head InjuryAshwini SharmaNo ratings yet
- Endocrine - FRCEM SuccessDocument110 pagesEndocrine - FRCEM SuccessskNo ratings yet
- Siadh Patient Case - Final1Document43 pagesSiadh Patient Case - Final1api-589685298No ratings yet
- Fluid Management in NicuDocument56 pagesFluid Management in NicuG Venkatesh100% (2)
- A Case Report On Hyponatremia Leading Sign of Hypopituitarism (Secondary To Adrenal Insufficiency)Document4 pagesA Case Report On Hyponatremia Leading Sign of Hypopituitarism (Secondary To Adrenal Insufficiency)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Paraneoplastic Syndromes Associated With LaryngealDocument15 pagesParaneoplastic Syndromes Associated With Laryngealandre halimNo ratings yet
- Critical Care Notes Clinical Pocket Guide - (Hematology Oncology)Document17 pagesCritical Care Notes Clinical Pocket Guide - (Hematology Oncology)Britanny NelsonNo ratings yet
- Acid Base Electolytes QuestionsDocument4 pagesAcid Base Electolytes QuestionsDonna R. Joyce0% (1)
- Endo Modified PDFDocument35 pagesEndo Modified PDFCarl JustineNo ratings yet
- SIADHDocument2 pagesSIADHKyla MacabulosNo ratings yet
- EL Husseiny's Essentials of Endocrinology 1247Document152 pagesEL Husseiny's Essentials of Endocrinology 1247حنين عاطفNo ratings yet
- Hyponatremia - Annals of Internal Medicine 2015Document19 pagesHyponatremia - Annals of Internal Medicine 2015ntnquynhproNo ratings yet
- Body Fluids 1 and 2: ObejctivesDocument15 pagesBody Fluids 1 and 2: ObejctivesJoanne Bernadette AguilarNo ratings yet
- Test Taking StrategiesDocument85 pagesTest Taking StrategiesNyjil Patrick Basilio ColumbresNo ratings yet
- St. Luke's College of Nursing: CVD Infarct, RightDocument19 pagesSt. Luke's College of Nursing: CVD Infarct, RightMercicae ANo ratings yet
- Demystifying HyponatremiaDocument10 pagesDemystifying HyponatremiaJavier Vivanco100% (1)
- Eman Question MSDocument6 pagesEman Question MSPaul ignacioNo ratings yet
- Lect15&16 Fluids&ElectrolytesDocument77 pagesLect15&16 Fluids&Electrolyteskhurram na100% (1)
- NCLEX Select All That Apply Practice ExamDocument58 pagesNCLEX Select All That Apply Practice ExamJasmine Jarap100% (2)
- Assessment and Management of Patients With Endocrine DisordersDocument55 pagesAssessment and Management of Patients With Endocrine Disorderseliza marie luisNo ratings yet
- Fluids and Electrolytes - ExamDocument6 pagesFluids and Electrolytes - ExamLouie Bello60% (5)
- Hyponatremia Algorhythm Concept MapDocument2 pagesHyponatremia Algorhythm Concept Mapnursing concept mapsNo ratings yet
- NCLEX HomeostasisDocument10 pagesNCLEX HomeostasisAngie MandeoyaNo ratings yet
- Hyponatremia Algorithm: Onset Rapid ( 48 Hours) : 3% Onset Rapid ( 48 Hours) : May Consider 3% Nac LDocument2 pagesHyponatremia Algorithm: Onset Rapid ( 48 Hours) : 3% Onset Rapid ( 48 Hours) : May Consider 3% Nac Lmina000005100% (1)