You might also like
- Mental Health and Mental IllnessesDocument108 pagesMental Health and Mental IllnessesVictoria VellaNo ratings yet
- MeaslesDocument16 pagesMeaslesdepan_dkb32No ratings yet
- Surgery PDFDocument4 pagesSurgery PDFJanine Maita BalicaoNo ratings yet
- Sexually Transmitted InfectionsDocument73 pagesSexually Transmitted InfectionsJessa MaeNo ratings yet
- Malignant Pleural EffusionsDocument52 pagesMalignant Pleural EffusionsKai XinNo ratings yet
- Soil Transmitted Helminth PDFDocument90 pagesSoil Transmitted Helminth PDFMinarni HoNo ratings yet
- Disaster Continuum: Scaling The Heights of Flexible LearningDocument25 pagesDisaster Continuum: Scaling The Heights of Flexible LearningKRIZIA ANE A. SULONGNo ratings yet
- TRANS - Pediatric Patient ProblemsDocument4 pagesTRANS - Pediatric Patient ProblemsRencel Hope Bañez100% (1)
- Topic Outline: Elements of Parasitology (3P's) Types of Association of Living OrganismsDocument6 pagesTopic Outline: Elements of Parasitology (3P's) Types of Association of Living OrganismsJhunrick Corpuz TumpalanNo ratings yet
- Pharma - SkinDocument8 pagesPharma - Skinreference books100% (1)
- MED1 Samplex Rationale 9 - Breast ExaminationDocument4 pagesMED1 Samplex Rationale 9 - Breast ExaminationMartina GarciaNo ratings yet
- Brief Notes On PharmacovigilanceDocument78 pagesBrief Notes On Pharmacovigilancejay100% (1)
- Acidfaststaining 140111210509 Phpapp02Document16 pagesAcidfaststaining 140111210509 Phpapp02AnjuNo ratings yet
- (EPI) 2.06 Community Diagnosis - DR - ZuluetaDocument4 pages(EPI) 2.06 Community Diagnosis - DR - ZuluetapasambalyrradjohndarNo ratings yet
- Week 4 - Disaster Management ContinuumDocument42 pagesWeek 4 - Disaster Management Continuumirish felixNo ratings yet
- Physiologic MonitoringDocument4 pagesPhysiologic MonitoringAimie DagaleaNo ratings yet
- Belizario VicenteDocument15 pagesBelizario VicenteRoshanDavidNo ratings yet
- 1.2 Immunity Response TransDocument10 pages1.2 Immunity Response TransJoshua SaanNo ratings yet
- Filaria - A Comprehensive StudyDocument63 pagesFilaria - A Comprehensive StudyDayledaniel SorvetoNo ratings yet
- Department of Health - Prevention and Control of Chronic Lifestyle Related Non Communicable Diseases - 2012-02-15Document7 pagesDepartment of Health - Prevention and Control of Chronic Lifestyle Related Non Communicable Diseases - 2012-02-15daryl ann dep-asNo ratings yet
- Community Health NursingDocument91 pagesCommunity Health NursingJanelle Gift SenarloNo ratings yet
- MedSurg Nursing Clinical-Concept Map-2Document3 pagesMedSurg Nursing Clinical-Concept Map-2adaezeNo ratings yet
- Epydemiologi AmebiasisDocument6 pagesEpydemiologi AmebiasisRizal FajriNo ratings yet
- Bio 2 Quiz ReviewerDocument2 pagesBio 2 Quiz ReviewerAlexandra RoderoNo ratings yet
- Department of Health - Persons With Disabilities - 2011-10-26Document9 pagesDepartment of Health - Persons With Disabilities - 2011-10-26daryl ann dep-asNo ratings yet
- Pedia-Reviewer CompleteDocument36 pagesPedia-Reviewer CompletePotato BroNo ratings yet
- Palliative Sedation Therapy in The Last Weeks of Life: A Literature Review and Recommendations For StandardsDocument19 pagesPalliative Sedation Therapy in The Last Weeks of Life: A Literature Review and Recommendations For StandardsMárcia MatosNo ratings yet
- Category Type of Exposure ManagementDocument10 pagesCategory Type of Exposure ManagementDianne GalangNo ratings yet
- Burton's Microbiology Chapter 1Document3 pagesBurton's Microbiology Chapter 1Micole Paz LopezNo ratings yet
- Department of Health - Adolescent and Youth Health Program (AYHP) - 2011-10-27Document8 pagesDepartment of Health - Adolescent and Youth Health Program (AYHP) - 2011-10-27daryl ann dep-asNo ratings yet
- Malaria Control Program: Printer-Friendly PDFDocument3 pagesMalaria Control Program: Printer-Friendly PDFdaryl ann dep-asNo ratings yet
- Admistration of Controlled Narcotic and Controlled Non-Narcotic MedicationsDocument37 pagesAdmistration of Controlled Narcotic and Controlled Non-Narcotic MedicationsKrezielDulosEscobarNo ratings yet
- Department of Health - National Tuberculosis Control Program - 2012-02-08Document5 pagesDepartment of Health - National Tuberculosis Control Program - 2012-02-08daryl ann dep-asNo ratings yet
- ICN Framework of Disaster NursingDocument18 pagesICN Framework of Disaster NursingKRIZIA ANE A. SULONG100% (1)
- Ordonnances: 170 Prescriptions Courantes en MédecineDocument323 pagesOrdonnances: 170 Prescriptions Courantes en MédecineGeeky Nurd100% (1)
- Primary Health CareDocument7 pagesPrimary Health CareJesena SalveNo ratings yet
- Communicable DiseaseDocument41 pagesCommunicable DiseaseMrz AlzNo ratings yet
- Cpm12th RabiesDocument15 pagesCpm12th RabiesKaren ArchesNo ratings yet
- Wound DressingDocument11 pagesWound DressingKRIZIA ANE A. SULONGNo ratings yet
- PHC2. The Philippine Health Care Delivery SystemDocument55 pagesPHC2. The Philippine Health Care Delivery SystemHumilyn NgayawonNo ratings yet
- MS CourseTask10Document2 pagesMS CourseTask10Aria67% (3)
- National Rabies Prevention and Control Program: Printer-Friendly PDFDocument3 pagesNational Rabies Prevention and Control Program: Printer-Friendly PDFdaryl ann dep-asNo ratings yet
- Department of Health - Licensure Examinations For Paraprofessionals Undertaken by The Department of Health - 2011-10-19Document5 pagesDepartment of Health - Licensure Examinations For Paraprofessionals Undertaken by The Department of Health - 2011-10-19daryl ann dep-asNo ratings yet
- Abdominal AbscessDocument3 pagesAbdominal AbscessIchalAzNo ratings yet
- Doh Updated Prog M-RDocument49 pagesDoh Updated Prog M-Rdeeday echavezNo ratings yet
- Communicable Disease: Brent Hospital and Colleges IncorporatedDocument3 pagesCommunicable Disease: Brent Hospital and Colleges IncorporatedJay AbasoloNo ratings yet
- Trichuris Trichiura: Lecture By: Maha Gamal AldeinDocument20 pagesTrichuris Trichiura: Lecture By: Maha Gamal AldeinMohammad DweibNo ratings yet
- CHN Lec FinalsDocument33 pagesCHN Lec FinalsAkashi SilvanoNo ratings yet
- Ecology: of The Disease or Dynamic of Disease Transmission Chapter TwoDocument42 pagesEcology: of The Disease or Dynamic of Disease Transmission Chapter TwoCabdi WaliNo ratings yet
- Technological University of The PhilippinesDocument91 pagesTechnological University of The Philippinessylvia tullerNo ratings yet
- Questions in HRDP-COPAR LectureDocument2 pagesQuestions in HRDP-COPAR LectureEugene RexNo ratings yet
- Microscopic Morphology Myocardial InfarctionDocument10 pagesMicroscopic Morphology Myocardial InfarctionnathanielNo ratings yet
- Poliomyeli TIS: Name:Nurzawani Binti Shamsudin Matric No: 0918424Document19 pagesPoliomyeli TIS: Name:Nurzawani Binti Shamsudin Matric No: 0918424Jerryuk20100% (1)
- Unified DTRDocument1 pageUnified DTRJay AdamzNo ratings yet
- Lecture 2-Introduction To MicroscopesDocument26 pagesLecture 2-Introduction To MicroscopesThuto SmithNo ratings yet
- Entamoeba HistolyticaDocument38 pagesEntamoeba HistolyticaAbdul Ghafar OrakzaiiiNo ratings yet
- Department of Health - Expanded Program On Immunization - 2012-05-16Document7 pagesDepartment of Health - Expanded Program On Immunization - 2012-05-16MasterclassNo ratings yet
- Fluid and Elctrolyte Balance.... Power PointDocument40 pagesFluid and Elctrolyte Balance.... Power PointMarwan M.100% (1)
- Blood and Tissue ProtozoaDocument32 pagesBlood and Tissue ProtozoaFort SalvadorNo ratings yet
- Department of Health - Knock Out Tigdas 2007 - 2011-10-19Document3 pagesDepartment of Health - Knock Out Tigdas 2007 - 2011-10-19daryl ann dep-asNo ratings yet
- Reversible and Irreversible Cell InjuryDocument55 pagesReversible and Irreversible Cell Injurygabb bbNo ratings yet
- CHN - Rabies Control ProgramDocument16 pagesCHN - Rabies Control ProgramJoseph KentNo ratings yet
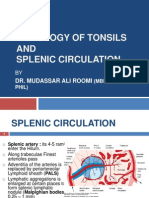
- Histology of Tonsil and Splenic Circulation by Dr. RoomiDocument21 pagesHistology of Tonsil and Splenic Circulation by Dr. RoomiMudassar RoomiNo ratings yet
- Levanthan Short Ans KeyDocument42 pagesLevanthan Short Ans Keyxyab.varga.swuNo ratings yet
- Measles: PGI Nicole Jenne C. TanDocument40 pagesMeasles: PGI Nicole Jenne C. TanNicole Jenne TanNo ratings yet
- 3.3 Family PlanningDocument9 pages3.3 Family PlanningGayle Regine DaquialNo ratings yet
- M1 - Urinary DisordersDocument2 pagesM1 - Urinary DisordersjuiceNo ratings yet
- Pertusis TreatmentDocument20 pagesPertusis TreatmentJaipratap SinghNo ratings yet
- National Leprosy Control ProgramDocument3 pagesNational Leprosy Control ProgramKrizle AdazaNo ratings yet
- Doh ProgramsDocument45 pagesDoh ProgramsVon Andre AposagaNo ratings yet
- Liceo de Cagayan University: College of NursingDocument3 pagesLiceo de Cagayan University: College of NursingKRIZIA ANE A. SULONGNo ratings yet
- 24 Hour Urine CollectionDocument11 pages24 Hour Urine CollectionKRIZIA ANE A. SULONGNo ratings yet
- 6 Filariasis Elimination ProgramDocument5 pages6 Filariasis Elimination ProgramKRIZIA ANE A. SULONGNo ratings yet
- Sulong, Krizia Ane A - TLGDocument2 pagesSulong, Krizia Ane A - TLGKRIZIA ANE A. SULONGNo ratings yet
- Liceo de Cagayan University: College of NursingDocument1 pageLiceo de Cagayan University: College of NursingKRIZIA ANE A. SULONGNo ratings yet
- Group 2: Abulag, Cahiles, Domondon, Galdo, Mancao, Melicor, Roxas, Sulong, Tagapulot, YanchaDocument6 pagesGroup 2: Abulag, Cahiles, Domondon, Galdo, Mancao, Melicor, Roxas, Sulong, Tagapulot, YanchaKRIZIA ANE A. SULONGNo ratings yet
- MLE: Meaningful Learning Experience: Second Semester, Academic Year - 2020-2021Document1 pageMLE: Meaningful Learning Experience: Second Semester, Academic Year - 2020-2021KRIZIA ANE A. SULONGNo ratings yet
- Iloilo Doctors' Hospital, Inc. Department of Internal MedicineDocument10 pagesIloilo Doctors' Hospital, Inc. Department of Internal MedicineAllison Eunice ServandoNo ratings yet
- Grade One Ankle Sprain Recovery TimeDocument4 pagesGrade One Ankle Sprain Recovery TimeMattNo ratings yet
- 2017 2018 Cib - Digital Final PDFDocument101 pages2017 2018 Cib - Digital Final PDFRo KohnNo ratings yet
- 2018.5.15 Insite Colo ContentDocument21 pages2018.5.15 Insite Colo ContentKatrinaBennettNo ratings yet
- Toxic Megacolon: Daniel M. Autenrieth, MD, and Daniel C. Baumgart, MD, PHDDocument8 pagesToxic Megacolon: Daniel M. Autenrieth, MD, and Daniel C. Baumgart, MD, PHDGoran TomićNo ratings yet
- Mood Disorders: Anda Gershon & Renee ThompsonDocument26 pagesMood Disorders: Anda Gershon & Renee ThompsonSimón Ortiz LondoñoNo ratings yet
- Endobronchial Valves For Severe EmphysemaDocument7 pagesEndobronchial Valves For Severe EmphysemairfanNo ratings yet
- Steps in Viral Pathogenesis-Lecture ThreeDocument3 pagesSteps in Viral Pathogenesis-Lecture ThreeIM CTNo ratings yet
- Nursing Process: Mrs. Sumaira Noreen Senior Nursing InstructorDocument40 pagesNursing Process: Mrs. Sumaira Noreen Senior Nursing InstructorSumaira NoreenNo ratings yet
- Multiple PregnancyDocument21 pagesMultiple PregnancyMazlina Maidin100% (1)
- Ac 72Document5 pagesAc 72Giovani TardiniNo ratings yet
- Mapehhealth Q3 Summative-TestDocument2 pagesMapehhealth Q3 Summative-Testelle VeeNo ratings yet
- ComplementDocument39 pagesComplementYeyeh SantosNo ratings yet
- Covid19 Vaccination Report Personnel LearnerDocument39 pagesCovid19 Vaccination Report Personnel LearnerAnalyn SamillanoNo ratings yet
- Rawatan: Kecelaruan Tingkah Laku. Kuala Lumpur: PTS Profesional PublisherDocument2 pagesRawatan: Kecelaruan Tingkah Laku. Kuala Lumpur: PTS Profesional PublisherNeng Azreen ZGNo ratings yet
- Health AssessmentDocument23 pagesHealth AssessmentPORTRAIT OF A NURSENo ratings yet
- Nueva Ecija University of Science and Technology: Case 7Document7 pagesNueva Ecija University of Science and Technology: Case 7jomariNo ratings yet
- Infective EndocarditisDocument58 pagesInfective EndocarditisTok KeawkaewNo ratings yet
- He Ma To Pathology MilestonesDocument21 pagesHe Ma To Pathology MilestonesCristyan David Quintero MuneraNo ratings yet
- 4 High Frequency VentilationDocument40 pages4 High Frequency Ventilationk0601828No ratings yet
- ISPD Peritonitis Guideline Recommendations: 2022 Update On Prevention and TreatmentDocument44 pagesISPD Peritonitis Guideline Recommendations: 2022 Update On Prevention and TreatmentMisael JimenezNo ratings yet
- Chapter 32. ConstipationDocument14 pagesChapter 32. ConstipationDiana F. MoscosoNo ratings yet
- Forensic Age EstimationDocument10 pagesForensic Age EstimationMaría Camila ValenciaNo ratings yet