You might also like
- Chemistry by K L Chugh Class 11 PDFDocument4 pagesChemistry by K L Chugh Class 11 PDFAshim Sinha17% (6)
- A-Level Biology Notes: By: Bianca HimawanDocument86 pagesA-Level Biology Notes: By: Bianca HimawanLauren Chikwehwa100% (3)
- Biochem CH 25 Nucleotide BiosynthesisDocument6 pagesBiochem CH 25 Nucleotide BiosynthesisSchat ZiNo ratings yet
- The Sliding Filament Theory Visual ModelDocument1 pageThe Sliding Filament Theory Visual ModelzephyrverliceNo ratings yet
- Lifs 1902 Muscle Lecture #2 2021-1Document109 pagesLifs 1902 Muscle Lecture #2 2021-1KenjiNo ratings yet
- Beneficent: - in The Name of Almighty Allah, The Merciful, TheDocument15 pagesBeneficent: - in The Name of Almighty Allah, The Merciful, TheKhalid MajidNo ratings yet
- Mitochondrion 03Document53 pagesMitochondrion 03api-19916399No ratings yet
- FTNS-3101-Oxidative PhosphorylationDocument4 pagesFTNS-3101-Oxidative PhosphorylationMd. Muhaiminul IslamNo ratings yet
- Biochemistry: A Short Course: The Proton Motive ForceDocument19 pagesBiochemistry: A Short Course: The Proton Motive ForceEli JohnsonNo ratings yet
- Motors 2020Document94 pagesMotors 2020azazel666No ratings yet
- Demonstration Practical 4 Micro Biology2323Document3 pagesDemonstration Practical 4 Micro Biology2323Meet ManiyaNo ratings yet
- Muscle PDFDocument46 pagesMuscle PDFJalo SutariNo ratings yet
- Photosynthesis March - AprilDocument40 pagesPhotosynthesis March - AprilIbrahim TurayNo ratings yet
- Grade-11 General-Biology-1 Q2 Wk7 GLAKDocument20 pagesGrade-11 General-Biology-1 Q2 Wk7 GLAKClarisse De GuiaNo ratings yet
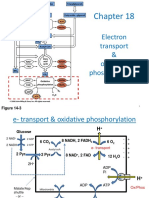
- Electron Transport & Oxidative Phosphorylation: Figure 14-3Document73 pagesElectron Transport & Oxidative Phosphorylation: Figure 14-3Stephanie Abisola AkingbadeNo ratings yet
- Second LectrueDocument44 pagesSecond Lectrueapi-3700537No ratings yet
- Bioenergetics MD PhysiothDocument70 pagesBioenergetics MD PhysioththestaffforpediatricptNo ratings yet
- 07 Muscle Slides BDocument57 pages07 Muscle Slides BBalew KassieNo ratings yet
- ATP Synthase StructureDocument36 pagesATP Synthase Structurekiran kombeNo ratings yet
- USMLE Step 1 First Aid 2021-101-230Document130 pagesUSMLE Step 1 First Aid 2021-101-230mariana yllanesNo ratings yet
- Amino Acids: Proteins and EnzymesDocument32 pagesAmino Acids: Proteins and EnzymesJay PandaNo ratings yet
- Muscle BiochemistryDocument19 pagesMuscle BiochemistrySantino MajokNo ratings yet
- Plan For Today: Finish Up With Electron Transport Chain and Oxidative PhosphorylationDocument52 pagesPlan For Today: Finish Up With Electron Transport Chain and Oxidative PhosphorylationKalai KrishnamurthyNo ratings yet
- 7 Actin Bascis Regulation and MuscleDocument25 pages7 Actin Bascis Regulation and Musclezj5bnxbymzNo ratings yet
- Metabolic PathwaysDocument6 pagesMetabolic Pathwaysgelary sousaNo ratings yet
- Photosynthesis 1 20210413 103416Document33 pagesPhotosynthesis 1 20210413 103416Abenathi NolusuNo ratings yet
- Q2W3Document3 pagesQ2W3Jihyun KimNo ratings yet
- XAVI PHOTOSYNTHESIS - Lecture BIOUMUMDocument47 pagesXAVI PHOTOSYNTHESIS - Lecture BIOUMUMPrita YhuniNo ratings yet
- Photosynthesis Worksheet 2 KeyDocument7 pagesPhotosynthesis Worksheet 2 KeysarfarazNo ratings yet
- Screenshot 2023-08-18 at 11.00.26 PMDocument99 pagesScreenshot 2023-08-18 at 11.00.26 PMAbod AbodNo ratings yet
- General Biology ReviewerDocument13 pagesGeneral Biology Reviewerzoe dizonNo ratings yet
- Oxidative Phosphorylation PDFDocument33 pagesOxidative Phosphorylation PDFdvdss29No ratings yet
- Week 1 ADP & ATP CycleDocument17 pagesWeek 1 ADP & ATP Cycledenveralbarico143No ratings yet
- Cellular - Metabolism 1Document26 pagesCellular - Metabolism 1Ans JavidNo ratings yet
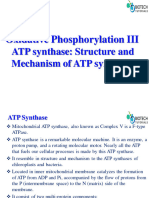
- Oxidative Phosphorylation and Electron Transport Chain III ATP Synthase Structure and FunctionDocument17 pagesOxidative Phosphorylation and Electron Transport Chain III ATP Synthase Structure and FunctionIffatnazNo ratings yet
- 1BMS1153 BL1-Energy MetabolismDocument35 pages1BMS1153 BL1-Energy Metabolismshakila786No ratings yet
- M8 Microbial MetabolismDocument56 pagesM8 Microbial MetabolismFares SamirNo ratings yet
- Lehninger ElectronTransportDocument20 pagesLehninger ElectronTransportZahid AliNo ratings yet
- Biology: By-Dr - Darshan PandaDocument21 pagesBiology: By-Dr - Darshan PandaMaggieSamNo ratings yet
- 1 Atp-AdpDocument19 pages1 Atp-AdpZhaira Anne AngelesNo ratings yet
- Regulation of Metabolic Pathways: Limited Number of Regulatory Enzymes Negative FeedbackDocument12 pagesRegulation of Metabolic Pathways: Limited Number of Regulatory Enzymes Negative FeedbackTheophilus BaidooNo ratings yet
- 111 - 1 Nutrition 14Document133 pages111 - 1 Nutrition 14Wei Liong SiaNo ratings yet
- Comentatory MbbsDocument7 pagesComentatory MbbsSai SreedharNo ratings yet
- Respiration DiagramDocument3 pagesRespiration Diagramapi-521781723No ratings yet
- CHO L5, L6 Metabolisim 2nd NutriDocument48 pagesCHO L5, L6 Metabolisim 2nd NutriLeena KhaledNo ratings yet
- ATPsyntasa PDFDocument9 pagesATPsyntasa PDFOsiithaa CañaszNo ratings yet
- 2017 PosterDocument1 page2017 PostertilamisuNo ratings yet
- Optical AmplifiersDocument89 pagesOptical AmplifiersBruno BrandãoNo ratings yet
- BiologicalReview29 4 ATP PresentationDocument21 pagesBiologicalReview29 4 ATP Presentationsmithsashay74No ratings yet
- Structure of ATP: RiboseDocument1 pageStructure of ATP: RiboseAuriceliaOliveiraNo ratings yet
- Pages From Lange Bio FlashcardDocument4 pagesPages From Lange Bio Flashcardsepanta2002No ratings yet
- 2017-29-Digoxin and Amiodarone (A Vorster)Document10 pages2017-29-Digoxin and Amiodarone (A Vorster)Sadiq ZakariaNo ratings yet
- Lecture 30: Electron Transport & ATP Synthesis Electron TransportDocument3 pagesLecture 30: Electron Transport & ATP Synthesis Electron TransportmoyayeNo ratings yet
- Biochem CH 24 Amino Acid BiosynthesisDocument6 pagesBiochem CH 24 Amino Acid BiosynthesisSchat ZiNo ratings yet
- Ch23 RespirationDocument66 pagesCh23 RespirationNectaryNo ratings yet
- ETC NotesDocument3 pagesETC Notesaminahali04.aaNo ratings yet
- Biological Oxidation ETCDocument37 pagesBiological Oxidation ETCsanofazal786No ratings yet
- 1 - ATP-ADP - CycleDocument10 pages1 - ATP-ADP - CycleYay SandovalNo ratings yet
- Oksidasi BiologiDocument62 pagesOksidasi BiologisenadaNo ratings yet
- Proteins 1Document15 pagesProteins 1missyclaudia084No ratings yet
- Assembly Instructions for Polypeptide Models: Academic Press/Molecular Design Inc. Precision Molecular ModelsFrom EverandAssembly Instructions for Polypeptide Models: Academic Press/Molecular Design Inc. Precision Molecular ModelsNo ratings yet
- Microbiology IntroductionDocument37 pagesMicrobiology IntroductionrnrmmanphdNo ratings yet
- Roles and Mechanisms of Hawthorn and Its ExtractsDocument12 pagesRoles and Mechanisms of Hawthorn and Its ExtractsHomer SimpsonNo ratings yet
- Vincent Et Al (L. Stuani - JE Sarry)Document14 pagesVincent Et Al (L. Stuani - JE Sarry)BELEN ROSERONo ratings yet
- sIM3 - Complement System - 22Document37 pagessIM3 - Complement System - 22Brian LeungNo ratings yet
- Difference of Broad Spectrum & Narrow Spectrum AntibioticsDocument36 pagesDifference of Broad Spectrum & Narrow Spectrum AntibioticsAFTAB H. ABBASINo ratings yet
- DNA Replication Sequencing Revision 2017Document58 pagesDNA Replication Sequencing Revision 2017Daniel sifuentes garciaNo ratings yet
- National Antibiotic Pedia GuidelinesDocument149 pagesNational Antibiotic Pedia GuidelinesGg GreyNo ratings yet
- 3 Locatelli2022Document13 pages3 Locatelli20226hrtn5jvz6No ratings yet
- Blood GroupingDocument8 pagesBlood GroupingdevarajNo ratings yet
- Comparative Analysis Among Pathogenic Fungal Species That Cause Gladiolus (Gladiolus Grandiflorus Hort.) Corm Rot in MexicoDocument8 pagesComparative Analysis Among Pathogenic Fungal Species That Cause Gladiolus (Gladiolus Grandiflorus Hort.) Corm Rot in MexicoCitlalli BrionesNo ratings yet
- 21 Health Benefits of Bitter KolaDocument4 pages21 Health Benefits of Bitter Kolaserjio47No ratings yet
- MoLGen - DNA Structure PDFDocument42 pagesMoLGen - DNA Structure PDFKaileen May SaballoNo ratings yet
- Histology Mock ExamDocument73 pagesHistology Mock ExamRozen GaiserNo ratings yet
- Effects of Avocado/soybean Unsaponifiables (ASU) On The Treatment of Ligature-Induced Periodontitis in RatsDocument11 pagesEffects of Avocado/soybean Unsaponifiables (ASU) On The Treatment of Ligature-Induced Periodontitis in RatsYon AditamaNo ratings yet
- Efficacy of Carica Papaya Enzyme As Antibacterial Hand SanitizerDocument18 pagesEfficacy of Carica Papaya Enzyme As Antibacterial Hand SanitizerAnna Garcia BuquidNo ratings yet
- LBUTherputic ProductsNov16 PDFDocument12 pagesLBUTherputic ProductsNov16 PDFHimanshu Dwivedi100% (1)
- Fcps PaediatricsDocument499 pagesFcps PaediatricsTahniat AishaNo ratings yet
- Microbiota-Gut-Brain Axis and Nutritional Strategy Under Heat StressDocument8 pagesMicrobiota-Gut-Brain Axis and Nutritional Strategy Under Heat StressJessica MarcellineNo ratings yet
- Acute Gingival Infection Lecture - pdf-1251132185Document68 pagesAcute Gingival Infection Lecture - pdf-1251132185irajput 001No ratings yet
- Biotech Reviewer 2nd Qtr. GRADE 8Document4 pagesBiotech Reviewer 2nd Qtr. GRADE 8Andrew P. Rico0% (1)
- Pharma Cards CHF DVTDocument14 pagesPharma Cards CHF DVTRiza Angela BarazanNo ratings yet
- Analysis of Pulpal Reactions To Restorative Procedures, Materials, Pulp Capping, and Future TherapiesDocument12 pagesAnalysis of Pulpal Reactions To Restorative Procedures, Materials, Pulp Capping, and Future TherapiesAmr EldokNo ratings yet
- Ntestinal Intraepithelial LymphocytesDocument21 pagesNtestinal Intraepithelial LymphocytesEDGAR FUENMAYOR PIRELANo ratings yet
- What Is A Point MutationDocument6 pagesWhat Is A Point MutationDesi Steve JobsNo ratings yet
- Antibiotics CologyDocument31 pagesAntibiotics CologyManthan ChauhanNo ratings yet
- Mutation: - From The Latin Word "Mutare" MeansDocument38 pagesMutation: - From The Latin Word "Mutare" MeansJan Andrea BendijoNo ratings yet
- Criteria # Efficacy Points + + + +: Doltegravir/Abaravir/LamividuneDocument5 pagesCriteria # Efficacy Points + + + +: Doltegravir/Abaravir/LamividuneValerie Gonzaga-CarandangNo ratings yet
- Basic Microbiology and Infection Control For Midwives-4Document207 pagesBasic Microbiology and Infection Control For Midwives-4rehanaNo ratings yet
- WBI01 01 Rms 20180308 PDFDocument21 pagesWBI01 01 Rms 20180308 PDFxinyu wuNo ratings yet