You might also like
- Specification of GuardrailDocument5 pagesSpecification of Guardrailmehrdad_so1981No ratings yet
- Concrete Lab ManualDocument42 pagesConcrete Lab ManualVENKATA RANGANADHNo ratings yet
- Drainage Gradients FallsDocument5 pagesDrainage Gradients FallsAnonymous Of0C4dNo ratings yet
- Standard-Deviation-for-Concrete CalculationDocument13 pagesStandard-Deviation-for-Concrete CalculationPrabhakar SvNo ratings yet
- Checklist For Rock Bolts PDFDocument4 pagesChecklist For Rock Bolts PDFImran FarooqNo ratings yet
- SEVEN Materials (MIR) Work (WIR) Inspection Requests Procedure 0DMQL00-DLVR-00-SEV-QM-PRO-00005Document11 pagesSEVEN Materials (MIR) Work (WIR) Inspection Requests Procedure 0DMQL00-DLVR-00-SEV-QM-PRO-00005Meshaal ALBalharithNo ratings yet
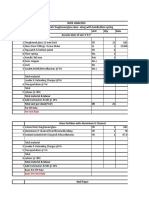
- Rate analysis for glass doors, partitions and signagesDocument6 pagesRate analysis for glass doors, partitions and signagesAnonymous Of0C4d75% (4)
- Lifting Capacity Enhancement of A Crawler Crane by Improving StabilityDocument9 pagesLifting Capacity Enhancement of A Crawler Crane by Improving StabilitygsoldatosNo ratings yet
- ISO 9001:2015 Quality Management System: Risk & Opportunities Assessment RecordDocument1 pageISO 9001:2015 Quality Management System: Risk & Opportunities Assessment RecordkarthikumarnpNo ratings yet
- How To Unprotect Excel Sheet Without PasswordDocument3 pagesHow To Unprotect Excel Sheet Without PasswordAnonymous Of0C4dNo ratings yet
- Inspection and test plan for retaining wall constructionDocument11 pagesInspection and test plan for retaining wall constructionBangkit SamosirNo ratings yet
- Audit Notification FormDocument10 pagesAudit Notification FormResearcherNo ratings yet
- Cube Test ReportDocument1 pageCube Test ReportShubham MareNo ratings yet
- Isolated Footing Design (BS 8110-97) : Footing No. Group ID Foundation Geometry - Length Width ThicknessDocument10 pagesIsolated Footing Design (BS 8110-97) : Footing No. Group ID Foundation Geometry - Length Width ThicknessAnonymous mWTB5TaMANNo ratings yet
- Quantum of Check of Material&WorkmanshipDocument35 pagesQuantum of Check of Material&Workmanshipsanjay vidhateNo ratings yet
- Concrete Technical SpecificationDocument44 pagesConcrete Technical SpecificationNgoc BangNo ratings yet
- J910-DH02-P10ZEN-040004 Field ITP For Shotcrete Work For Ash Handling Facilities - Rev. 0 (AFC)Document13 pagesJ910-DH02-P10ZEN-040004 Field ITP For Shotcrete Work For Ash Handling Facilities - Rev. 0 (AFC)rudi sarifudinNo ratings yet
- Date: Plaster Commencement Permission Name of The Work: Floor Drawing No. Location Sr. No. Check PointsDocument2 pagesDate: Plaster Commencement Permission Name of The Work: Floor Drawing No. Location Sr. No. Check PointsAnonymous Of0C4dNo ratings yet
- Astm A 123 - 2013Document8 pagesAstm A 123 - 2013JOSENo ratings yet
- Inspection & Test Plan (Itp) : Road WorkDocument1 pageInspection & Test Plan (Itp) : Road WorkLOPA THANDARNo ratings yet
- WSDOT FOP for Compressive Strength of Cement MortarsDocument14 pagesWSDOT FOP for Compressive Strength of Cement Mortarsmalaya tripathyNo ratings yet
- Concrete Trial Mix Checklist - 01.09.2022Document5 pagesConcrete Trial Mix Checklist - 01.09.2022Pandiaraj VNo ratings yet
- REPORT - Trial Mix Material Grout (Pumpable)Document7 pagesREPORT - Trial Mix Material Grout (Pumpable)Triadi Bagus GumilarNo ratings yet
- Certificate of Compliance: Att: Dorat Al TameerDocument1 pageCertificate of Compliance: Att: Dorat Al TameerMohammad ArslanNo ratings yet
- Method Statement of Lateral Load Test (BHEL ANPARA)Document11 pagesMethod Statement of Lateral Load Test (BHEL ANPARA)sugurpraveenNo ratings yet
- Quality Assurance PlanDocument92 pagesQuality Assurance PlanHariom GuptaNo ratings yet
- TolerancesDocument2 pagesTolerancesAdithya ShourieNo ratings yet
- Equivalent Steel GradesDocument3 pagesEquivalent Steel Gradesbasiri jayadeepNo ratings yet
- Amendment N - I MA Y 2002 IS 1200 (PART 8) : 1993 Methods Measurement of Building and Civil Engineering WorksDocument8 pagesAmendment N - I MA Y 2002 IS 1200 (PART 8) : 1993 Methods Measurement of Building and Civil Engineering Worksraviteja036No ratings yet
- Project - 1: - PROJECT TITLE:-To Reduce Bolt Loosening Problem inDocument38 pagesProject - 1: - PROJECT TITLE:-To Reduce Bolt Loosening Problem inmanpreetNo ratings yet
- Disclosure To Promote The Right To InformationDocument17 pagesDisclosure To Promote The Right To Informationchannakeshava pandurangaNo ratings yet
- PQP - Kilaraipur PDFDocument53 pagesPQP - Kilaraipur PDFVijendra SharmaNo ratings yet
- Novo SPTDocument32 pagesNovo SPTBambang SantosoNo ratings yet
- 141667-FAF-SPE-EOH-000007 OEE Galvanised Structural Steel Specifications PDFDocument12 pages141667-FAF-SPE-EOH-000007 OEE Galvanised Structural Steel Specifications PDFmarigusatuNo ratings yet
- QCP-Soil Investigation WorksDocument9 pagesQCP-Soil Investigation WorksManash Protim GogoiNo ratings yet
- OBS - 510 - Rev 01 - Eng MilliporeDocument4 pagesOBS - 510 - Rev 01 - Eng MilliporeSakthy ArunaNo ratings yet
- Qcs 2010 Section 12 Part 3 Filling PDFDocument4 pagesQcs 2010 Section 12 Part 3 Filling PDFbryanpastor106100% (1)
- NPCIL-SIMPLEX BOUNDARY SLIPPAGE CALCULATIONSDocument4 pagesNPCIL-SIMPLEX BOUNDARY SLIPPAGE CALCULATIONSAnonymous cG5MyHM100% (1)
- Quality Assurance Plan For Civil4mDocument3 pagesQuality Assurance Plan For Civil4mMohammed Abdul BaseerNo ratings yet
- CL Totalgowin Tks202Document2 pagesCL Totalgowin Tks202tjNo ratings yet
- Inspection and Test Plan: Activity: ITP For Inspection of Pile Load Test WorksDocument3 pagesInspection and Test Plan: Activity: ITP For Inspection of Pile Load Test WorksjitendraNo ratings yet
- Support Reactions Footing DesignDocument14 pagesSupport Reactions Footing Designgyan_th9229No ratings yet
- AIMIL Fully Automatic Compression Tester FACTDocument3 pagesAIMIL Fully Automatic Compression Tester FACTvasudeva yasasNo ratings yet
- ASTM D 5780-95 Standard Test Method For Individual Piles in Permafrost Under Static Axial Compressive LoadDocument14 pagesASTM D 5780-95 Standard Test Method For Individual Piles in Permafrost Under Static Axial Compressive LoadPablo Antonio Valcárcel Vargas100% (1)
- Rocky Construction 1st Running Bill for Conveyor Belt FoundationDocument5 pagesRocky Construction 1st Running Bill for Conveyor Belt Foundationanon_388492125No ratings yet
- Astm D3282 93 - 260421Document6 pagesAstm D3282 93 - 260421Mark D VillanuevaNo ratings yet
- Sand Calibration FormetDocument2 pagesSand Calibration FormetAnish PanchalNo ratings yet
- Method Statement For Sub Grade: Project Procedure Plan - Fipl#2, Phase 1Document4 pagesMethod Statement For Sub Grade: Project Procedure Plan - Fipl#2, Phase 1HARIOM GUPTANo ratings yet
- 20Document1 page20Khizer IslamNo ratings yet
- Concrete Mix Design K175 KGDocument1 pageConcrete Mix Design K175 KGWiditra Fetty PurbaNo ratings yet
- TH ND: 2) The Results Are Related To The Test Performed at Location Shown by ClientDocument16 pagesTH ND: 2) The Results Are Related To The Test Performed at Location Shown by Clientakshay kothiyalNo ratings yet
- ITP For Fabrication & Installation of Tensile Fabric ShadesDocument1 pageITP For Fabrication & Installation of Tensile Fabric ShadesSun ShadeNo ratings yet
- Qualification RangeDocument1 pageQualification RangeSARSAN NDTNo ratings yet
- Flexural Modulus of Elasticity of Dimension Stone: Standard Test Method ForDocument3 pagesFlexural Modulus of Elasticity of Dimension Stone: Standard Test Method ForRufo CascoNo ratings yet
- Hardness Conversion ChartDocument10 pagesHardness Conversion ChartAshutosh SinghNo ratings yet
- Guid PlasteringDocument2 pagesGuid PlasteringBozzay TamásNo ratings yet
- Concrete inspection reportDocument1 pageConcrete inspection reportRangga GautamaNo ratings yet
- S21-CnS Roads and DrainsDocument39 pagesS21-CnS Roads and DrainsLukeNo ratings yet
- Invoice Cum Material Issue Voucher: Miv No. CWC No. CWC Date: Sap Material Document No. Posting DateDocument1 pageInvoice Cum Material Issue Voucher: Miv No. CWC No. CWC Date: Sap Material Document No. Posting Datehimanshu kalraNo ratings yet
- Anti CarbonationDocument4 pagesAnti Carbonationraja qammarNo ratings yet
- AMANA Specs-ASHPHALTIC CONCRETE WORKSDocument25 pagesAMANA Specs-ASHPHALTIC CONCRETE WORKSJishad NalakathNo ratings yet
- Bridge Design Format For Rural Road NQM Project AssamDocument35 pagesBridge Design Format For Rural Road NQM Project Assamarif ahmedNo ratings yet
- Pmay UDocument14 pagesPmay UAnonymous Of0C4d100% (1)
- Presentation On E-Measurement BookDocument22 pagesPresentation On E-Measurement BookAnonymous Of0C4dNo ratings yet
- How To Unprotect Excel SheetDocument1 pageHow To Unprotect Excel SheetAnonymous Of0C4dNo ratings yet
- Brick Work CPDocument2 pagesBrick Work CPAnonymous Of0C4dNo ratings yet
- EOI FOR PROFESSIONAL CONSULTANTS EMPANELMENTDocument89 pagesEOI FOR PROFESSIONAL CONSULTANTS EMPANELMENTAnonymous Of0C4dNo ratings yet
- Self-Focusing of Laser BeamDocument21 pagesSelf-Focusing of Laser BeamAnonymous Of0C4dNo ratings yet
- Short SpecificationsDocument6 pagesShort SpecificationsAnonymous Of0C4dNo ratings yet
- Module 2.7: Environmental and Social SafeguardsDocument92 pagesModule 2.7: Environmental and Social SafeguardsAnonymous Of0C4dNo ratings yet
- CLSS Leaflet EWS LIG EnglishDocument2 pagesCLSS Leaflet EWS LIG EnglishAnonymous Of0C4dNo ratings yet
- Simplifed Manning Formula TableDocument4 pagesSimplifed Manning Formula TableAnonymous Of0C4dNo ratings yet
- Fisibility Chart of RedevelopmentDocument4 pagesFisibility Chart of RedevelopmentAnonymous Of0C4dNo ratings yet
- Hazen and William's FormulaDocument1 pageHazen and William's FormulaAnonymous Of0C4dNo ratings yet
- 02A CLSS MIG Leaflet EnglishDocument2 pages02A CLSS MIG Leaflet EnglishAnonymous Of0C4dNo ratings yet
- Build RADocument14 pagesBuild RAAnonymous Of0C4dNo ratings yet
- Ann. 1 - Study FormatDocument4 pagesAnn. 1 - Study FormatAnonymous Of0C4dNo ratings yet
- PMAY(U) Beneficiary Led Construction and EnhancementDocument2 pagesPMAY(U) Beneficiary Led Construction and EnhancementAnonymous Of0C4dNo ratings yet
- PMAY Single LeafletDocument2 pagesPMAY Single LeafletAnonymous Of0C4dNo ratings yet
- 03 AHP Leaflet EnglishDocument2 pages03 AHP Leaflet EnglishAnonymous Of0C4dNo ratings yet
- 00 PMAY Leaflet EnglishDocument2 pages00 PMAY Leaflet EnglishAnonymous Of0C4dNo ratings yet
- Building Estimate RA Based On Pune PWD SRDocument28 pagesBuilding Estimate RA Based On Pune PWD SRAnonymous Of0C4dNo ratings yet
- Building Estimate RA Based On Pune PWD SRDocument28 pagesBuilding Estimate RA Based On Pune PWD SRAnonymous Of0C4dNo ratings yet
- 10 HfapoaDocument25 pages10 HfapoaAnonymous Of0C4dNo ratings yet
- Coloumn Stiff of ColumnDocument4 pagesColoumn Stiff of ColumnAnonymous Of0C4dNo ratings yet
- Unit Qty Rate Sr. No Item Description Item No/Code Amou NT in Rs Labou R Comp Onent Labou R Per SQMDocument3 pagesUnit Qty Rate Sr. No Item Description Item No/Code Amou NT in Rs Labou R Comp Onent Labou R Per SQMAnonymous Of0C4d100% (1)
- Two Slab DistontinuesDocument4 pagesTwo Slab DistontinuesAnonymous Of0C4dNo ratings yet
- 10 HfapoaDocument25 pages10 HfapoaAnonymous Of0C4dNo ratings yet