Professional Documents
Culture Documents
เวชปฎิบัติในการรักษาสิว
เวชปฎิบัติในการรักษาสิว
Uploaded by
Yosawadee VisoottivisethCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
เวชปฎิบัติในการรักษาสิว
เวชปฎิบัติในการรักษาสิว
Uploaded by
Yosawadee VisoottivisethCopyright:
Available Formats
Continuing Medical Education
CME 2 CREDITS
เวชปฏิบัµิในการรักษาโรคสิว: การรักษา*
John Sullivan, MBBS, FACD; Veronica Preda, BSc, MBBS
áปลáละเรียบเรียงâดย นพ.ประวิตร พิศาลบุตร (พ.บ. (เกียรตินิยมอันดับหนึ่ง),
Diplomate, American Board of Dermatology & American Subspecialty Board of Dermatological Immunology)
รหัÊกิ¨กรรม 3-3220-000-9304/101102
แนวทา§
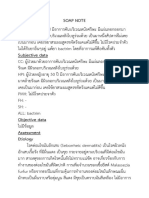
วัµ¶Ø»ระสงค์ รูปทÕè 1. Severe acne in a man in
การรักษาสิว his early 20s
เพื่อให้ทราบถึงแนวทางการรักษาโรคสิว ทั้งในแง่การใช้
ยาทาและยารับประทาน รวมทั้งผลแทรกซ้อนที่ต้องระวังใน โดยทั่วไปแล้ว
การใช้ยารักษาสิวเหล่านี้ พบว่ า ผู้ ป่ ว ยโรคสิ ว
เพศหญิ ง ให้ ค วาม
ร่วมมือในการรักษาที่
รูปแบบµ‹า§æ ในการรักษาสิว ต้องทายาหลายๆ ตัว
ส่วนเพศชายนิยมใช้ Combination therapies, including systemic
ในกรณีที่ผู้ป่วยเป็นโรคสิวมาก ควรใช้แนวทางการรักษาที่ ยาชนิ ด รั บ ประทาน treatments, are required to treat this patient’s
severely inflamed lesions and reduce the risk
ได้ผลเร็วเพื่อช่วยลดการอักเสบซึ่งจะลดโอกาสเสี่ยงต่อการเกิดแผล มากกว่ า ยาทา ใน of further scarring. Such treatment will also
เป็นถาวร การรักษาสิวนั้นอาจใช้แค่ยาทาหรือยารับประทาน หรือ กรณีที่จำาเป็นต้องใช้ provide the basis for long-term control.
ใช้ทั้ง 2 อย่างร่วมกัน ในผู้ป่วยที่เป็นสิวชนิดไม่รุนแรง (mild acne) ยาทาร่ ว มด้ ว ยก็ มั ก
อาจเลือกใช้ยาตัวเดียว (monotherapy) ได้ พบว่าการรักษาโรคสิว จะชอบยาที่ทาเพียงวันละครั้ง พบว่าเมื่ออาการของสิวดีขึ้นผู้ป่วย
โดยการใช้ยาปฏิชีวนะแม้ไม่มีฤทธิ์สลายคอมมีโดน (comedolytic มักขาดแรงจูงใจที่ต้องใช้ยาหลายขนาน จนเมื่อสิวกำาเริบขึ้นมาใหม่
activity) โดยตรง แต่จากลักษณะทางคลินิกก็พบว่าผู้ป่วยมีจำานวน จึงจะสนใจใช้ยาให้ครบ
คอมมีโดนน้อยลงเรื่อยๆ ส่วนยาทา retinoids, benzoyl peroxide
(BP) และ salicylic acid สามารถลดจำานวนรอยโรคที่อักเสบ รวม ยารักษาสิว
ถึงลดสิวอุดตันทั้งชนิดสิวอุดตันหัวดำาและหัวขาว ผู้ป่วยที่เป็นโรคสิว
ชนิดรุนแรง (ดังผู้ป่วยในรูปที่ 1) ควรได้รับการรักษาด้วยยาที่มีฤทธิ์ ยารักษาสิวมีหลายกลุ่มดังแสดงในตารางที่ 1 โดยตารางนี้
ทัง้ ต้านการอักเสบและฆ่าเชือ้ แบคทีเรียร่วมกัน ร่วมกับยาทีอ่ อกฤทธิ์ จะอธิบายถึงสาเหตุที่บางครั้งจำาเป็นต้องใช้ยาบางกลุ่มร่วมกัน เช่น
สลายคอมมีโดน การใช้ ย าทากลุ่ ม เรติ น อยด์ ร่ ว มกั บ ยาปฏิ ชี ว นะชนิ ด ทาหรื อ ชนิ ด
สำาหรับสิวอักเสบทีใ่ บหน้าทีเ่ ป็นน้อยจนถึงปานกลาง พบว่าการ รับประทานในช่วง 6-12 สัปดาห์แรกของการรักษาช่วยคุมอาการ
ใช้ยาทาเพียงอย่างเดียวอาจมีประสิทธิภาพใกล้เคียงกับการให้ยา ของสิวได้เร็วกว่าการใช้ยาทาเรตินอยด์เพียงอย่างเดียว เมือ่ พ้น 6-12
ปฏิชวี นะชนิดรับประทาน แต่ในกรณีเป็นสิวรุนแรงและเป็นชนิดแพร่ สัปดาห์แรกแล้วจึงอาจใช้แค่ยาทาเรตินอยด์เท่านั้น สำาหรับการใช้
กระจาย อาจใช้ยาทาร่วมกับยาตัวอืน่ หรือร่วมกับยารับประทานเพือ่ ยารักษาสิวร่วมกันนัน้ ให้ดรู ายละเอียดเพิม่ เติมได้ในกรอบ Combi-
ควบคุมอาการของสิวให้เร็วขึ้น nation therapies for acne
* º·¤ÇÒÁ¹Õàé »š¹µÍ¹·Õè 2 ¢Í§º·¤ÇÒÁàÃ×Íè § “àǪ»¯ÔºµÑ ãÔ ¹¡ÒÃÃÑ¡ÉÒâäÊÔÇ” ·Õµè ¾Õ ÁÔ ¾ã¹ÇÒÃÊÒà Medical Progress ©ºÑºàÁÉÒ¹ ¾.È.2552 (Medical Progress CME,
Vol.8 No.4) «Öè§ã¹µÍ¹·Õè 1 ¢Í§º·¤ÇÒÁ¡Å‹ÒǶ֧¡ÒÃÇÔ¹Ô¨©Ñ ¡ÒûÃÐàÁÔ¹¤ÇÒÁÃعáç áÅСÒôÙáżÔÇ˹ѧ
Medical Progress CME / November 2010 41
Continuing Medical Education
ยาทารักษาสิว การทายารักษาสิว
ยาทารักษาสิวส่วนใหญ่มีลักษณะเป็นเจลหรือครีมที่ทาทิ้งไว้ โดยทั่วไปแพทย์ควรแนะนำาผู้ป่วยว่า หลังทำาความสะอาด
(leave-on) รายละเอียดของกลุม่ ยาทารักษาสิวชนิดทีเ่ ป็นน้อยจนถึง ใบหน้าและซับหน้าให้แห้งแล้วควรรอประมาณ 10-15 นาทีจงึ ทายา
ปานกลางแสดงในตารางที่ 2 รักษาสิว เพราะการทายารักษาสิวขณะที่ผิวหนังยังเปียกชื้นอยู่อาจ
µารา§ทÕè 1. Therapeutic groups of acne treatments*
Group Examples Beneficial actions Comedonal Inflammatory Onset and time
acne acne to maximum
clinical benefits
Cleansers Surfactants (eg, sodium Remove oils (solubilize 3 3 1 to 2 weeks
lauryl sulfate) sebum), debris, bacteria
Antibacterials and Reduce bacterial numbers 3 3 1 to 6 weeks
antiseptics
Salicylic acid Solubilizes sebum +/- +/- Days to weeks
Comedolytic
Antibiotics Benzoyl peroxide Comedolytic and prevents 3 3 Hours to days to
and comedone formation 6 weeks
antibacterials Anti-inflammatory
Salicylic acid microgel Solubilizes sebum 3 3 3 Hours to days to
complex Comedolytic and prevents 6 weeks
comedone formation
Antimicrobial
Anti-inflammatory
Topical: clindamycin, Anti-inflammatory 3 3 3 1 to 6 weeks
erythromycin Antimicrobial
Systemic: tetracyclines, Reduce comedone
macrolides, sulfonamides formation
Retinoids Topical: adapalene, Comedolytic and prevent 3 3 3 4 to 12 weeks
isotretinoin, tazarotene, comedone formation
tretinoin Anti-inflammatory
Even out pigment changes
and reduce scarring
Systemic: isotretinoin As for topical retinoids, and 3 3 3 3 3 4 to 16 weeks
markedly reduces sebum
production and, indirectly,
Propionibacterium acnes
Can induce prolonged
remissions
Hormones Some combined oral Reduce and alter sebum 3 3 3 3 12 to 36 weeks
contraceptives production, reduce keratin
Spironolactone plug formation and, 3 3 8 to 12 weeks
indirectly,
P acnes numbers
*Over-the-counter anti-acne products contain a range of ‘active’ ingredients not mentioned in this table. Peer-reviewed literature supporting the efficacy of these ingredients is generally lacking, and
their discussion is beyond the scope of this article.
42 Medical Progress CME / November 2010
ทำาให้ผิวระคายเคืองง่ายขึ้น ควรทาครีม เจล หรือโลชันรักษาสิว
ทัว่ ทัง้ บริเวณทีเ่ ป็น เพราะยาทาเหล่านีน้ อกจากจะรักษาสิวอักเสบที่ µารา§ทÕè 2. Topical medicated therapies for mild to
moderate facial acne
เป็นอยู่แล้ว ยังป้องกันไม่ให้เกิดสิวอักเสบขึ้นมาใหม่อีกด้วย
Minimal or mild acne
ระยะเวลาที่ใช้ในการรักษา การใช้ยาทาปฏิชีวนะ BP หรือ • Benzoyl peroxide 2.5 to 5% cream or gel nightly
ยาทาต่างชนิดร่วมกันมักทำาให้สวิ อักเสบทุเลาลงได้เร็ว (มักเริม่ เห็นผล • Salicylic acid microgel complex (gel or leave-on wipes) twice daily
ในเวลาเป็นชั่วโมงหรือวัน) การรักษาในกรณีของสิวที่เป็นน้อยจนถึง • Azelaic acid-not routinely used
ปานกลางใช้เวลานาน 6-12 สัปดาห์ ขึ้นอยู่กับการตอบสนองและ Mild to moderate acne or inadequate response to above after 6
weeks
ความทนทานต่อการใช้ยา (ตารางที่ 2) ในกรณีทมี่ กี ารอักเสบไม่บอ่ ย • Retinoid cream or gel second-nightly for three weeks then nightly:
นักอาจให้การรักษาแบบเป็นช่วงๆ แต่ถ้ามีการอักเสบบ่อยอาจให้ - Adapalene 0.1% cream or gel
การรักษาต่อเนือ่ งเป็นระยะเวลายาวด้วยยาทา BP หรือเรตินอยด์ ใน - Isotretinoin 0.05% gel
การรักษาสิวนั้นถ้าเป็นยาทา BP หรือยาปฏิชีวนะต้องใช้ต่อเนื่องกัน - Tazarotene 0.05% (increasing to 0.1% if inadequate) cream
- Tretinoin 0.05% (increasing to 0.1% if still inadequate) cream
อย่างน้อย 6 สัปดาห์ และถ้าเป็นยาทาเรตินอยด์ควรใช้ต่อเนื่องกัน or gel
นาน 3 เดือน จึงประเมินผลว่าการรักษาได้ผลหรือไม่ - Benzoyl peroxide 5% plus clindamycin 1% combination gel
nightly*
- Benzoyl peroxide 4 or 5% cream or gel nightly in combination
การป้องกันปัญหาจากการรักษาสิว with an antibiotic, either erythromycin 2% gel or clindamycin 1%
lotion, each morning*
พบว่ายาทา BP และ salicylic acid มักก่อให้ผวิ เกิดระคายเคือง - Benzoyl peroxide 4 or 5% cream or gel twice daily (for patients
(แดง แห้ง และ/หรือลอก) ทั้งยาทา BP และเรตินอยด์ทำาให้ผิวไว with oily non-sensitive skin)
ต่อแสงมากขึ้น (รูปที่ 2) สำาหรับรายละเอียดเพิ่มเติมของการใช้ BP Rapid control of inflammatory acne
Consider an initial combination with a topical antibiotic:
และ salicylic acid
รูปทÕè 2. Skin irritation, cheilitis • Retinoid nightly, and erythromycin 2% gel or clindamycin 1% lotion
and desquamation in a patient
ในการรักษาสิวตาม each morning or twice daily*
taking systemic isotretinoin กรอบ Benzoyl • Benzoyl peroxide 5% plus clindamycin 1% combination gel nightly*
• Benzoyl peroxide 4 or 5% nightly, and erythromycin 2% gel or
peroxide vs sali- clindamycin 1% lotion each morning or twice daily*
cylic acid micro- • Salicylic acid microgel complex twice daily, and erythromycin 2%
gel or clindamycin 1% lotion each morning or twice daily*
gel complex as
*Once good control has been achieved (usually after 6 to 12 or more weeks of treatment),
acne treatments consider stopping the antibiotic and relying on retinoid or benzoyl peroxide monotherapy
for maintaining control. Subsequent flares can then be managed by reinitiating the same
ควรแนะนำ า antibiotic combination (again usually for 6 to 12 weeks) until good control is re-established.
Topical antibiotics can be used once or twice daily in combination with benzoyl peroxide
and retinoids. The combination product Duac is more effective and better tolerated than its
ให้ผู้ป่วยทายา BP separate products.
และเรตินอยด์ก่อน
นอนเพื่ อ ลดการ ระคายเคืองในช่วง 3-4 สัปดาห์แรกของการทายาอาจทายาคืน
ระคายเคือง โดย เว้นคืน ต่อมาจึงเพิ่มเป็นทาทุกคืน ถ้าเริ่มมีการระคายเคืองอาจลด
This reaction occurs in 15 to 20% of patients ทายาบางๆ และ การทายากลับมาเป็นคืนเว้นคืนตามเดิม แม้วา่ อาจทา BP ได้วนั ละ 2
prescribed topical retinoids and/or benzoyl
peroxide but can be minimized or prevented หลีกเลีย่ งการทาใน ครัง้ แต่พบบ่อยว่าการทา BP เกินวันละครัง้ มักทำาให้ผวิ ระคายเคือง
by introducing these therapies gradually,
together with gentle skin care measures บริเวณรอบดวงตา นอกจากนัน้ ตัวยา BP จะฟอกสีผม เสือ้ ผ้า ผ้าเช็ดตัว และผ้าปูทนี่ อน
and/or a topical or systemic antibiotic. Sun ร่องจมูก และรอบ จึงควรทายาอย่างน้อย 30 นาทีกอ่ นเข้านอน (แต่ในประเทศไทยและ
protection and avoidance measures are also
important as these therapies increase skin ริมฝีปาก ในผู้ที่มี ประเทศสหรัฐอเมริกา แพทย์ผิวหนังนิยมให้ทายา BP ทิ้งไว้นาน
sensitivity to sunlight.
ประวัตผิ วิ ไวต่อการ 5-10 นาทีก่อนล้างหน้าตอนเช้าและเย็น หรือตอนเย็นอย่างเดียว
Medical Progress CME / November 2010 43
Continuing Medical Education
การใช้ยารับประทานรักษาสิว
µารา§ทÕè 3. Systemic antibiotic acne therapies
Moderate facial acne failing topical therapy and/or widespread ยารับประทานที่ใช้รักษาสิว ได้แก่ ยาปฏิชีวนะ เรตินอยด์
mild to moderate acne
• First-line therapy: doxycycline 50 to 100 mg nightly ยาคุมกำาเนิดชนิด combined oral contraceptives (COCs),
If above not tolerated or contraindicated consider: spinorolactone และ metformin สำาหรับการรักษาสิวชนิดที่เป็น
• Second-line therapy: erythromycin 250 mg twice daily or รุนแรงและแพร่กระจายอาจใช้ยารับประทานร่วมกับยาทา
roxithromycin 150 mg nightly
• Third-line therapy: minocycline 50 to 100 mg nightly การให้ ย าปฏิ ชี ว นะชนิ ด รั บ ประทานอาจจั ด เป็ น การรั ก ษา
Moderate to severe facial acne and/or widespread acne failing to อันดับแรก (first-line) ในผู้ป่วยเพศชายที่มักชอบรับประทานยา
respond sufficiently to a 6-week trial of above
มากกว่าการทายา ส่วนในเพศหญิงต้องระวังยารักษาสิวที่มีผลต่อ
• First-line therapy: doxycycline 150 to 200 mg daily (in larger
males) ทารกในครรภ์ เช่น ยารับประทาน tetracyclines และเรตินอยด์
If above not tolerated or contraindicated consider: นอกจากนัน้ การใช้ยาปฏิชวี นะชนิดรับประทานในผูป้ ว่ ยเพศหญิงอาจ
• Second-line therapy: erythromycin 500 mg twice daily or
roxithromycin 300 mg nightly ทำาให้เกิดโรคเชื้อยีสต์ในช่องคลอด (vaginal candidiasis)
• Third-line therapy: minocycline 100 mg nightly or trimethoprim
160 mg plus sulfamethoxazole 800 mg twice daily
Significant facial acne and/or insufficient facial response to above ยารับประทานปฏิชีวนะรักษาสิว
Combine systemic antibiotic and a topical therapy: ในประเทศออสเตรเลียแพทย์นิยมสั่งจ่ายยาปฏิชีวนะชนิด
• Retinoid: adapalene 0.1% cream or gel, isotretinoin 0.05% gel, รับประทานเพือ่ รักษาสิวเป็นคอร์ส 6 สัปดาห์, 3 เดือน หรือ 6 เดือน
tazarotene 0.1% cream, tretinoin 0.05% or 0.1% cream or gel
nightly* และอาจให้ ผู้ ป่ ว ยมารั บ ยาเดิ ม ได้ ในกรณี ที่ ใ ห้ ย าปฏิ ชี ว นะชนิ ด
• Benzoyl peroxide 4 to 5% cream or gel nightly* รับประทานเพียงตัวเดียวแล้วพบว่าการตอบสนองของสิวไม่ดพี อ อาจ
• Salicylic acid microgel complex twice daily*
ให้ยาเดิมในขนาดยาที่สูงขึ้น หรืออาจเลือกใช้ยาปฏิชีวนะตัวใหม่
*Once good control has been achieved (after usually 6 to 12 or more weeks of treatment),
consider stopping the antibiotic and relying on retinoid or benzoyl peroxide monotherapy ตารางที่ 3 แสดงรายการยาปฏิชีวนะชนิดรับประทานที่ใช้รักษา
for maintaining control. Subsequent flares can then be managed by reinitiating the same
antibiotic combination (again usually for 6 to 12 weeks) until good control is re-established.
Topical antibiotics can be used once or twice daily in combination with benzoyl peroxide
โรคสิว ในเพศหญิงอาจพิจารณาการรักษาด้วยฮอร์โมนร่วมด้วย ยา
and retinoids. The combination product stiefel is more effective and better tolerated than its
separate products. ปฏิชีวนะ (ทั้งชนิดทาและชนิดรับประทาน) มักออกฤทธิ์ร่วมกับการ
ใช้ยาทา BP และเรตินอยด์ทาำ ให้คมุ อาการสิวอักเสบทีใ่ บหน้าได้ดขี นึ้
และทาเรตินอยด์ก่อนนอน นอกจากนั้นการทา BP และเรตินอยด์ พบว่าเชื้อโรคที่ทำาให้เกิดสิวอักเสบคือ P. acnes ดื้อต่อยา
พร้อมกัน BP จะขัดขวางการออกฤทธิ์ของเรตินอยด์ - ผู้เรียบเรียง) erythromycin ชนิดรับประทานได้บอ่ ยกว่ายาปฏิชวี นะชนิดรับประทาน
ถ้าทายา BP หรือเรตินอยด์แล้วมีการระคายเคือง ควรแนะนำา ตัวอืน่ อย่างไรก็ตามการใช้ยา erythromycin ชนิดรับประทานยังนิยม
ให้ผู้ป่วยรออย่างน้อย 30 นาทีหลังล้างหน้าจึงเริ่มทายา อาจให้ ใช้ในหญิงมีครรภ์ที่มีสิวกำาเริบ และ/หรือในผู้ป่วยเพศหญิงที่เป็นสิว
ผู้ป่วยทายาในปริมาณที่น้อยลงหรือทายาวันเว้นวันจนกว่าอาการผิว ที่อาจตั้งครรภ์ระหว่างการรักษาได้
ระคายเคืองดีขึ้น อาจใช้ครีมให้ความชุ่มชื้นชนิดที่ไม่ก่อคอมมีโดน ในการรักษาด้วยยา doxycycline ชนิดรับประทานนัน้ อาจพบ
(non-comedogenic) ร่วมด้วย โดยทาทับยารักษาสิว การแพ้ยาชนิด fixed drug eruption ได้ โดยอาจเกิดขึน้ รวดเร็วมาก
ในเวลาไม่กชี่ วั่ โมงหลังรับประทานยา พบบ่อยทีส่ ดุ ทีใ่ บหน้า (รูปที่ 3)
การเปลี่ยนการรักษา หรือขาหนีบ ไม่ควรใช้ยา minocycline และ sulfonamide เป็นยา
ในกรณีที่ใช้ยาทารักษาสิวแล้วไม่ได้ผล ก่อนเปลี่ยนการรักษา รับประทานรักษาสิวอันดับแรก (first-line therapy) เพราะอาจ
ต้องพิจารณาโดยถี่ถ้วนก่อน เพราะการรักษาที่ไม่ได้ผลอาจเกิดจาก มีโอกาสเกิดการแพ้ยาอย่างรุนแรงได้บ่อย (รูปที่ 4) คือพบ drug
การที่ผู้ป่วยไม่ใช้ยาตามที่แพทย์สั่ง หรือเกิดจากผลแทรกซ้อนจาก hypersensitivity syndrome และในกรณีของยา sulfonamide ยัง
การใช้ยา เช่น การระคายเคือง ก่อให้เกิด Stevens-Johnson syndrome และ toxic epidermal
44 Medical Progress CME / November 2010
necrolysis ด้วย ทั้งนี้ยา minocycline ยังทำาให้เกิด delayed P. acnes จะดือ้ ยาปฏิชวี นะ ดังนัน้ ในการรักษาสิวทีต่ อ่ เนือ่ งกันนาน
reactions (ทีเ่ กิดหลังได้ยานานเป็นเดือนหรือเป็นปี) คือพบผิวเปลีย่ น แพทย์ควรพิจารณาเป็นระยะๆ ว่าเกิดการดื้อยาหรือไม่ พบว่ายา
สีเป็นสีเทา-น้ำาเงิน (blue-grey pigmentation) ตรงตำาแหน่งที่เป็น ทา BP ช่วยลดการดื้อยาปฏิชีวนะลงได้ ในผู้ป่วยที่ทนยา BP ได้จึง
สิวและรอยแผลเป็นสิว และอาจก่อให้เกิด drug-induced lupus อาจให้ยาปฏิชวี นะร่วมกับยาทา BP ในกรณีทผี่ ปู้ ว่ ยทนยา BP ไม่ได้
(ที่มีลักษณะคาบเกี่ยวกับ polyarteritis nodosa) นอกจากนั้นยา อาจให้ยาปฏิชีวนะร่วมกับยาทา salicylic acid
minocycline ยังอาจก่อให้เกิด benign intracranial hypertension นอกจากนั้นในกรณีของผู้ป่วยสิวที่ดื้อต่อยาปฏิชีวนะ หากเป็น
ดั ง นั้ น เ นื่ อ ง จ า ก สิวน้อยถึงปานกลางอาจให้การรักษาด้วยฮอร์โมนในเพศหญิง และ
รูปทÕè 3. A fixed drug eruption การใช้ ย า mino- ให้ยา isotretinoin ชนิดรับประทานในผูป้ ว่ ยเพศชายและหญิงที่เป็น
due to doxycycline therapy in a
17-year-old male cycline ยังมีความ สิวรุนแรงมาก และในเพศชายที่เป็นสิวรุนแรงน้อยจนถึงปานกลาง
เสี่ยงต่อการเกิดผล
แ ท ร ก ซ้ อ น สู ง จึ ง ยาเรµินอยดชนิดรับประทาน
ไม่ ค วรใช้ ย าตั ว นี้ ยา isotretinoin ชนิดรับประทานมีความเสี่ยงสูงมากเพราะ
ในขนาดที่ สู ง เกิ น ทำาให้ทารกในครรภ์พิการได้ ยาตัวนี้ต้องสั่งจ่ายโดยแพทย์ผิวหนัง
กำาหนด เท่านั้น ในเพศหญิงจึงอาจพิจารณาทางเลือกอื่นคือ การให้ยาคุม
กำาเนิด (COC pills) เพื่อรักษาสิว ยา isotretinoin มีประโยชน์
¡Òô×éÍÂÒ»¯ÔªÕǹРอย่างยิ่งในการรักษาสิวที่เป็นรุนแรงมาก และยังมีประโยชน์ในการ
The red, irritable, round or oval raised plaques เนื่องจากการ รักษาทีด่ อื้ ต่อการรักษาอืน่ รวมทัง้ ใช้ในการรักษาสิวทีอ่ าจก่อแผลเป็น
usually become evident and/or noticeably ใช้ยาปฏิชวี นะมีสว่ น ทั้งทางร่างกายและจิตใจ เมื่อใช้การรักษาอื่นแล้วไม่ได้ผล
worsen within hours of taking doxycycline. They
most commonly occur on the face or groin สำาคัญในการรักษา
area, and can occasionally develop a central
blister. The eruption settles within weeks of สิ ว เพราะออกฤทธิ์ Combined oral contraceptives
stopping therapy but can sometimes cause
hyperpigmentation that can take months to ทั้ ง ต้ า นการอั ก เสบ ยาคุมกำาเนิด combined oral contraceptives (COC pills)
fade. Fading of hyperpigmentation on the face และฆ่าเชือ้ แบคทีเรีย ทีน่ าำ มาใช้รกั ษาสิวมีสว่ นผสมของ cyproterone acetate, desoges-
can be quickened by acne treatments such as
topical tretinoin. จึ ง มี โ อกาสที่ เ ชื้ อ trel, dienogest, drospirenone, gestodene หรือ levonorgestrel
รูปทÕè 4a to c. Minocycline hypersensitivity syndrome in a 16-year-old male after 10 weeks of minocycline therapy
Features included a fever, sore throat, cervical lymphadenopathy, malaise, shortness of breath, a puffy swollen head and neck with erythema,
pustules and erosion on the face (a, left), a skin eruption including diffuse truncal erythema and scale (b, centre), along with prominent hand
and foot involvement with tender erythematous swelling that resolved with significant peeling and desquamation (c, right). There was associated
hepatitis and pneumonitis. Complete resolution of symptoms took 12 weeks.
Medical Progress CME / November 2010 45
Continuing Medical Education
ในกรณีของผู้ป่วยเพศหญิงที่เป็นสิวรุนแรงมาก พบว่าการให้
µารา§ทÕè 4. Combined oral contraceptive pills useful
in acne COC ทีม่ สี ว่ นผสมของ cyproterone (ทีเ่ ป็น anti-androgenic และ
เป็น COC รุ่นที่ 4) มีประโยชน์มาก รวมทั้งผู้ป่วยที่เป็น polycystic
Progestogen Estrogen COC generation
ovarian disease ร่วมด้วย แต่ยาตัวนีเ้ พิม่ อัตราเสีย่ งต่อการเกิดภาวะ
Cyproterone Ethinylestradiol 4th
acetate 2 mg* 35 µg หลอดเลือดดำาอุดตัน ดังนั้นในผู้ป่วยสิวที่เป็นไม่มากนักอาจให้ COC
Levonorgestrel 100 Ethinylestradiol 2nd รุ่นที่ 2 ที่มีทั้ง levonorgestrel และ estrogen ในปริมาณต่ำา ส่วน
µg* 20 µg COC รุน่ ที่ 3 และ spironolactone derivative COC เหมาะสำาหรับ
Dienogest 2 mg Ethinylestradiol 3rd ผู้ป่วยเพศหญิงที่ต้องการ estrogen ในขนาดสูง
30 µg
Drospirenone 3 mg Ethinylestradiol Spironolactone
30 µg analogue ยา spironolactone
Desogestrel 150 Ethinylestradiol 3rd ยา spironolactone เป็นสเตียรอยด์สังเคราะห์ที่มีฤทธิ์ขับ
µg 30 µg ปัสสาวะอย่างอ่อน มักใช้ร่วมกับ COC ในผู้ป่วยสิวที่มี seborrhea
Gestodene 75 µg Ethinylestradiol 3rd และ/หรือ hypertrichosis ขนาดที่ใช้ปกติคือ 50-100 มก./วัน
30 µg
*Reasonably good quality controlled trials have shown that cyproterone and low-dose
นาน 6-9 เดือน ควรเตือนผู้ป่วยให้ระวังการเกิดความดันโลหิตต่ำา
levonorgestrel-containing products have benefits in acne over comparator third-generation
COCs. The benefits are greatest for cyproterone. Placebo-controlled trials have shown ในคนที่มีน้ำาหนักน้อย อาจลดขนาดยาลงเหลือวันละ 25-50 มก.
benefits in acne for all third-generation progestogens and the ‘spironolactone analogue’
drospirenone. ตามความเหมาะสม
การรักษาโรคสิวด้วยฮอร์โมนนั้น แพทย์ควรศึกษาวิธีการใช้
ขนาดต่ำา (100 มคก.) ที่เป็น progestogen (ตารางที่ 4) โดยทั่วไป ยา ซักประวัติ และตรวจร่างกายโดยละเอียด รวมถึงควรปรึกษา
แล้วยาคุมกำาเนิดชนิดฝัง (implantable contraceptives) ทำาให้สิว สูตินรีแพทย์และอายุรแพทย์ตามความเหมาะสม
เลวลง
แพทย์อาจพิจารณาเลือกใช้การรักษาด้วยฮอร์โมนเพื่อคุมสิว ยา metformin และการลดน้ำาหนัก
ในระยะยาวในผู้ป่วยเพศหญิงที่เป็นสิวชนิดที่มักเป็นซ้ำาตั้งแต่น้อย มีการศึกษาพบว่าการรักษาสิวด้วยการลดน้ำาหนัก และ/หรือ
จนถึงมาก การรักษาด้วยฮอร์โมนมักได้ผลช้า พบบ่อยว่ามักเริ่มเห็น ให้ยา metformin เป็นเวลา 6 เดือนได้ผลคล้ายคลึงกับการรักษา
ผลเมื่อได้ยานานถึง 3 เดือนหรือมากกว่านั้น และมักได้ผลเต็มที่ใน ด้วย COC ที่มีส่วนผสมของ cyproterone โดยการศึกษานี้ให้ยา
ระยะ 6-9 เดือน metformin 500 มก.วันละ 2 ครั้งในช่วง 3 เดือนแรก ต่อมาเพิ่ม
การให้การรักษาด้วย COC ร่วมกับยาทารักษาสิวในช่วง 2-3 ขนาดยาเป็น 1,000 มก.วันละ 2 ครั้ง พบว่านอกจากอาการสิวดีขึ้น
เดือนแรกของการให้ COC จะช่วยให้การรักษาสิวทีใ่ บหน้าออกฤทธิ์ แล้ว ยา metformin และการลดน้ำาหนักยังช่วยลดภาวะ insulin
ได้เร็วขึ้น และมีผลควบคุมสิวในระยะยาวนานขึ้นกว่าการให้ COC resistance และลดโอกาสเสี่ยงของการเกิดโรคต่างๆ ที่สัมพันธ์กับ
แต่เพียงอย่างเดียว นอกจากนั้นการให้ COC ร่วมกับยาปฏิชีวนะ โรคอ้วน ทั้งนี้อาจใช้ยา merformin ร่วมกับยาทารักษาสิว และอาจ
ชนิดรับประทานในช่วง 3-6 เดือนแรกก็ช่วยควบคุมอาการกำาเริบ ใช้ร่วมกับยาปฏิชีวนะชนิดรับประทานรักษาสิวได้
ของสิวได้เร็วกว่า การให้ยาปฏิชีวนะชนิดรับประทานร่วมกับ COC
ไม่พบว่ามีผลต่อการคุมกำาเนิด อย่างไรก็ตามในฉลากยาของ COC การµั้§ครรภ์และโรคสิว
ได้ระบุวา่ การให้ COC ร่วมกับยาปฏิชวี นะชนิดรับประทานอาจทำาให้
ผลการคุมกำาเนิดของ COC ลดน้อยลง จึงควรแจ้งให้ผู้ป่วยทราบ ผู้ป่วยที่เป็นสิวและเป็น polycystic ovarian syndrome ที่
โอกาสเสี่ยงนี้ และผู้ป่วยอาจจำาเป็นต้องได้รับการคุมกำาเนิดวิธีที่ 2 ประสงค์จะตั้งครรภ์มักได้ประโยชน์เพิ่มเติมจากการรับประทานยา
ในช่วงที่ได้รับยาร่วมกันนี้ metformin เพราะยาตัวนี้ทำาให้สิวดีขึ้นและช่วยในแง่การเจริญพันธุ์
46 Medical Progress CME / November 2010
ในขณะที่ส่วนใหญ่แล้วการรักษาต่างๆ ที่ต้องการช่วยให้ตั้งครรภ์ซึ่ง เป็นที่น่าวิตกว่ายานี้สามารถหาซื้อได้ทั่วไปโดยไม่ผ่านแพทย์
รวมทั้ง in vitro fertilization มักทำ�ให้สิวเลวลงชั่วคราว ในกรณีทผี่ หู้ ญิงทีร่ บั ประทานยา spironolactone แล้วตัง้ ครรภ์
ผู้ป่วยสิวที่สัมพันธ์กับฮอร์โมน (hormonal acne) มักมีสิว ต้องหยุดยาทันที ถ้ารับประทานยาตัวนี้ในช่วง 2-3 เดือนแรกของ
กำ�เริบช่วงไตรมาสแรกของการตั้งครรภ์ แต่หลังจากนั้นสิวมักดีขึ้น อายุครรภ์ ยาตัวนี้ไม่น่ามีผลเสียใดๆ แต่ถ้าได้รับยาตัวนี้ในช่วง 2-3
อย่างรวดเร็วและมักหายไปในไตรมาสสุดท้าย พบว่าการให้นมบุตร เดือนสุดท้ายของการตั้งครรภ์จะมีผลต่อพัฒนาการของทารกใน
มักทำ�ให้สิวกลับมาเป็นซ้ำ�ช้าลง ผู้ป่วยเพศหญิงหลายรายที่เป็น ครรภ์เพศชายทำ�ให้มีลักษณะเพศหญิง (feminization) ส่วนยากลุ่ม
สิวเรื้อรังสังเกตว่าสิวมักเป็นน้อยลงหรือหายไปในการตั้งครรภ์ครั้ง tetracyclines มีผลต่อกระดูกและฟันของทารกในครรภ์ จึงห้าม
ต่อๆ ไป ไม่ให้หญิงมีครรภ์รับประทาน และไม่ให้ใช้ในเด็กอายุต่ำ�กว่า 8 ปี
ยารักษาสิวที่จัดว่าปลอดภัยในกรณีที่ตั้งครรภ์ ได้แก่ (บางตำ�ราระบุว่าห้ามใช้ในเด็กอายุต�่ำ กว่า 13 ปี หรือจนกว่าจะมี
- Benzoyl peroxide ฟันแท้ขึ้นครบ)
- Erythromycin (ทั้งรูปแบบยาทาและยารับประทาน)
- Clindamycin การรักษาสิวในอนาคต
- Azelaic acid
ยารักษาสิวที่ห้ามไม่ให้ใช้ในสตรีที่มีโอกาสตั้งครรภ์ ได้แก่ ปั จ จุ บั น มี ก ารศึ ก ษาและวิ จั ย เรื่ อ งการใช้ เ ลเซอร์ แ ละการ
- ยา isotretinoin ชนิดรับประทาน ฉายแสงรักษาสิวกันมาก แต่ก็ยังไม่ใช่วิธีหลักทั่วไปที่ใช้รักษาสิวกัน
- Tetracyclines (doxycycline และ minocycline) ในขณะนี้ เพราะมักมีค่าใช้จ่ายสูงมาก และข้อมูลบางด้านอาจยังไม่
- Spironolactone เพียงพอ การฉายแสงและใช้เลเซอร์รักษาสิวที่มีการศึกษาและเริ่ม
- ยาทาเรตินอยด์ทั้งรูปแบบครีมและเจล ใช้รักษาสิวในขณะนี้ เช่น
ยา isotretinoin ชนิดรับประทานเป็นยารักษาสิวที่มีผลทารก การฉายแสงสีน้ำ�เงิน (blue light therapy) แสงช่วงคลื่น
วิรปู ทีพ่ สิ จู น์แล้วว่าทำ�ให้เสีย่ งต่อการเกิดทารกพิการ ในกรณีทผี่ ปู้ ว่ ย เฉพาะนี้ฆ่าเชื้อแบคทีเรียที่ก่อให้เกิดสิว เนื่องจากแสงสีน้ำ�เงินที่
รับประทานยาตัวนี้แล้วสงสัยว่าตั้งครรภ์ต้องหยุดยาทันที และควร ฉายออกมาไม่มีส่วนผสมของรังสียูวีจึงไม่ทำ�ให้ผิวหนังได้รับอันตราย
ทดสอบการตั้งครรภ์ หากตั้งครรภ์จริงต้องแจ้งตจแพทย์ผู้สั่งจ่ายยา การรักษาด้วยวิธีนี้เหมาะกับผู้ที่เป็นสิวอักเสบธรรมดา แต่ถ้าเป็นสิว
เพือ่ การปรึกษาและส่งต่อสูตนิ รีแพทย์เพือ่ พิจารณาการทำ�แท้ง ดังนัน้ อักเสบมากชนิดเป็นถุงซิสต์ที่เรียกว่าสิวหัวช้างก็ใช้ไม่ได้ผล
จึงห้ามไม่ให้ใช้ยา isotretinoin ในผู้หญิงที่คิดจะตั้งครรภ์หรือกำ�ลัง การฉายพลังงานแสงและความร้อน (light and heat energy)
ตั้งครรภ์อยู่ โดยต้องหยุดยาครบ 1 เดือนจึงตั้งครรภ์ได้โดยปลอดภัย เชื่อว่าการใช้พลังงานแสงและความร้อนจะฆ่าเชื้อแบคทีเรียและลด
ต้องไม่ให้ยานี้ขณะให้นมบุตร ต้องไม่บริจาคโลหิตระหว่างรับยา ไม่ การทำ�งานของต่อมไขมัน โดยทำ�ให้ต่อมไขมันหดตัวลง
นำ�ยาไปแจกจ่ายผู้อื่น และต้องใช้ยาภายใต้การดูแลของแพทย์โดย Photodynamic therapy เช่น การทา aminolevulinic acid
เคร่งครัดเท่านั้น (ในสหรัฐอเมริกาสตรีวัยเจริญพันธุ์ต้องคุมกำ�เนิด (ALA) ร่วมกับการฉายแสง มีการใช้สารละลาย ALA (5-aminole-
ก่อนรับยา 1 เดือน และต้องทำ�ตรวจการตัง้ ครรภ์ 2 ครัง้ จึงเริม่ ให้ยา vulinic acid) ทาผิวหนัง สารละลายตัวนี้ท�ำ ให้ผิวไวต่อแสงมากขึ้น
ได้ และต้องทำ�ตรวจครรภ์ซ้ำ�ทุกเดือนระหว่างรับยา - ผู้เรียบเรียง) หลังจากทายา 15-60 นาที (ระยะเวลาขึ้นกับความรุนแรงของสิว)
ผูต้ งั้ ครรภ์ทไี่ ด้รบั ยา isotretinoin มีโอกาสเกิดทารกวิรปู สูงถึงร้อยละ จะเช็ดยาออกและฉายแสง
25-30 ความผิดปกติของทารกที่พบบ่อยคือ ที่กะโหลกและใบหน้า การใช้เทคนิค ELOS คือใช้พลังงานแสง (intense pulse
หัวใจ ระบบประสาทส่วนกลาง และต่อมไทมัส แม้ว่าจะมีการเตือน light; IPL) ร่วมกับคลืน่ วิทยุ (radiofrequency; RF) รักษาสิวอักเสบ
ถึงอันตรายข้อนีอ้ ยูเ่ สมอก็ยงั พบว่ายังมีการตัง้ ครรภ์เกิดขึน้ 3.4 ครัง้ / โดยที่คลื่นแสงฆ่าเชื้อแบคทีเรียที่เป็นต้นเหตุของสิว และคลื่นแสง
1,000 คอร์สของการรักษาด้วยยา isotretinoin ยาตัวนี้ต้องสั่งจ่าย ร่วมกับคลื่นวิทยุยังลดการทำ�งานของต่อมไขมัน ทำ�ให้ผลิตไขมันซึ่ง
โดยตจแพทย์ และควรให้ผปู้ ว่ ยเซ็นรับทราบ แต่ส�ำ หรับประเทศไทย เป็นต้นเหตุของสิวน้อยลง รวมทั้งยังช่วยให้การสมานผิวเกิดเร็วขึ้น
Medical Progress CME / November 2010 47
Continuing Medical Education
Combination therapies for acne Benzoyl peroxide vs salicylic acid microgel complex
Topical acne treatments alone can be surprisingly effective for as acne treatments
controlling localized facial acne. However, combination therapy Before a recent series of industry-sponsored trials comparing
(a topical therapy with another topical therapy, or a topical benzoyl peroxide and salicylic acid microgel complex, acne
therapy with a systemic therapy) is a consideration in certain treatment studies classically only reassessed acne severity after
patients. These patients are those who have more severe, deep, a week of therapy. This recent series is one of the first to
widespread and inflammatory acne and those who fail to respond answer a very important question for patients: how quickly do
to or tolerate topical therapy. The combinations increase the the different acne treatments result in visible improvements in
treatment benefits and also help reduce the side effects of each inflammatory acne lesions?6,7
agent.
Examples of combination therapies Both benzoyl peroxide and salicylic acid microgel complex
work quickly. When used twice a day, they resulted in over
• For rapid control of an inflammatory acne facial flare, consider 50% of subjects reporting an improvement in their inflammatory
combination therapy of a topical or systemic antibiotic with acne lesions within 8 hours of starting treatment. By 8 hours,
topical benzoyl peroxide, retinoid and/or salicylic microgel clinically significant improvement was observed in over 75% of
complex. treated lesions (clinician assessed). Improvement over placebo
• Benzoyl peroxide has been shown to increase the continued to the seventh day, and regular use maintained this
effectiveness of erythromycin and clindamycin and can even5 reduction in inflammatory papules and pustules. The salicylic
restore the antibiotic sensitivity of the bacterium concerned. acid microgel complex was slightly better in improving the
Separate benzoyl peroxide and antibiotic creams or gels less inflammatory acne6,7lesions, including open comedones and
or the combination product of benzoyl peroxide 5% plus dilated plugged pores.
clindamycin 1% can be used. The simplicity of use and the Skin irritation
better tolerability of the combination product, which has been
formulated to protect against benzoyl peroxide irritation in all These sponsored trials also emphasised the importance of
but the most sensitive skin, have been associated with greater implementing strategies that help avoid skin irritation side
adherence, higher patient preference and successful nightly effects when starting topical benzoyl peroxide therapy. Many
application in most patients.4 patients interpret skin irritation due to a topical treatment
as failure of the treatment to improve their acne and/or the
• Several trials support the practice of combining a topical treatment making their acne worse.
retinoid (particularly adapalene and tazarotene) with a topical
antibiotic when initiating treatment for inflammatory facial acne.
This combination produces clinically significant benefits over
either product alone, including faster onset of benefits, a
greater reduction in acne lesion count and a lower incidence Summary
of irritation. The lower irritancy of the combination allows most
patients to tolerate nightly retinoid use from day one.4 • Acne may be treated using either topical or systemic
therapies, or combinations of these.
• For mild to moderate acne, many topical treatments are at
การใช้ไดโอดเลเซอร์ (diode laser) มีการศึกษาการใช้ least as effective as monotherapy with oral antibiotics.
1450-nm diode laser ในการรักษาสิว • For more severe or widespread acne, using a topical therapy
การใช้เพาส์ดายเลเซอร์ (pulsed dye laser) with another topical therapy or a systemic therapy achieves
more rapid and greater control.
อย่างไรก็ตามการใช้การฉายแสงและเลเซอร์รักษาสิวนั้นยัง • Agents with proven efficacy as topical acne therapies include
ไม่จัดว่าเป็นการรักษาสิวในลำาดับแรก เพราะยังมีค่าใช้จ่ายสูง ผล benzoyl peroxide, salicylic acid microgel complex, topical
antibiotics and topical retinoids.
การศึกษายังไม่มากพอว่าได้ผลดีแค่ไหน และผลการรักษาอยู่ได้ • Agents with proven efficacy as systemic acne therapies
นานแค่ไหน include systemic antibiotics and retinoids, certain combined
oral contraceptives, spironolactone and metformin.
• Retinoids, tetracyclines and spironolactone are not safe to
สรุป use during pregnancy.
• Poor adherence is a common reason for ‘treatment failure’,
and is often due to side effects (such as irritation), incorrect
ผู้สนใจในแนวทางการรักษาสิวอาจหาข้อมูลเพิ่มเติมได้จาก product use and/or inconvenient regimens.
www.allaboutacne.com.au
A list of references can be obtained upon request to the editor.
48 Medical Progress CME / November 2010
The Quiz
รหัสกิจกรรม 3-3220-000-9304/101102
คÓ¶าÁสÓËรับบทควาÁ เวชปฏิบัµิในการรักษาโรคสิว: การรักษา
นพ.ประวิตร พิศาลบุตร (พ.บ. (เกียรตินิยมอันดับหนึ่ง),
Diplomate, American Board of Dermatology & American Subspecialty Board of Dermatological Immunology)
1. ยา salicylic acid microgel complex ออกฤทธิ์ในการรักษาสิวอย่างไร 6. จากบทความฉบับนี้ หากผู้ป่วยเป็นสิวที่ใบหน้าแบบปานกลางจนถึงรุนแรง
ก. ละลายไขมัน sebum และ/หรือสิวทีเ่ ป็นแพร่กระจายทีไ่ ด้ยา minocycline 50-100 มก. ทุกคืนมา
ข. สลายก้อนไขมันอุดตัน (comedolytic) นาน 6 สัปดาห์ โดยรับประทานยาครบถ้วนแล้วยังไม่ตอบสนองต่อการรักษา
ค. ป้องกันการเกิดก้อนไขมันอุดตัน ยารับประทานที่จัดว่าเป็น first-line therapy ในกรณีนี้ได้แก่ข้อใด
ง. ลดการอักเสบ ก. Doxycycline 50-100 มก. ทุกคืน
จ. ถูกทุกข้อ ข. Roxithromycin 300 มก. ทุกคืน
ค. Erythromycin 500 มก. วันละ 2 ครั้ง
2. ยาทารักษาสิวที่จัดอยู่ในกลุ่มเรตินอยด์ได้แก่ข้อใด ง. Doxycycline 150-200 มก. ต่อวัน (ในเพศชายที่ตัวโต)
ก. Macrolides จ. ถูกทุกข้อ
ข. Adapalene
ค. Benzoyl peroxide 7. จากบทความฉบับนี้ หากผู้ป่วยเป็นสิวที่ใบหน้าที่แบบปานกลางจนถึงรุนแรง
ง. Salicylic acid microgel complex และ/หรือสิวทีเ่ ป็นแพร่กระจายทีไ่ ด้ยา minocycline 50-100 มก. ทุกคืนมา
จ. ถูกทุกข้อ นาน 6 สัปดาห์ โดยรับประทานยาครบถ้วนแล้วยังไม่ตอบสนองต่อการรักษา
ยารับประทานที่จัดว่าเป็น second-line therapy ในกรณีนี้ได้แก่ข้อใด
3. ยาทารักษาสิวที่ใช้ในกรณีสิวที่เป็นน้อยมากหรือเป็นน้อย (minimal or mild ก. Doxycycline 50-100 มก. ทุกคืน
acne) ได้แก่ข้อใด ข. Roxithromycin 300 มก. ทุกคืน
ก. Benzoyl peroxide 2.5-5% cream ค. Erythromycin 250 มก. วันละ 2 ครั้ง
ข. Adapalene 0.1% cream ง. Doxycycline 150-200 มก. ต่อวัน
ค. Tazarotene 0.05% cream จ. ถูกทุกข้อ
ง. Retinoids ทุกคืน และ clindamycin 1% lotion วันละ 2 ครั้ง
จ. ถูกทุกข้อ 8. ยารักษาสิวที่ปลอดภัยต่อการตั้งครรภ์ได้แก่ยาใด
ก. Adapalene
4. จากบทความฉบับนี้ ยาทารักษาสิวที่ใช้ในกรณีสิวที่เป็นน้อยจนถึงปานกลาง ข. Benzoyl peroxide
(mild to moderate acne) หรือสิวที่ตอบสนองไม่เพียงพอต่อการทายา ค. Tazarotene
benzoyl peroxide 5% cream ทุกคืนมานาน 6 สัปดาห์ได้แก่ข้อใด ง. Minocycline
ก. Adapalene 0.1% cream จ. ถูกทุกข้อ
ข. Tazarotene 0.05% cream
ค. Isotretinoin 0.05% gel 9. ยารักษาสิวที่ห้ามใช้ในสตรีที่มีโอกาสตั้งครรภ์ได้แก่ยาใด
ง. Benzoyl peroxide 5% plus clindamycin 1% combination gel ก. Doxycycline
จ. ถูกทุกข้อ ข. Spironolactone
ค. Retinoid creams
5. จากบทความฉบับนี้ ยาชนิดรับประทานที่จัดว่าเป็น first-line therapy ง. Retinoid gels
สำาหรับรักษาสิวทีใ่ บหน้าทีเ่ ป็นปานกลางและไม่ตอบสนองต่อยาทา และ/หรือ จ. ถูกทุกข้อ
สิวที่เป็นน้อยจนถึงปานกลางชนิดที่เป็นแพร่กระจาย ได้แก่ข้อใด
ก. Doxycycline 50-100 มก. ทุกคืน 10. ยาชนิดรับประทานที่มีการทดลองนำามารักษาสิวที่มีลักษณะเป็น “anti-
ข. Erythromycin 250 มก. วันละ 2 ครั้ง diabetic drug in the biguanide class” ได้แก่ยาใด
ค. Roxithromycin 150 มก. ทุกคืน ก. Isotretinoin
ง. Minocycline 50-100 มก. ทุกคืน ข. Spironolactone
จ. ถูกทุกข้อ ค. Cyproterone
ง. Metformin
จ. ถูกทุกข้อ
กรุณาตอบในชุดกระดาษคÓตอบ หมดเขตรับคÓตอบ 28 กุมภาพันธ์ 2554 เฉลยคÓตอบในเล่ม Medical Progress CME Vol.10 No.3
Medical Progress CME / November 2010 49
You might also like
- ยาต้านจุลชีพDocument28 pagesยาต้านจุลชีพHongyuu Lee100% (1)
- เภสัชวิทยาDocument15 pagesเภสัชวิทยาBam SarinratNo ratings yet
- ข้อสอบMCQ เรื่อง endocrineDocument58 pagesข้อสอบMCQ เรื่อง endocrinetotoil22100% (2)
- ประเมินแพ้ยาDocument34 pagesประเมินแพ้ยาTheepop Lerdkarn100% (1)
- ราคากลางของยาตามบัญชียาหลักแห่งชาติ2553 excelDocument38 pagesราคากลางของยาตามบัญชียาหลักแห่งชาติ2553 excelvivianNo ratings yet
- รวมเล่ม ชีทจิตเวช รามาธิบดี (Fixed Bookmark)Document155 pagesรวมเล่ม ชีทจิตเวช รามาธิบดี (Fixed Bookmark)NATTAPAT SANGKAKUL100% (1)
- ทบทวนยาปฏิชีวนะDocument23 pagesทบทวนยาปฏิชีวนะณกรณ์ อยู่นิ่ม100% (1)
- ADR Skin - คู่มือติดตามอาการไม่พึงประสงค์ที่เกิดขึ้นจากผิวหนังDocument73 pagesADR Skin - คู่มือติดตามอาการไม่พึงประสงค์ที่เกิดขึ้นจากผิวหนังSupalerk Kowinthanaphat100% (1)
- File 3068.file 122Document55 pagesFile 3068.file 122Mr. YellNo ratings yet
- CAP PneumoniaDocument10 pagesCAP Pneumoniaบอส เลิศเกียรติรัชตะNo ratings yet
- คู่มือการใช้ยา21043Document135 pagesคู่มือการใช้ยา21043vivian100% (5)
- Daily Log 1 5Document18 pagesDaily Log 1 5Manuschanok SutthipongNo ratings yet
- MCQ รอบ 1 Rx19Document44 pagesMCQ รอบ 1 Rx19เด็กชายท็อปปิ้ง ชอบกลิ้งเข้าคณะเภสัชศาสตร์No ratings yet
- Cross AllergyDocument64 pagesCross AllergySitthipon TrikanchanawatthanaNo ratings yet
- Checklist stock ยา ER ใหม่Document1,079 pagesChecklist stock ยา ER ใหม่Pucca' JernyNo ratings yet
- Sodium Bicarbonate 3. Calcium CarbonateDocument27 pagesSodium Bicarbonate 3. Calcium CarbonatethanapongNo ratings yet
- Uncommon DiseasejDocument102 pagesUncommon DiseasejArluk WanthaphisutNo ratings yet
- Had 3Document7 pagesHad 3Praphatsorn ChaphakdeeNo ratings yet
- คู่มือทักษะตามเกณฑ์ความรู้ความสามารถทางวิชาชีพDocument55 pagesคู่มือทักษะตามเกณฑ์ความรู้ความสามารถทางวิชาชีพชนิชา ธาดาวรภัทร์83% (6)
- แยกโรค MCQ รวมปี (คล้ายอุบล)Document335 pagesแยกโรค MCQ รวมปี (คล้ายอุบล)thanapongNo ratings yet
- DoseDocument2 pagesDoseVajirawit PetchsriNo ratings yet
- Tinea CapitisDocument15 pagesTinea CapitisNanthicha MkplNo ratings yet
- 5การประเมินภาวะสุขภาพระบบผิวหนังDocument31 pages5การประเมินภาวะสุขภาพระบบผิวหนังDel Del100% (1)
- Guideline ASU Ramathibodi. Mar 2015 แนวทางปฏิบัติในการดูแลผู้ป่วยโรคติดเชื้อระบบทางเดินหายใจส่วนบนDocument9 pagesGuideline ASU Ramathibodi. Mar 2015 แนวทางปฏิบัติในการดูแลผู้ป่วยโรคติดเชื้อระบบทางเดินหายใจส่วนบนsms_msn_No ratings yet
- การรักษาสิวในร้านยาDocument5 pagesการรักษาสิวในร้านยาBeboh PhotowindyNo ratings yet
- Acne สมาคมโรคผิวหนังไทยDocument8 pagesAcne สมาคมโรคผิวหนังไทยUdsanee SukpimonphanNo ratings yet
- SOAP Vaginal CandidiasisDocument9 pagesSOAP Vaginal Candidiasisอรรณพ บุญยิ่งNo ratings yet
- Seb DermDocument5 pagesSeb DermNapassawan KhongpanNo ratings yet
- Skin - Part 2Document123 pagesSkin - Part 2Icee SinlapasertNo ratings yet
- CCPE บทความจากสาขาเครื่องสำอางDocument20 pagesCCPE บทความจากสาขาเครื่องสำอางRtgg PKNo ratings yet
- บทความ Antimicrobial Dosing Concepts in Patients With Reduced Kidney FunctionDocument20 pagesบทความ Antimicrobial Dosing Concepts in Patients With Reduced Kidney Functionqury quazaNo ratings yet
- SOAP2 แก้ไขแล้วDocument23 pagesSOAP2 แก้ไขแล้วSaritaSawatNo ratings yet
- กรณีศึกษาDocument18 pagesกรณีศึกษาGoy BubbiesNo ratings yet
- นำเสนอSOAPฝึกงาน กชกรDocument33 pagesนำเสนอSOAPฝึกงาน กชกรYo Turtle KidzNo ratings yet
- บทบาทเภสัชกรคุ้มครองผู้บริโภค ที่มีต่อระบบยาและสาธารณสุขDocument17 pagesบทบาทเภสัชกรคุ้มครองผู้บริโภค ที่มีต่อระบบยาและสาธารณสุขThe Pharmacy Council, Thailand100% (1)
- ปฏิบัติการที่ 8 Epilepsy Case1 S&ODocument9 pagesปฏิบัติการที่ 8 Epilepsy Case1 S&OEn Oh O EndNo ratings yet
- Tech 4 SuppositoryDocument14 pagesTech 4 SuppositoryKamegameNo ratings yet
- Clinical Comparison of Pseudoephedrine and PhenylephrineDocument8 pagesClinical Comparison of Pseudoephedrine and PhenylephrineKitiyot YotsombutNo ratings yet
- RDU Common ColdDocument8 pagesRDU Common ColdBeboh Photowindy100% (1)
- Biopharm, Epi EconDocument14 pagesBiopharm, Epi EconNutDen R X NuttapongNo ratings yet
- แนวทางเวชปฏิบัติเพื่อรักษาผู้ติดบุหรี่Document111 pagesแนวทางเวชปฏิบัติเพื่อรักษาผู้ติดบุหรี่เด็กชายสมันตภัทร แฟนคลับอาจารย์กวง100% (3)
- SOAPDocument3 pagesSOAPPépé TechopathamNo ratings yet
- Laboratory TestDocument16 pagesLaboratory TestZeazaa 陈秀香No ratings yet
- 7 Bacterial Meningitis - 129-134Document6 pages7 Bacterial Meningitis - 129-134Zeazaa 陈秀香No ratings yet
- (ร่าง) มาตรฐานร้านยาคุณภาพDocument21 pages(ร่าง) มาตรฐานร้านยาคุณภาพนิวัช สายนภาNo ratings yet
- การใช้ยาเทคนิคพิเศษDocument66 pagesการใช้ยาเทคนิคพิเศษMr. YellNo ratings yet
- Topical Dermatologic Products 18 สค 2015Document65 pagesTopical Dermatologic Products 18 สค 2015ตามา รถไฟมา ตามารถไฟ100% (5)
- คู่มือการใช้ยาในสตรีDocument19 pagesคู่มือการใช้ยาในสตรีเด็กชายท็อปปิ้ง ชอบกลิ้งเข้าคณะเภสัชศาสตร์No ratings yet
- แบบรายงานเหตุการณ์ไม่พึงประสงค์จากการใช้ผลิตภัณฑ์สุขภาพDocument5 pagesแบบรายงานเหตุการณ์ไม่พึงประสงค์จากการใช้ผลิตภัณฑ์สุขภาพIcee Sinlapasert100% (1)
- ใบงานระบบระบบร่างกายDocument6 pagesใบงานระบบระบบร่างกายชื่อยาววววว 'วววNo ratings yet
- Steroid PotencyDocument2 pagesSteroid PotencyTheerasakNo ratings yet
- Quiz 3Document2 pagesQuiz 3Mr. YellNo ratings yet
- Drug Monograph SodamintDocument5 pagesDrug Monograph Sodamintdeltafox007No ratings yet
- รอยแผลเป็น นิภาพรDocument39 pagesรอยแผลเป็น นิภาพรNeelapaijit DA NipapondNo ratings yet
- ประเภทของมอยส์เจอไรเซอร์ และวิธีการเลือกใช้ให้ถูกต้อง - sophistmedicDocument1 pageประเภทของมอยส์เจอไรเซอร์ และวิธีการเลือกใช้ให้ถูกต้อง - sophistmedicNanthicha KrajangpawNo ratings yet
- เวชสำอางเพื่อการชะลอวัยDocument8 pagesเวชสำอางเพื่อการชะลอวัยเด็กชายสมันตภัทร แฟนคลับอาจารย์กวง100% (1)
- Pre-Op Skin PrepDocument12 pagesPre-Op Skin PrepRungtip RuangnaparatNo ratings yet
- 104962449 วิธีกินยาDocument8 pages104962449 วิธีกินยาbuaby005No ratings yet
- สำเนา Seminar - microemulsion in Anti-Acne Drug 230930Document18 pagesสำเนา Seminar - microemulsion in Anti-Acne Drug 2309306210710023No ratings yet