You might also like
- Classification of AnaemiaDocument2 pagesClassification of AnaemiaAnand_Ram_7113No ratings yet
- Hematology Notes for Medical StudentsFrom EverandHematology Notes for Medical StudentsRating: 5 out of 5 stars5/5 (1)
- Decreased Hemoglobin Available For Erythrocytes Microcytic, Hypochromic Anemia More Hemoglobin Available For Erythrocytes Macrocytic AnemiaDocument2 pagesDecreased Hemoglobin Available For Erythrocytes Microcytic, Hypochromic Anemia More Hemoglobin Available For Erythrocytes Macrocytic AnemiaIB leaksNo ratings yet
- Haematology and Transfusions Caroline Young c2f 2013Document64 pagesHaematology and Transfusions Caroline Young c2f 2013api-195799092No ratings yet
- Pathophysiology of Acute Myelogenous Leukemia Fab m4Document3 pagesPathophysiology of Acute Myelogenous Leukemia Fab m4KristaMaeC.Lazo100% (2)
- AnemiaDocument6 pagesAnemiaHengli NatunaNo ratings yet
- Kuliah AnemiaaDocument44 pagesKuliah AnemiaaAhmad Umar AfNo ratings yet
- Anemias: Table Showing Types of Anemias and Causes Reticulocyte Count Microcytic Normocytic Macrocytic LOWDocument4 pagesAnemias: Table Showing Types of Anemias and Causes Reticulocyte Count Microcytic Normocytic Macrocytic LOWbrown_chocolate87643No ratings yet
- Super Simplified Pathology Hematology - Dr. Priyanka SachdevDocument500 pagesSuper Simplified Pathology Hematology - Dr. Priyanka SachdevMohd SaquibNo ratings yet
- Update On (Approach To) AnemiaDocument44 pagesUpdate On (Approach To) AnemiaIsaac MwangiNo ratings yet
- Tes Darah LengkapDocument18 pagesTes Darah Lengkapanisa rachmitaNo ratings yet
- USMLE - Heme & Lymph PathologyDocument21 pagesUSMLE - Heme & Lymph PathologyMatt McGlothlinNo ratings yet
- Hematology Mudit Khanna PDFDocument40 pagesHematology Mudit Khanna PDFSylvia DiamondNo ratings yet
- COMPLETE BLOOD PICTURE Ok-1 PDFDocument78 pagesCOMPLETE BLOOD PICTURE Ok-1 PDFEmanuel100% (1)
- Megaloblastic AnemiaDocument13 pagesMegaloblastic AnemiaManchlaNo ratings yet
- Aematology: Col Kamran AfzalDocument32 pagesAematology: Col Kamran AfzalZaraNo ratings yet
- Ana IfDocument101 pagesAna Ifshrikrishnapathlab100% (1)
- Haematolgy NotesDocument4 pagesHaematolgy NotesLuqman QadirNo ratings yet
- Diseases of The Bone Marrow and Blood Conditions That Can Occur When The Blood-Forming Cells in The Bone Marrow Become AbnormalDocument4 pagesDiseases of The Bone Marrow and Blood Conditions That Can Occur When The Blood-Forming Cells in The Bone Marrow Become AbnormalLuqman QadirNo ratings yet
- HematologyDocument42 pagesHematologyadaako100% (8)
- Hematology 1Document61 pagesHematology 1katz_hotchickNo ratings yet
- Peripheral Blood SmearDocument46 pagesPeripheral Blood SmearAris ResurreccionNo ratings yet
- He Ma To Pathology WebDocument100 pagesHe Ma To Pathology Webusamas85556No ratings yet
- Hematology تفريغ د شافعي 2013Document45 pagesHematology تفريغ د شافعي 2013Arwa Qishta100% (1)
- Hematopoietic System PathologyDocument78 pagesHematopoietic System PathologyNuhu SibaNo ratings yet
- Introduction To HematologyDocument23 pagesIntroduction To HematologyReba PhiliposeNo ratings yet
- RBC DisordersDocument27 pagesRBC Disordersbpt2100% (1)
- Understanding Anemia: Causes, Symptoms, Diagnosis and TreatmentDocument33 pagesUnderstanding Anemia: Causes, Symptoms, Diagnosis and TreatmentPurple basketNo ratings yet
- Microcytic Hypochromic Macrocytic Normochromic Normocytic: Anemia HematocritDocument7 pagesMicrocytic Hypochromic Macrocytic Normochromic Normocytic: Anemia Hematocritjjjj31No ratings yet
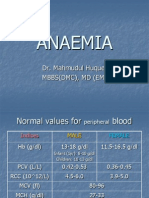
- Anaemia: Dr. Mahmudul Huque. Mbbs (DMC), MD (Em)Document32 pagesAnaemia: Dr. Mahmudul Huque. Mbbs (DMC), MD (Em)Junayed Safar MahmudNo ratings yet
- PejowebApproach To Anemia by Dr. Joel Solorzani RomeroDocument57 pagesPejowebApproach To Anemia by Dr. Joel Solorzani RomeroAshraf FaragNo ratings yet
- Peripheral Smear Examination PDFDocument91 pagesPeripheral Smear Examination PDFtufis02No ratings yet
- RED CELL MORPHOLOGY Tabulation SummaryDocument6 pagesRED CELL MORPHOLOGY Tabulation SummaryStephen YorNo ratings yet
- Hematology: AnemiaDocument46 pagesHematology: AnemiaCyrus100% (1)
- BoardReviewPart1A BenignHemePathDocument170 pagesBoardReviewPart1A BenignHemePathMaria Cristina Alarcon NietoNo ratings yet
- Blood SystemDocument14 pagesBlood SystemNguyễn MinhNo ratings yet
- Coagulation Problems PPTDocument69 pagesCoagulation Problems PPTBao NguyenNo ratings yet
- Red Blood Cell Disorders ExplainedDocument106 pagesRed Blood Cell Disorders ExplainedCharmaine Clarke-BlytheNo ratings yet
- Red Blood Cells PathologyDocument47 pagesRed Blood Cells PathologyRodriguez Vivanco Kevin DanielNo ratings yet
- 21 Anaemia and PancytopeniaDocument42 pages21 Anaemia and PancytopeniaLeon Hui MingNo ratings yet
- HaematopathologyDocument253 pagesHaematopathologyamyNo ratings yet
- AnemiaDocument56 pagesAnemiaSivaNo ratings yet
- Lecture 3rd. AnemiaDocument39 pagesLecture 3rd. Anemiaعمیرسعید قاضیNo ratings yet
- Clinical Internship: Hematology: WBC AnomaliesDocument8 pagesClinical Internship: Hematology: WBC AnomaliesNaomi NicoleNo ratings yet
- L4 Hemolytic AnaemiaDocument85 pagesL4 Hemolytic AnaemiaVenniilaaSaravananNo ratings yet
- Anemia: Dr. Tahira Jehangir Assistant Professor, Pharmacology Department NWSM, PeshawarDocument35 pagesAnemia: Dr. Tahira Jehangir Assistant Professor, Pharmacology Department NWSM, PeshawarAsif KhanNo ratings yet
- Shelly AnemiaDocument56 pagesShelly AnemiaSylda Rakmah Syarti IINo ratings yet
- Myeloproliferative NeoplasmsDocument59 pagesMyeloproliferative NeoplasmssaketNo ratings yet
- Hematology Review: by Felicia Magee Tardy, M.S., MT (Ascp)Document52 pagesHematology Review: by Felicia Magee Tardy, M.S., MT (Ascp)Reen LeenNo ratings yet
- Abnormal RBC in HistologyDocument24 pagesAbnormal RBC in HistologyG M TAMIM CHOWDHURY789No ratings yet
- Types of Anaemia and How To Remember Them: With Sophie BroughtonDocument28 pagesTypes of Anaemia and How To Remember Them: With Sophie BroughtonurtikikeNo ratings yet
- Clasification of Anemia: Prof. Dr. Adi Koesoema Aman SPPK (KH) Dr. Malayana Nasutioan Mked - SPPKDocument46 pagesClasification of Anemia: Prof. Dr. Adi Koesoema Aman SPPK (KH) Dr. Malayana Nasutioan Mked - SPPKrubyniNo ratings yet
- AnaemiaDocument34 pagesAnaemiadakshpanchal26369No ratings yet
- 19 Intro To AnemiaDocument3 pages19 Intro To AnemiaPeter JosephNo ratings yet
- Penyakit HematologiDocument128 pagesPenyakit HematologiLintang SuroyaNo ratings yet
- Anemia: Iin Novita Nurhidayati Mahmuda FK Ums Rs Pku Muhammadiyah SurakartaDocument55 pagesAnemia: Iin Novita Nurhidayati Mahmuda FK Ums Rs Pku Muhammadiyah Surakartafenti nurul khafifahNo ratings yet
- Anemia OsamaDocument57 pagesAnemia Osamaosamafoud7710No ratings yet
- Past Papers - 4.01 AnaemiaDocument29 pagesPast Papers - 4.01 Anaemianoob1314No ratings yet
- Cah SaqDocument5 pagesCah Saqnoob1314No ratings yet
- Skeletal Vs Cardiac Vs SmoothDocument2 pagesSkeletal Vs Cardiac Vs Smoothnoob1314No ratings yet
- Voice ExercisesDocument2 pagesVoice Exercisesnoob1314No ratings yet
- Core Presentations Template CoverDocument1 pageCore Presentations Template Covernoob1314No ratings yet
- Past Papers - 4.03 Bleeding DisorderDocument14 pagesPast Papers - 4.03 Bleeding Disordernoob1314No ratings yet
- Past Papers - 4.05 DVTDocument17 pagesPast Papers - 4.05 DVTnoob1314No ratings yet
- Past Papers - 4.05 DVTDocument17 pagesPast Papers - 4.05 DVTnoob1314No ratings yet
- Past Papers - 4.02 LeukaemiaDocument18 pagesPast Papers - 4.02 Leukaemianoob1314No ratings yet
- Colorectal Cancer TableDocument1 pageColorectal Cancer Tablenoob1314No ratings yet
- Past Papers - 4.05 Iron Deficiency in PregnancyDocument8 pagesPast Papers - 4.05 Iron Deficiency in Pregnancynoob1314No ratings yet
- Block 4 Revision SbaDocument38 pagesBlock 4 Revision Sbanoob1314No ratings yet
- Past Papers - 4.04 ThalassaemiaDocument13 pagesPast Papers - 4.04 Thalassaemianoob1314No ratings yet
- Past Papers - 4.04 Malaria - Infective FeverDocument2 pagesPast Papers - 4.04 Malaria - Infective Fevernoob1314No ratings yet
- Upper Limb Nerve LesionsDocument7 pagesUpper Limb Nerve Lesionsnoob1314No ratings yet
- CSL30 - Tom SmithDocument3 pagesCSL30 - Tom Smithnoob1314No ratings yet
- Indigenous Q ADocument2 pagesIndigenous Q Anoob1314No ratings yet
- Background InfoDocument5 pagesBackground Infonoob1314No ratings yet
- Causes, Mechanisms and Consequences of Acute and Chronic GastritisDocument9 pagesCauses, Mechanisms and Consequences of Acute and Chronic Gastritisnoob1314No ratings yet
- Exam Questions Based On DR Ellyard's ClassesDocument1 pageExam Questions Based On DR Ellyard's Classesnoob1314No ratings yet
- Screw Home MechanismDocument2 pagesScrew Home Mechanismnoob1314No ratings yet
- Quotes Gamsat Section 2Document9 pagesQuotes Gamsat Section 2noob1314No ratings yet
- Astronomy InvestigationDocument7 pagesAstronomy Investigationnoob1314No ratings yet
- Odysseus' World ExploredDocument14 pagesOdysseus' World Explorednoob1314No ratings yet
- Health EthicsDocument2 pagesHealth Ethicsnoob1314No ratings yet
- Mcribogioly Revision LectureDocument5 pagesMcribogioly Revision Lecturenoob1314No ratings yet
- Haemodynamic SDocument4 pagesHaemodynamic Snoob1314No ratings yet
- CHEM1011 N. Roberts: Naming Inorganic Compounds Naming Inorganic CompoundsDocument4 pagesCHEM1011 N. Roberts: Naming Inorganic Compounds Naming Inorganic Compoundsnoob1314No ratings yet
- Notes For SCIF1111Document3 pagesNotes For SCIF1111noob1314No ratings yet