You might also like
- Nursing Care Plan For Covid-19 PatientDocument4 pagesNursing Care Plan For Covid-19 PatientAkande83% (6)
- Therapy Ed 2018 223-231Document9 pagesTherapy Ed 2018 223-231Walter del AguilaNo ratings yet
- Ananth Narayan and Paniker 11th EditionDocument42 pagesAnanth Narayan and Paniker 11th EditionArjun Kandara50% (2)
- Impact of Random Assignment On Study Outcome: An Empirical ExaminationDocument12 pagesImpact of Random Assignment On Study Outcome: An Empirical ExaminationC NortonNo ratings yet
- Establishing The Internal and External Validity of Experimental StudiesDocument9 pagesEstablishing The Internal and External Validity of Experimental Studieskeramatboy88No ratings yet
- Considerations For Planning and Designing Meta-Analysis in Oral MedicineDocument9 pagesConsiderations For Planning and Designing Meta-Analysis in Oral Medicinedrvivek reddyNo ratings yet
- Evidence Based PracticeDocument28 pagesEvidence Based Practiceraghad awwadNo ratings yet
- "Evidence-Based Medicine": Department of Clinical PharmacologyDocument26 pages"Evidence-Based Medicine": Department of Clinical PharmacologyLucas Victor AlmeidaNo ratings yet
- Part 17 PDFDocument6 pagesPart 17 PDFKarolina PolskaNo ratings yet
- Resumo Tipos EstudoDocument5 pagesResumo Tipos EstudosusanammNo ratings yet
- Sample ChapterDocument12 pagesSample ChapterCinthia Gonzalez NunezNo ratings yet
- Clinical Trials BookDocument11 pagesClinical Trials BookMaria SpatariNo ratings yet
- Malone - CH 5Document70 pagesMalone - CH 5kola belloNo ratings yet
- Fixed or Random Effects Meta Analysis Common.12Document12 pagesFixed or Random Effects Meta Analysis Common.12Yusuf RachmanNo ratings yet
- An Evidence-Based Approach To Zygomatic Fractures: Clinical ScenarioDocument7 pagesAn Evidence-Based Approach To Zygomatic Fractures: Clinical ScenarioyanuararipratamaNo ratings yet
- Clinicalresearchfocus: The Research QuestionDocument4 pagesClinicalresearchfocus: The Research QuestionNiputu CintyadewiNo ratings yet
- The Use of Historical Controls in Post-Test Only Non-Equivalent Control GroupDocument10 pagesThe Use of Historical Controls in Post-Test Only Non-Equivalent Control GroupEditor IJTSRDNo ratings yet
- Diya Sana K N - Research MethodologyDocument22 pagesDiya Sana K N - Research MethodologydiywritesanunknownwriterNo ratings yet
- B Metris 2 - Summary Study DesignsDocument28 pagesB Metris 2 - Summary Study DesignsSawada TsunayoshiNo ratings yet
- Z Al-Roubaie - 2020Document12 pagesZ Al-Roubaie - 2020Kossay ZaouiNo ratings yet
- Meta-Analysis: A Tool For Clinical and Experimental Research in PsychiatryDocument8 pagesMeta-Analysis: A Tool For Clinical and Experimental Research in PsychiatryΑβραξας ΓαβριήλNo ratings yet
- Yuan 2012Document12 pagesYuan 2012Renata YolandaNo ratings yet
- Medical Statistics: Lecture 2: Types of Medical StudiesDocument14 pagesMedical Statistics: Lecture 2: Types of Medical StudiesamirNo ratings yet
- MINORS Criteria For Non-Randomized StudiesDocument5 pagesMINORS Criteria For Non-Randomized StudiesRamiro Manzano NúñezNo ratings yet
- Research Fundamentals: IV. Choosing A Research Design: K N. H, MD, R U. K, MDDocument8 pagesResearch Fundamentals: IV. Choosing A Research Design: K N. H, MD, R U. K, MDJoseph Dela CruzNo ratings yet
- What Is Clinical ReviewDocument3 pagesWhat Is Clinical ReviewTia ListyanaNo ratings yet
- 1 - Outcomes ResearchDocument12 pages1 - Outcomes ResearchMauricio Ruiz MoralesNo ratings yet
- Selection of Cases and Controls IDocument10 pagesSelection of Cases and Controls Isergioarciniegas29No ratings yet
- Downs and Black (1998)Document8 pagesDowns and Black (1998)ASHISH KUMARNo ratings yet
- Blinding Protocols, Treatment Credbility, and Expectancy - Methodologic Issues in Clinical Trial of Osteopathic Manipulative TreatmentDocument7 pagesBlinding Protocols, Treatment Credbility, and Expectancy - Methodologic Issues in Clinical Trial of Osteopathic Manipulative TreatmentrafaelNo ratings yet
- 38 The Use of Meta-Analysis in Pharmacoepidemiology: Jesse A. BerlinDocument27 pages38 The Use of Meta-Analysis in Pharmacoepidemiology: Jesse A. BerlinFranklin garryNo ratings yet
- Factors That Influence Validity (1) : Study Design, Doses and PowerDocument2 pagesFactors That Influence Validity (1) : Study Design, Doses and PowerHabib DawarNo ratings yet
- Cross-Sectional Studies: Strengths, Weaknesses, and RecommendationsDocument7 pagesCross-Sectional Studies: Strengths, Weaknesses, and RecommendationsHesed VirtoNo ratings yet
- Early Practice Focus Evidenc Based Practice in Facial Plastic SurgeryDocument13 pagesEarly Practice Focus Evidenc Based Practice in Facial Plastic SurgeryariskaNo ratings yet
- Chapter 2 - Introduction To Quantitative ResearchDocument62 pagesChapter 2 - Introduction To Quantitative ResearchIconMaicoNo ratings yet
- Curtin 2017Document12 pagesCurtin 2017jmdrg2No ratings yet
- Types of Research StudiesDocument38 pagesTypes of Research Studiesنزار الحرازيNo ratings yet
- Research Design: Faculty of Public Health, Khon Kaen UniversityDocument32 pagesResearch Design: Faculty of Public Health, Khon Kaen UniversityWhatever UseeNo ratings yet
- NIH Public Access: Author ManuscriptDocument16 pagesNIH Public Access: Author ManuscriptMarvin BundoNo ratings yet
- Kassirer 1989Document8 pagesKassirer 1989diegoarmandomargueNo ratings yet
- Reviewon QualityassessmentDocument13 pagesReviewon QualityassessmentnewsPewNo ratings yet
- Evaluation of Scientific Publications - Part 20 - Establishing Equivalence or Non-Inferiority in Clinical Trials PDFDocument6 pagesEvaluation of Scientific Publications - Part 20 - Establishing Equivalence or Non-Inferiority in Clinical Trials PDFPhoNo ratings yet
- The Meta-Analysis in Evidence-Based Medicine: High-Quality Research When Properly PerformedDocument3 pagesThe Meta-Analysis in Evidence-Based Medicine: High-Quality Research When Properly PerformedAdin SuryaNo ratings yet
- How To Write A Research Paper: EditorialDocument2 pagesHow To Write A Research Paper: EditorialjustinohaganNo ratings yet
- EPI 2.05 Overview of Analytic Observational StudiesDocument7 pagesEPI 2.05 Overview of Analytic Observational StudiesJoher MendezNo ratings yet
- PPC15 Biostatistics WorkbookDocument22 pagesPPC15 Biostatistics WorkbookongolebasilNo ratings yet
- Research Designs in Clinical EpidemiologyDocument8 pagesResearch Designs in Clinical EpidemiologyDulce Nalleli Aguilar TejedaNo ratings yet
- Review Bias in Clinical Intervention ResearchDocument9 pagesReview Bias in Clinical Intervention ResearchHesed VirtoNo ratings yet
- Rating The Quality of Evidence-InconsistencyDocument9 pagesRating The Quality of Evidence-InconsistencyGeorgina CNo ratings yet
- Research MethodologyDocument6 pagesResearch MethodologyKumiqinNo ratings yet
- Hierarchy of Evidence Factsheet v1 11042016 PDFDocument2 pagesHierarchy of Evidence Factsheet v1 11042016 PDFMirja AdiyaksaNo ratings yet
- Scientific ResearchDocument18 pagesScientific ResearchRenz Marjolino Dasilio100% (1)
- CriticalAppraisalWorksheetSys ReviewDocument2 pagesCriticalAppraisalWorksheetSys Reviewimroatul ulyaNo ratings yet
- Principles of Drug Literature Evaluation For Observational Study DesignsDocument13 pagesPrinciples of Drug Literature Evaluation For Observational Study Designs李姵瑩No ratings yet
- Retrospective Studies and Chart Reviews: Dean R Hess PHD RRT FaarcDocument4 pagesRetrospective Studies and Chart Reviews: Dean R Hess PHD RRT Faarcdoc_next_doorNo ratings yet
- Critical Appraisal of Studies Using Laboratory Animal ModelsDocument13 pagesCritical Appraisal of Studies Using Laboratory Animal ModelsRahmanu ReztaputraNo ratings yet
- Hierarchy and VariablesDocument3 pagesHierarchy and VariablesAshley WuNo ratings yet
- What Is Scientific Research and How Can It Be DoneDocument10 pagesWhat Is Scientific Research and How Can It Be DoneSanjay ChouhanNo ratings yet
- Critical Appraisal Guide: Research MethodologyDocument3 pagesCritical Appraisal Guide: Research MethodologylizNo ratings yet
- 3.1 Randomized Control Trials PDFDocument4 pages3.1 Randomized Control Trials PDFPia BustosNo ratings yet
- Nciph ERIC10Document5 pagesNciph ERIC10bejarhasanNo ratings yet
- Concise Biostatistical Principles & Concepts: Guidelines for Clinical and Biomedical ResearchersFrom EverandConcise Biostatistical Principles & Concepts: Guidelines for Clinical and Biomedical ResearchersNo ratings yet
- Practical Oncologic Molecular Pathology: Frequently Asked QuestionsFrom EverandPractical Oncologic Molecular Pathology: Frequently Asked QuestionsNo ratings yet
- Vaccination Programs in Poultry - Poultry - Merck Veterinary MaDocument9 pagesVaccination Programs in Poultry - Poultry - Merck Veterinary MaSamapanNo ratings yet
- Toronto Notes - Case 4 - DiabetesDocument1 pageToronto Notes - Case 4 - DiabetesSumer ChauhanNo ratings yet
- Satuan Acara Penyuluhan Penanganan Dan Pencegahan Penyakit PanuDocument8 pagesSatuan Acara Penyuluhan Penanganan Dan Pencegahan Penyakit PanuRamayanaNo ratings yet
- ProstatitisDocument19 pagesProstatitischithranuNo ratings yet
- Torrent Downloaded From Extratorrent - CCDocument33 pagesTorrent Downloaded From Extratorrent - CCDhytzz AbejoNo ratings yet
- NCP Risk For InfectionDocument2 pagesNCP Risk For InfectionI Am SmilingNo ratings yet
- COMMUNITY DENTISTRY AND PUBLIC HEALTHqDocument6 pagesCOMMUNITY DENTISTRY AND PUBLIC HEALTHqLangNo ratings yet
- White Blue Modern Marine Pollution InfographicDocument2 pagesWhite Blue Modern Marine Pollution InfographicJanella Mae C. RiegoNo ratings yet
- Manifestations of Miasms in DiseaseDocument3 pagesManifestations of Miasms in Diseaselydia2301100% (2)
- Disorders of The Respiratory SystemDocument9 pagesDisorders of The Respiratory SystemAjay Pal NattNo ratings yet
- Opportunistic Moulds 13-03-2014Document22 pagesOpportunistic Moulds 13-03-2014Ian MosesNo ratings yet
- Pseudomembranous Candidiasis Induced byDocument5 pagesPseudomembranous Candidiasis Induced byGenevieve Florencia Natasya SaraswatiNo ratings yet
- Antibiotik GangrenDocument10 pagesAntibiotik GangrenMutiara Khaerun NisaNo ratings yet
- Clinical Communications: Pediatric: Pediatric Sepsis Secondary To An Occult Dental Abscess: A Case ReportDocument5 pagesClinical Communications: Pediatric: Pediatric Sepsis Secondary To An Occult Dental Abscess: A Case Reportdelfi simatupangNo ratings yet
- COPD - Jindal Chest ClinicDocument31 pagesCOPD - Jindal Chest ClinicJindal Chest ClinicNo ratings yet
- An Overview of Muscle Histopathology in Myositis: Differentiating Subtypes of MyositisDocument35 pagesAn Overview of Muscle Histopathology in Myositis: Differentiating Subtypes of MyositisIsaac MaderoNo ratings yet
- Ischemic StrokeDocument8 pagesIschemic StrokeSofía Maltés GarridoNo ratings yet
- Infective Endocarditis1Document50 pagesInfective Endocarditis1Eman ShNo ratings yet
- Misdiagnosis and Misuse of Medication in AdhdDocument5 pagesMisdiagnosis and Misuse of Medication in AdhdAyub MaingiNo ratings yet
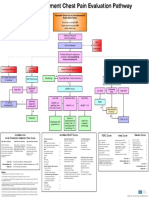
- Emergency Department Chest Pain Evaluation PathwayDocument2 pagesEmergency Department Chest Pain Evaluation Pathwaymuhammad sajidNo ratings yet
- Hepatitis A: Key FactsDocument4 pagesHepatitis A: Key FactskasokiNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsPasula VishalNo ratings yet
- ICD 10 - Chapter 1 Certain Infectious and Parasitic DiseasesDocument16 pagesICD 10 - Chapter 1 Certain Infectious and Parasitic DiseasesHuseikha VelayazulfahdNo ratings yet
- Medication For URTI Symptoms YKDocument12 pagesMedication For URTI Symptoms YKYee Kwan LiewNo ratings yet
- Contagious Bovine Pleuropneumonia: DR. DK Singh Pathologist, IAASDocument34 pagesContagious Bovine Pleuropneumonia: DR. DK Singh Pathologist, IAASSuraj_SubediNo ratings yet
- Presentation On Epistaxis in ChildrenDocument39 pagesPresentation On Epistaxis in ChildrenAdditi SatyalNo ratings yet
- Dzexams 2am Anglais 833192Document3 pagesDzexams 2am Anglais 833192sarasara199630No ratings yet