You might also like
- Optimal Operating Room Design IIIDocument9 pagesOptimal Operating Room Design IIIMinhNo ratings yet
- Optimize Green Warehouse LocationDocument23 pagesOptimize Green Warehouse LocationBhavya KhattarNo ratings yet
- Research Fifty (50) Bed Level 1 Government General Hospital: College of ArchitectureDocument29 pagesResearch Fifty (50) Bed Level 1 Government General Hospital: College of ArchitectureGerardo, Liano Ezekiel N.No ratings yet
- What Does It Take To Run An ICU or Perioperative Medicine ServiceDocument19 pagesWhat Does It Take To Run An ICU or Perioperative Medicine Servicefriday ChitsongaNo ratings yet
- Pandemic Resilient HospitalDocument17 pagesPandemic Resilient HospitalClarisse DoriaNo ratings yet
- Renzael (2015)Document31 pagesRenzael (2015)German Gabriel Anaya VegaNo ratings yet
- Welcome To The Era of Universal Airway Management: EditorialDocument5 pagesWelcome To The Era of Universal Airway Management: EditorialHugo Robles GómezNo ratings yet
- 61 NandhanaRK Electives ReportDocument12 pages61 NandhanaRK Electives ReportnandhanaNo ratings yet
- Design Guidelines HospitalDocument39 pagesDesign Guidelines HospitalKhaled FacebNo ratings yet
- 0731 HMSDocument5 pages0731 HMSDegele TadesseNo ratings yet
- Creating+Order+Out+of+Chaos+ +a+Leadership+Approach+ +2010 +2010 +2010 +2010 +2010Document18 pagesCreating+Order+Out+of+Chaos+ +a+Leadership+Approach+ +2010 +2010 +2010 +2010 +2010Anita FaúndezNo ratings yet
- Teleworking and workplace flexibility impact on firm performanceDocument23 pagesTeleworking and workplace flexibility impact on firm performanceMuhammad FaizNo ratings yet
- DESIGN AND ANALYSIS OF A MULTISPECIALTY HOSPITALDocument10 pagesDESIGN AND ANALYSIS OF A MULTISPECIALTY HOSPITALRAHUL C RNo ratings yet
- Malkin CH1 PDFDocument11 pagesMalkin CH1 PDFPatriciaMariaNo ratings yet
- A Theoretical Review of Flexibility Agility and ReDocument25 pagesA Theoretical Review of Flexibility Agility and ReNanda NogueiraNo ratings yet
- Establishing_a_new_cardiac_surgical_unit_ChallengeDocument4 pagesEstablishing_a_new_cardiac_surgical_unit_ChallengeJoji BorromeoNo ratings yet
- Grisaru v5 Final PDFDocument9 pagesGrisaru v5 Final PDFrajimuruganNo ratings yet
- Design Considerations For Collaborative CareDocument28 pagesDesign Considerations For Collaborative CareJulian HutabaratNo ratings yet
- 6 - Summary - Maximising Usability - The Principles of Universal DesignDocument2 pages6 - Summary - Maximising Usability - The Principles of Universal DesignShibani ShashinNo ratings yet
- Makespan Performance Improvement Through Flexibility Enabled Concurrency - Understanding The Underlying Mechanisms of RoutingDocument12 pagesMakespan Performance Improvement Through Flexibility Enabled Concurrency - Understanding The Underlying Mechanisms of RoutingKristin MackNo ratings yet
- Value StreamDocument11 pagesValue Streamluis anchayhua pradoNo ratings yet
- Artículo de TRABAJO ESTANDARIZADO Frangeskou2020Document23 pagesArtículo de TRABAJO ESTANDARIZADO Frangeskou2020luis miguelNo ratings yet
- Operating Room DesignDocument15 pagesOperating Room DesignKousik AmancharlaNo ratings yet
- Earthy 1998 - Umm-HcsDocument34 pagesEarthy 1998 - Umm-HcsGustavo Cláudio Benedito MeloNo ratings yet
- Frameworks For Learner Assessment in Medicine: AMEE Guide No. 78Document15 pagesFrameworks For Learner Assessment in Medicine: AMEE Guide No. 78Raneem FathyNo ratings yet
- Universalism, Universal Design and Equitable Access To The Built EnvironmentDocument10 pagesUniversalism, Universal Design and Equitable Access To The Built EnvironmentTeodora NedelcuNo ratings yet
- Executive Summary Reducing Care FragmentationDocument5 pagesExecutive Summary Reducing Care FragmentationswestyNo ratings yet
- Simulation and Its Role in Medical Education: Contemporary IssueDocument6 pagesSimulation and Its Role in Medical Education: Contemporary IssueYorim Sora PasilaNo ratings yet
- Healthcare Sustainability Evaluation Using A Hybrid Fuzzy Multi-Criteria Decision-Making ModelDocument21 pagesHealthcare Sustainability Evaluation Using A Hybrid Fuzzy Multi-Criteria Decision-Making ModelANKUSH SINHANo ratings yet
- Strategic ConvergenceDocument42 pagesStrategic ConvergencerajneeshchowdhuryNo ratings yet
- Operation and Maintenance in Facilities Management Practices: A Gap Analysis in MalaysiaDocument7 pagesOperation and Maintenance in Facilities Management Practices: A Gap Analysis in MalaysiaNateNo ratings yet
- Improving Knowledge Provision For Shared Decision Making in Patient-Physician Relationships - A Multiagent Organizational ApproachDocument10 pagesImproving Knowledge Provision For Shared Decision Making in Patient-Physician Relationships - A Multiagent Organizational ApproachLaily HidayatiNo ratings yet
- Critical Control Rooms - Managing ChangeDocument9 pagesCritical Control Rooms - Managing ChangeJin JiangNo ratings yet
- BIT ManifestoDocument110 pagesBIT ManifestoRoman SchulzNo ratings yet
- Essential Guide-Maximize Lab Performance PDFDocument40 pagesEssential Guide-Maximize Lab Performance PDFAnonymous 9FaBkBktNo ratings yet
- Quality Function Deployment and Its Profitability Engagement: A Systems Thinking PerspectiveDocument19 pagesQuality Function Deployment and Its Profitability Engagement: A Systems Thinking PerspectiveLina marcela Pardo buenoNo ratings yet
- Guidelines and Pathways For Clinical Practice in Tendinopathy: Their Role and DevelopmentDocument1 pageGuidelines and Pathways For Clinical Practice in Tendinopathy: Their Role and Development7fsfgjss6tNo ratings yet
- Hospital Information Systems PlanningDocument9 pagesHospital Information Systems PlanningMayada El attarNo ratings yet
- ACD 2009 v7Document7 pagesACD 2009 v7gabs521No ratings yet
- AlinIQ AMS GuideDocument40 pagesAlinIQ AMS GuidesootjeNo ratings yet
- Translation Engine in Support of Context-Level InteroperabilityDocument9 pagesTranslation Engine in Support of Context-Level InteroperabilityMusasimaru HojotosiNo ratings yet
- Functional Requirements As An Integral Part of The Design and Development Process: Summary and RecommendationsDocument18 pagesFunctional Requirements As An Integral Part of The Design and Development Process: Summary and RecommendationsJanu RomansyahNo ratings yet
- The Road Map: From Little Victories To Systematic TransformationDocument22 pagesThe Road Map: From Little Victories To Systematic TransformationdrsohifNo ratings yet
- Hospital Facility Layout: Design Advisor SponsorDocument5 pagesHospital Facility Layout: Design Advisor SponsorVictor Conrad AlinioNo ratings yet
- MGM102 Test 1 SA 2016Document2 pagesMGM102 Test 1 SA 2016Amy WangNo ratings yet
- Artigo - Microlearning For Patient SafetyDocument20 pagesArtigo - Microlearning For Patient Safetyorquidia jaquimNo ratings yet
- ECM Lab Preread M ModelDocument8 pagesECM Lab Preread M ModelAdriana Q.No ratings yet
- Advantages and Disadvantages of Warehouse Centralization - Hospital CaseDocument8 pagesAdvantages and Disadvantages of Warehouse Centralization - Hospital CasejahsdjashdahdgadgNo ratings yet
- A Study of Current Maintenance Strategies and The Reliability of Critical Medical Equipment in Hospitals in Relation To Patient OutcomesDocument9 pagesA Study of Current Maintenance Strategies and The Reliability of Critical Medical Equipment in Hospitals in Relation To Patient OutcomesAya AhmedNo ratings yet
- Optimizing Hospital Building Design For Peak Hour EfficiencyDocument15 pagesOptimizing Hospital Building Design For Peak Hour Efficiencyluckylj0406No ratings yet
- Masters in HelathcareDocument6 pagesMasters in HelathcareNnamdiNo ratings yet
- How To Modify LeanDocument16 pagesHow To Modify Leanraphael boechatNo ratings yet
- Audit Assessment of The FacilitiesDocument17 pagesAudit Assessment of The FacilitiesrizkaNo ratings yet
- The Resilient Potential Behaviours in An Internal Medicine DepartmentDocument18 pagesThe Resilient Potential Behaviours in An Internal Medicine DepartmentDaniel fabian Sánchez henaoNo ratings yet
- A Medical Director's Perspective: The Making of An Outstanding Medical Director of Case ManagementDocument2 pagesA Medical Director's Perspective: The Making of An Outstanding Medical Director of Case Managementacma2010No ratings yet
- Visser-A Conceptual Framework For Maintenance ManagementDocument9 pagesVisser-A Conceptual Framework For Maintenance ManagementnuwanNo ratings yet
- Lean Models Classification Towards A Holistic ViewDocument9 pagesLean Models Classification Towards A Holistic ViewbayramNo ratings yet
- 2011 - Now Lets Make It Really Complex - GeralDocument26 pages2011 - Now Lets Make It Really Complex - GeralJossNo ratings yet
- Flexibility Adaptability in Hospital Design Construction 1twhvzoDocument46 pagesFlexibility Adaptability in Hospital Design Construction 1twhvzoJessa Dynn Agraviador VelardeNo ratings yet
- Plumbing ToolsDocument24 pagesPlumbing ToolsHarold Abubo Haber100% (4)
- Construction of Pervious PavementDocument37 pagesConstruction of Pervious PavementJessa Dynn Agraviador VelardeNo ratings yet
- Trendy Dimsum Afss PDFDocument1 pageTrendy Dimsum Afss PDFJessa Dynn Agraviador VelardeNo ratings yet
- Zoning and SoilDocument2 pagesZoning and SoilJessa Dynn Agraviador VelardeNo ratings yet
- Design ConceptDocument2 pagesDesign ConceptJessa Dynn Agraviador VelardeNo ratings yet
- Humanities ReportDocument78 pagesHumanities ReportJessa Dynn Agraviador VelardeNo ratings yet
- Construction of Pervious PavementDocument6 pagesConstruction of Pervious PavementJessa Dynn Agraviador VelardeNo ratings yet
- SouthernCoastal Frontyard LoresDocument2 pagesSouthernCoastal Frontyard LoresJessa Dynn Agraviador VelardeNo ratings yet
- Hotel Facility Design and Architectural ConstructionDocument7 pagesHotel Facility Design and Architectural ConstructionJessa Dynn Agraviador Velarde100% (1)
- Morphe 2008Document18 pagesMorphe 2008Jyro TriviñoNo ratings yet
- Datacollactionofresort 150217232203 Conversion Gate01Document62 pagesDatacollactionofresort 150217232203 Conversion Gate01Jessa Dynn Agraviador VelardeNo ratings yet
- Fire Code of The Philppines 2008 PDFDocument16 pagesFire Code of The Philppines 2008 PDFjpkhepNo ratings yet
- VelardeDocument32 pagesVelardeJessa Dynn Agraviador VelardeNo ratings yet
- Ekistic PrinciplesDocument1 pageEkistic PrinciplesJessa Dynn Agraviador VelardeNo ratings yet
- Planning 341: Ekistics: The Science of Human Settlements: Far Eastern UniversityDocument7 pagesPlanning 341: Ekistics: The Science of Human Settlements: Far Eastern UniversityJessa Dynn Agraviador VelardeNo ratings yet
- Architectura Space ProrammingDocument2 pagesArchitectura Space ProrammingJessa Dynn Agraviador VelardeNo ratings yet
- Planning ReportDocument21 pagesPlanning ReportJessa Dynn Agraviador VelardeNo ratings yet
- Design ResearchfinalsDocument10 pagesDesign ResearchfinalsJessa Dynn Agraviador VelardeNo ratings yet
- StructuresDocument4 pagesStructuresJessa Dynn Agraviador VelardeNo ratings yet
- Group4 Mixed Use DevelopmentDocument35 pagesGroup4 Mixed Use DevelopmentJessa Dynn Agraviador VelardeNo ratings yet
- Human Scale and TransparencyDocument2 pagesHuman Scale and TransparencyJessa Dynn Agraviador VelardeNo ratings yet
- Talisay City Plaza Complex RedevelopmentDocument1 pageTalisay City Plaza Complex RedevelopmentJessa Dynn Agraviador VelardeNo ratings yet
- Design ConceptDocument6 pagesDesign ConceptJessa Dynn Agraviador VelardeNo ratings yet
- Planning ReportDocument21 pagesPlanning ReportJessa Dynn Agraviador VelardeNo ratings yet
- Government Center Plaza Complex GuideDocument28 pagesGovernment Center Plaza Complex GuideJessa Dynn Agraviador Velarde100% (2)
- Trauma CenterDocument4 pagesTrauma CenterJessa Dynn Agraviador VelardeNo ratings yet
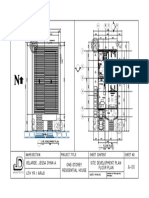
- Velarde, Jessa Dynn A. 4TH YR./ AR401 One-Storey Residential House Site Development Plan Floor PlanDocument1 pageVelarde, Jessa Dynn A. 4TH YR./ AR401 One-Storey Residential House Site Development Plan Floor PlanJessa Dynn Agraviador Velarde100% (1)
- Types of Pre-Cast Wall PanelDocument3 pagesTypes of Pre-Cast Wall PanelJessa Dynn Agraviador VelardeNo ratings yet
- Parallel Computing: # Registering Cores For Parallel ProcessDocument4 pagesParallel Computing: # Registering Cores For Parallel ProcessJohn SinghNo ratings yet
- Route StructureDocument3 pagesRoute StructureAndrei Gideon ReyesNo ratings yet
- Democracy Against Domination PDFDocument257 pagesDemocracy Against Domination PDFvmcosNo ratings yet
- LING-05 Assets and Liabilities of The English Language Prepared by Mario Pei and John Nist Edited by David F. MaasDocument17 pagesLING-05 Assets and Liabilities of The English Language Prepared by Mario Pei and John Nist Edited by David F. MaasDavid F Maas71% (7)
- Trauma-Informed CounselingDocument1 pageTrauma-Informed Counselingapi-492010604No ratings yet
- + or Cryptopotato - Com or U.today-Domain Domains-UsDocument128 pages+ or Cryptopotato - Com or U.today-Domain Domains-UsMalkeet SinghNo ratings yet
- Keerai BenefitsDocument3 pagesKeerai BenefitsjnaguNo ratings yet
- Mananquil v. MoicoDocument2 pagesMananquil v. Moicoangelo prietoNo ratings yet
- Data Center Cooling Solutions That Lower Costs With High Energy SavingsDocument5 pagesData Center Cooling Solutions That Lower Costs With High Energy Savingskhamsone pengmanivongNo ratings yet
- September/News/Septiembre 2013: P.O. Box 44 WWW - Hecatomberecords.esDocument7 pagesSeptember/News/Septiembre 2013: P.O. Box 44 WWW - Hecatomberecords.eshecatomberecordsNo ratings yet
- The Story of A Seagull and The Cat Who Taught Her To Fly PDFDocument46 pagesThe Story of A Seagull and The Cat Who Taught Her To Fly PDFYo Seven67% (3)
- Business Plan Template For AfterSchool ProgramsDocument6 pagesBusiness Plan Template For AfterSchool Programsshelana BarzeyNo ratings yet
- Advanced Engineering Mathematics 10th EditionDocument7 pagesAdvanced Engineering Mathematics 10th EditionsamuelNo ratings yet
- Digital Mining Technology CAS-GPS Light Vehicle System Technical SpecificationDocument5 pagesDigital Mining Technology CAS-GPS Light Vehicle System Technical SpecificationAbhinandan PadhaNo ratings yet
- English DWDM 2022 Book 7 Int Sample PagesDocument7 pagesEnglish DWDM 2022 Book 7 Int Sample PagesLuiz Roberto MartinesNo ratings yet
- Refunds Maceda Law and PD957Document2 pagesRefunds Maceda Law and PD957QUINTO CRISTINA MAENo ratings yet
- Lab Skill Workbook - Applied Physics - Seph0009 07-12-2023Document87 pagesLab Skill Workbook - Applied Physics - Seph0009 07-12-2023rahulsaitalasilaNo ratings yet
- Pricelist PT SCB Maret 2023Document11 pagesPricelist PT SCB Maret 2023PT RUKUN CAHAYA ABADINo ratings yet
- Module 6 Questions and AnswersDocument10 pagesModule 6 Questions and AnswersProject InfoNo ratings yet
- Prakash V MST SahaniDocument8 pagesPrakash V MST SahaniAditi IndraniNo ratings yet
- CAE Proposal Expressions and SamplesDocument6 pagesCAE Proposal Expressions and SamplesKimLiênNguyễnNo ratings yet
- Nilai Murni PKN XII Mipa 3Document8 pagesNilai Murni PKN XII Mipa 3ilmi hamdinNo ratings yet
- MMA2019 SDocument2 pagesMMA2019 SToni IbrahimNo ratings yet
- Jha 2018Document4 pagesJha 2018AditiNo ratings yet
- Handout-Wisdom QuestionsDocument1 pageHandout-Wisdom Questionsapi-369459770No ratings yet
- A Thief in Venice - Tara CrescentDocument108 pagesA Thief in Venice - Tara Crescentfilippa.lindenNo ratings yet
- (English (Auto-Generated) ) Reviving The Labor Movement - Margaret Levi - TEDxSeattle (DownSub - Com)Document14 pages(English (Auto-Generated) ) Reviving The Labor Movement - Margaret Levi - TEDxSeattle (DownSub - Com)Surat PEHKTNo ratings yet
- Final test grammar and vocabulary practiceDocument5 pagesFinal test grammar and vocabulary practicexico_euNo ratings yet
- Quotes by Swami VivekanandaDocument6 pagesQuotes by Swami Vivekanandasundaram108No ratings yet
- Sindhi 2020Document1 pageSindhi 2020Engr Javed AkhtarNo ratings yet