You might also like
- Paper Giving Advice and Nursing InstructionDocument6 pagesPaper Giving Advice and Nursing InstructionVionaysNo ratings yet
- M Fadillah Alfikri FLM Jiwa 1 - 1P - Konsep DasarDocument9 pagesM Fadillah Alfikri FLM Jiwa 1 - 1P - Konsep DasarSaid abdul jalil GassppooeellNo ratings yet
- Uts Aena Div Keperawatan Anestesiologi TK II Semester VIDocument1 pageUts Aena Div Keperawatan Anestesiologi TK II Semester VIpadila hipzahNo ratings yet
- Role Play DiareDocument7 pagesRole Play DiareNi Putu aristaNo ratings yet
- Octavia Tugas Akhir BingDocument3 pagesOctavia Tugas Akhir BingOctavia NurulNo ratings yet
- JURNAL Alifka OkDocument8 pagesJURNAL Alifka OkAlifka PratiwiNo ratings yet
- Introduction To PatientDocument6 pagesIntroduction To PatientKomang AprianiNo ratings yet
- Hipertension DialogueDocument2 pagesHipertension DialogueLeli Aprina100% (1)
- Nurse-Patient Relationship TheoriesDocument17 pagesNurse-Patient Relationship TheoriesAyu GuloNo ratings yet
- DAFTAR PUSTAKA Gadar 1Document2 pagesDAFTAR PUSTAKA Gadar 1Rini WahyuniNo ratings yet
- Proposal Terapi Aktivitas Kelompok Stimulasi PersepsiDocument9 pagesProposal Terapi Aktivitas Kelompok Stimulasi PersepsiMuhammad FarkhaniNo ratings yet
- Tugas Kelompok Ke IDocument12 pagesTugas Kelompok Ke IernawatiNo ratings yet
- UNIT 3 (What Do You Feel)Document33 pagesUNIT 3 (What Do You Feel)oktika100% (1)
- Penerapan Telenursing Dalam Pelayanan Kesehatan: Literature ReviewDocument8 pagesPenerapan Telenursing Dalam Pelayanan Kesehatan: Literature ReviewAdi RiskiNo ratings yet
- Hubungan Kegawat Daruratan Dengan Waktu Tanggap Pa-DikonversiDocument8 pagesHubungan Kegawat Daruratan Dengan Waktu Tanggap Pa-DikonversiRiskynurdianadespriyanti KikiNo ratings yet
- B.inggris (Applying IV Infusion)Document2 pagesB.inggris (Applying IV Infusion)Renika Dwi WahyuniNo ratings yet
- Soal Ujian Semester III D.iv TK - Ii.-1Document2 pagesSoal Ujian Semester III D.iv TK - Ii.-1anggunNo ratings yet
- SIMPRO Model For Effectivennes Nursing ModelDocument7 pagesSIMPRO Model For Effectivennes Nursing ModelcholiidNo ratings yet
- Calculating Nutritional Needs for PatientsDocument34 pagesCalculating Nutritional Needs for PatientsvandelNo ratings yet
- Analisa Kasus HIPERGLIKEMIDocument30 pagesAnalisa Kasus HIPERGLIKEMIanis dwi prakasiwiNo ratings yet
- Bhs InggrisDocument16 pagesBhs InggrisMuhammad WardiNo ratings yet
- Role Play Taking Blood SmpelDocument2 pagesRole Play Taking Blood SmpelRofiqNo ratings yet
- Knowledge On Nursing Check - Apr 2021Document6 pagesKnowledge On Nursing Check - Apr 2021Dewi Surya AdiningsihNo ratings yet
- Manuscript Head Up 30Document9 pagesManuscript Head Up 30Rahmat BudianaNo ratings yet
- Disinfectants and antiseptics substances functionsDocument4 pagesDisinfectants and antiseptics substances functionsFera NurjanahNo ratings yet
- Dialog Giving AdviceDocument1 pageDialog Giving AdviceIlham UtamaNo ratings yet
- Conversation Hand WashingDocument3 pagesConversation Hand WashingSindy OctaNo ratings yet
- Teks RomDocument5 pagesTeks RomNight RaidNo ratings yet
- Conversation About Suggestion For A Diabetic DietDocument2 pagesConversation About Suggestion For A Diabetic DietverilyNo ratings yet
- ID Faktor Faktor Yang Mempengaruhi TingkatDocument14 pagesID Faktor Faktor Yang Mempengaruhi TingkatdewiNo ratings yet
- Jurnal Keperawatan Jiwa Bahasa Inggris 1Document12 pagesJurnal Keperawatan Jiwa Bahasa Inggris 1Fitry WahyuniiNo ratings yet
- Sbar Dialog InggrisDocument1 pageSbar Dialog InggrisMergana Satwika Arini IINo ratings yet
- Role Play HipertensiDocument2 pagesRole Play Hipertensimentari damaiyantiNo ratings yet
- Dilla Aulia - 1811124764Document3 pagesDilla Aulia - 1811124764Dilla AuliaNo ratings yet
- Makalah Bahasa InggrisDocument15 pagesMakalah Bahasa Inggrisfera kartikaNo ratings yet
- 5th Meeting Checking Vital SignsDocument8 pages5th Meeting Checking Vital SignsbanguntrinurhadiNo ratings yet
- Lembar Balik Stroke WNDocument17 pagesLembar Balik Stroke WNriska widianingsihNo ratings yet
- Tugas Kelompok 2 (Symptoms)Document15 pagesTugas Kelompok 2 (Symptoms)Dandy PutraNo ratings yet
- Role Play Kelompok 1 Bahasa Inggris Kelas ADocument6 pagesRole Play Kelompok 1 Bahasa Inggris Kelas Ayandini prafitriNo ratings yet
- Unit 1 - P1337420119335 - Imroatul HDocument6 pagesUnit 1 - P1337420119335 - Imroatul HMar'atus SholihahNo ratings yet
- Soal Bahasa Inggris SMT 3 2017 2018Document7 pagesSoal Bahasa Inggris SMT 3 2017 2018Tuti Alawiyah100% (1)
- SP 7 GDSDocument3 pagesSP 7 GDSMaria Monica0% (1)
- Vital Signs CheckDocument3 pagesVital Signs CheckadenNo ratings yet
- GCS dan REMS dalam Memprediksi Outcome Pasien Trauma KepalaDocument12 pagesGCS dan REMS dalam Memprediksi Outcome Pasien Trauma KepalaSatria Yosi HernawanNo ratings yet
- Tuberculosis Booklet: Causes, Symptoms, TreatmentDocument10 pagesTuberculosis Booklet: Causes, Symptoms, TreatmentSartina LukmanNo ratings yet
- Modul Bahasa Inggris 5Document47 pagesModul Bahasa Inggris 5라라씨lalassi100% (1)
- Dialog 1: Siang, Anna. Bagaimana Keadaan Anda Hari Ini?) Saya Rasa Saya Demam) Anda)Document12 pagesDialog 1: Siang, Anna. Bagaimana Keadaan Anda Hari Ini?) Saya Rasa Saya Demam) Anda)KLINIK ADHYAKSA KEJAKSAAN TINGGI SUMATERA UTARANo ratings yet
- Tugas Bahasa Inggris Wound CareDocument2 pagesTugas Bahasa Inggris Wound CareBela Asa100% (1)
- English Nurfadilah PDFDocument20 pagesEnglish Nurfadilah PDFNurfadillahNo ratings yet
- Skenario Bahasa Inggris Pengkajian Demam TipoidDocument2 pagesSkenario Bahasa Inggris Pengkajian Demam TipoidKharisma FauziyahNo ratings yet
- Jurnal Kesehatan: Terapi Akupresur Menurunkan Tekanan Darah Pasien HipertensiDocument6 pagesJurnal Kesehatan: Terapi Akupresur Menurunkan Tekanan Darah Pasien HipertensiNova RizkenNo ratings yet
- Sap Seks Bebas Sub - IndoDocument14 pagesSap Seks Bebas Sub - IndoSelvia Dwi Permatasari100% (1)
- Form MTBS - Kasus Faduma - Aniq Lutfiyah - I4b019078 PDFDocument4 pagesForm MTBS - Kasus Faduma - Aniq Lutfiyah - I4b019078 PDFAniq LutfiyahNo ratings yet
- Giving Injection &applying InfusionDocument17 pagesGiving Injection &applying InfusionIsmaNo ratings yet
- Slide 4 - Patient Admission Form-1Document9 pagesSlide 4 - Patient Admission Form-1Widyaayu 2507No ratings yet
- TOPIC 10 ASSISTING WITH ELIMINATION Moh Ilham Firdaus (1019031083)Document7 pagesTOPIC 10 ASSISTING WITH ELIMINATION Moh Ilham Firdaus (1019031083)Fadilah Anjar MastrinNo ratings yet
- Admission and Basic Nursing CareDocument26 pagesAdmission and Basic Nursing CareKardana PutraNo ratings yet
- Admitting PatientsDocument12 pagesAdmitting PatientsTommy Aja Ma'InNo ratings yet
- Community AND Family Case Study (CFCS) ReportDocument5 pagesCommunity AND Family Case Study (CFCS) ReportKirbashini KanasanNo ratings yet
- Assessment of Infectious Gastroenteritis PatientsDocument7 pagesAssessment of Infectious Gastroenteritis PatientsmithaNo ratings yet
- Complete The Crossword Puzzle Below: NameDocument2 pagesComplete The Crossword Puzzle Below: NameTmanoj PraveenNo ratings yet
- Informed Consent - Filler - RadiesseDocument7 pagesInformed Consent - Filler - RadiesseAshraf AboNo ratings yet
- Revisiting Structural Family TherapyDocument2 pagesRevisiting Structural Family TherapyKim ScottNo ratings yet
- Delivery Room: Assessment I. ProfileDocument5 pagesDelivery Room: Assessment I. ProfileSofia CartallaNo ratings yet
- Autism Spectrum Disorder Screening Machine Learning Adaptation and DSM 5 Fulfillment PDFDocument6 pagesAutism Spectrum Disorder Screening Machine Learning Adaptation and DSM 5 Fulfillment PDFBudi SantoNo ratings yet
- Chapter 16 Radiation Protection and Safety PDFDocument236 pagesChapter 16 Radiation Protection and Safety PDFAshutosh SinghNo ratings yet
- Radiology 2Document15 pagesRadiology 2Alonso GuardadoNo ratings yet
- Antibiotic Resistance: Bioinformatics-Based Understanding As A Functional Strategy For Drug DesignDocument19 pagesAntibiotic Resistance: Bioinformatics-Based Understanding As A Functional Strategy For Drug DesignBhabani DasNo ratings yet
- QADocument11 pagesQAGladys FernandezNo ratings yet
- Kronmed: Congresul Național Pentru Studenți Și Tineri MediciDocument87 pagesKronmed: Congresul Național Pentru Studenți Și Tineri MediciIubiNo ratings yet
- Memory in AutismDocument384 pagesMemory in AutismkapsicumNo ratings yet
- Basic ECGDocument152 pagesBasic ECGTuấn Thanh VõNo ratings yet
- Nakayama ProcedureDocument6 pagesNakayama ProcedureRosyiidta JanahNo ratings yet
- NS Camp 2012 - Health History Form For HTsDocument1 pageNS Camp 2012 - Health History Form For HTsThanhThao NguyenNo ratings yet
- Modified Release Dosage FormDocument24 pagesModified Release Dosage FormSuraj ChoudharyNo ratings yet
- Sinding Larsen Johansson SyndromeDocument3 pagesSinding Larsen Johansson SyndromeLuis Miguel MartinsNo ratings yet
- MCQ Pharmacology and Pharmacotherapeutics IVDocument13 pagesMCQ Pharmacology and Pharmacotherapeutics IVDr. Anil LandgeNo ratings yet
- Drug Discovery & Development ProcessDocument57 pagesDrug Discovery & Development ProcessHazel Ruth Yara CastilloNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesNursing Care Plan: Assessment Diagnosis Planning Intervention Rationale EvaluationCarolAnneRagpalaGaudiaNo ratings yet
- Endocrine EmergencyDocument24 pagesEndocrine EmergencymalarmathiNo ratings yet
- Otsuka Pharmaceutical v. Torrent Pharmaceuticals Et. Al.Document6 pagesOtsuka Pharmaceutical v. Torrent Pharmaceuticals Et. Al.PriorSmartNo ratings yet
- Intrauterine Growth RestrictionDocument42 pagesIntrauterine Growth RestrictionOgirahma T. NaidNo ratings yet
- VALDEZ, Gail-Marie R. Eaec-3 Yr. Psychiatric Assessment and Mental Status Exam General DataDocument8 pagesVALDEZ, Gail-Marie R. Eaec-3 Yr. Psychiatric Assessment and Mental Status Exam General DatabochoiNo ratings yet
- Pedoman Obat High AlertDocument6 pagesPedoman Obat High AlertErvinaOctavianiNo ratings yet
- Final Solicitation LetterDocument2 pagesFinal Solicitation LetterBrian Jobim TanNo ratings yet
- Care Plan - Ineffective MobilityDocument10 pagesCare Plan - Ineffective MobilityAshley ToppNo ratings yet
- Cover Letter ExampleDocument2 pagesCover Letter ExampleChristina VongNo ratings yet
- Unit 4 Study Guide PathoDocument10 pagesUnit 4 Study Guide Pathoangieswenson100% (1)
- Hematologic Reference Ranges A PDFDocument3 pagesHematologic Reference Ranges A PDFmalaimaxNo ratings yet
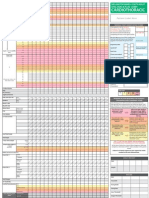
- Adult Early Warning Score Observation Chart For Cardiothoracic UnitDocument1 pageAdult Early Warning Score Observation Chart For Cardiothoracic UnitalexipsNo ratings yet