You might also like
- Defining CharacteristicsDocument2 pagesDefining CharacteristicsAngel MayNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanMariel GamaloNo ratings yet
- Nursing Care Plan for Effective Airway ClearanceDocument5 pagesNursing Care Plan for Effective Airway ClearanceAnnahNo ratings yet
- College of Health Sciences Nursing Care Plan for Acute Myocardial InfarctionDocument4 pagesCollege of Health Sciences Nursing Care Plan for Acute Myocardial InfarctionLouise GudmalinNo ratings yet
- Nursing Care Plan for Fever and DyspneaDocument14 pagesNursing Care Plan for Fever and DyspneaAldwin AyuyangNo ratings yet
- Fatigue Related To Autoimmune Disease As Evidenced by Patient Inability To Maintain Usual Level of Physical ActivityDocument5 pagesFatigue Related To Autoimmune Disease As Evidenced by Patient Inability To Maintain Usual Level of Physical ActivityJordz PlaciNo ratings yet
- Rufino, Leslie Kriztel S. BSN 3-2 Group 1Document6 pagesRufino, Leslie Kriztel S. BSN 3-2 Group 1Deinielle Magdangal RomeroNo ratings yet
- NCP DengueDocument3 pagesNCP DengueNecy Tessa C. AcostaNo ratings yet
- NCP InsomniaDocument2 pagesNCP InsomniaAj MacotoNo ratings yet
- ChestPainReliefDocument3 pagesChestPainReliefCzynna Dela CruzNo ratings yet
- Nursing Care Plan Community Acquired PneumoniaDocument2 pagesNursing Care Plan Community Acquired Pneumoniaderic92% (50)
- NCP DizzinessDocument2 pagesNCP Dizzinesschristine mercadoNo ratings yet
- NCP (Postpartum Hemmorhage)Document3 pagesNCP (Postpartum Hemmorhage)Anne DyNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationVince Adrian FiguracionNo ratings yet
- General Data and Nursing Care Plan for a 1 Month Old Male Patient with PneumoniaDocument10 pagesGeneral Data and Nursing Care Plan for a 1 Month Old Male Patient with PneumoniaOlivelhynn BernaldoNo ratings yet
- NCP ExampleDocument4 pagesNCP ExampleBea Abigail BrocalNo ratings yet
- Case AbstractDocument11 pagesCase AbstractGovernance BookNo ratings yet
- Dino File 2Document6 pagesDino File 2Jhade Danes BalanlayNo ratings yet
- Viray, Messiah Jezreel: NCP #3 For RHDDocument3 pagesViray, Messiah Jezreel: NCP #3 For RHDJezzy VeeNo ratings yet
- Or NCPDocument5 pagesOr NCPjelopigar921No ratings yet
- Clustered Data Nursing Diagnosis (Diagnostic Label) PriorityDocument4 pagesClustered Data Nursing Diagnosis (Diagnostic Label) PriorityRoger ViloNo ratings yet
- Perioperative Nursing Care Plan TAHBSODocument4 pagesPerioperative Nursing Care Plan TAHBSOPatricia OrtegaNo ratings yet
- A Nursing Care Plan Presented To The Faculty of The Nursing DepartmentDocument4 pagesA Nursing Care Plan Presented To The Faculty of The Nursing DepartmentAnge MinguitoNo ratings yet
- HydrocephalusDocument3 pagesHydrocephalusMae Arra Lecobu-anNo ratings yet
- NCP FinalDocument5 pagesNCP FinalVenus BonglayNo ratings yet
- Breast Mass Bilateral To Consider FibroadenomaDocument5 pagesBreast Mass Bilateral To Consider FibroadenomaYum CNo ratings yet
- Nursing Care Plan for BronchospasmDocument5 pagesNursing Care Plan for BronchospasmCG Patron BamboNo ratings yet
- APPENDICITISDocument15 pagesAPPENDICITISTiffany AdriasNo ratings yet
- Saint Paul University Nursing Care PlanDocument5 pagesSaint Paul University Nursing Care PlanCG Patron BamboNo ratings yet
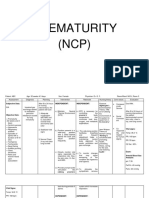
- Prematurity and Lung Surfactant TherapyDocument27 pagesPrematurity and Lung Surfactant TherapyDivine LavaNo ratings yet
- NCP Severe Labor PainDocument3 pagesNCP Severe Labor PainPaolo EspinosaNo ratings yet
- Case Study, Chapter 20, Assessment of Respiratory FunctionDocument11 pagesCase Study, Chapter 20, Assessment of Respiratory FunctionMaddyNo ratings yet
- W2 - MEDSURG Guidelines For Nursing Interventions On Coma PatientsDocument6 pagesW2 - MEDSURG Guidelines For Nursing Interventions On Coma PatientsKyla L. Madjad100% (1)
- Baby G's Fever Nursing Care PlanDocument8 pagesBaby G's Fever Nursing Care Plan2BGrp3Plaza, Anna MaeNo ratings yet
- PERFORMING CPT (Percussion, Vibaration, Postural Drainage)Document5 pagesPERFORMING CPT (Percussion, Vibaration, Postural Drainage)Patricia Feb De Los SantosNo ratings yet
- Nursing assessment and care plan for disturbed sleep patternDocument4 pagesNursing assessment and care plan for disturbed sleep patternArianna Jasmine MabungaNo ratings yet
- Proper Hygiene Prevents Spread of PathogensDocument4 pagesProper Hygiene Prevents Spread of PathogensSheda BondNo ratings yet
- Nursing Care Plan for Labor and DeliveryDocument2 pagesNursing Care Plan for Labor and DeliveryFelmerPolancoRodaNo ratings yet
- Villanueva Bsn-1a - NcplecDocument6 pagesVillanueva Bsn-1a - NcplecKhyra Ysabelle VillanuevaNo ratings yet
- Barrientos Case StudyDocument6 pagesBarrientos Case StudyCalvin Dante BarrientosNo ratings yet
- NCP MakingDocument1 pageNCP MakingRose Camille Delos Santos DatuinNo ratings yet
- NCM 112 Lab (Prelims)Document14 pagesNCM 112 Lab (Prelims)Erica Mei CapiliNo ratings yet
- Basic Life Support: - Presenter Name: - Anna Marie S. QuinonezDocument21 pagesBasic Life Support: - Presenter Name: - Anna Marie S. QuinonezQuinonez Anna MarieNo ratings yet
- The Basics: A Comprehensive Outline of Nursing School ContentFrom EverandThe Basics: A Comprehensive Outline of Nursing School ContentRating: 5 out of 5 stars5/5 (3)
- Apis Mellifica; or, The Poison of the Honey-Bee, Considered as a Therapeutic AgentFrom EverandApis Mellifica; or, The Poison of the Honey-Bee, Considered as a Therapeutic AgentNo ratings yet
- Regaining Bladder Control: For Incontinence on Exertion or Following Pelvic SurgeryFrom EverandRegaining Bladder Control: For Incontinence on Exertion or Following Pelvic SurgeryNo ratings yet
- Reiki For Beginners: The Ultimate Reiki Guide That Teaches You All You Need To Know About Reiki Healing & Improving Your Life With The Power Of Reiki!From EverandReiki For Beginners: The Ultimate Reiki Guide That Teaches You All You Need To Know About Reiki Healing & Improving Your Life With The Power Of Reiki!No ratings yet
- Releasing Cranial/Dural Strains, Eliminating the Mystique: A Simple, Concise, New TechniqueFrom EverandReleasing Cranial/Dural Strains, Eliminating the Mystique: A Simple, Concise, New TechniqueRating: 5 out of 5 stars5/5 (1)
- Floor Plan and Genogram CHNDocument2 pagesFloor Plan and Genogram CHNAnne Ruth OlinNo ratings yet
- 5.70 (H) Mmol/l: Moderate Pain at Lower Right Leg R/T InflammationDocument2 pages5.70 (H) Mmol/l: Moderate Pain at Lower Right Leg R/T InflammationAnne Ruth OlinNo ratings yet
- Concept PaperDocument2 pagesConcept PaperAnne Ruth OlinNo ratings yet
- Bobit and Sandigan Family Initial Data InformationDocument2 pagesBobit and Sandigan Family Initial Data InformationAnne Ruth OlinNo ratings yet
- Bobit and Sandigan Family Initial Data InformationDocument2 pagesBobit and Sandigan Family Initial Data InformationAnne Ruth OlinNo ratings yet
- CP CDX PresentationDocument2 pagesCP CDX PresentationAnne Ruth OlinNo ratings yet
- (St. Paul University System) 680 Pedro Gil St. Malate, ManilaDocument3 pages(St. Paul University System) 680 Pedro Gil St. Malate, ManilaAnne Ruth OlinNo ratings yet
- CP KidneyHTDocument2 pagesCP KidneyHTAnne Ruth OlinNo ratings yet
- Aripiprazole RuthyDocument2 pagesAripiprazole RuthyAnne Ruth OlinNo ratings yet
- Concept PaperDocument2 pagesConcept PaperAnne Ruth OlinNo ratings yet
- Gibbs Er 2Document1 pageGibbs Er 2Anne Ruth OlinNo ratings yet
- Common Illness: Metab MuscleDocument6 pagesCommon Illness: Metab MuscleAnne Ruth OlinNo ratings yet
- CP KidneyHTDocument2 pagesCP KidneyHTAnne Ruth OlinNo ratings yet
- Concept PaperDocument2 pagesConcept PaperAnne Ruth OlinNo ratings yet
- MedicationsDocument1 pageMedicationsAnne Ruth OlinNo ratings yet
- CP KidneyHTDocument2 pagesCP KidneyHTAnne Ruth OlinNo ratings yet
- Acute Renal Failure, Septic Shock, Hospital-Acquired Pneumonia Diagnosis and TreatmentDocument1 pageAcute Renal Failure, Septic Shock, Hospital-Acquired Pneumonia Diagnosis and TreatmentAnne Ruth OlinNo ratings yet
- Emergency MedsDocument12 pagesEmergency MedsAnne Ruth OlinNo ratings yet
- OpemrazoleDocument2 pagesOpemrazoleAnne Ruth OlinNo ratings yet
- Picos2 .0Document5 pagesPicos2 .0Anne Ruth OlinNo ratings yet
- OpemrazoleDocument2 pagesOpemrazoleAnne Ruth OlinNo ratings yet
- Drug Name and Dose Classification Mechanism of Action Indication Adverse Reaction/ Side Effects NSG ResponsibilityDocument6 pagesDrug Name and Dose Classification Mechanism of Action Indication Adverse Reaction/ Side Effects NSG ResponsibilityAnne Ruth OlinNo ratings yet
- NCP JjoDocument7 pagesNCP JjoAnne Ruth OlinNo ratings yet
- Mental Status Examination MS. MelsDocument3 pagesMental Status Examination MS. MelsAnne Ruth OlinNo ratings yet
- AbilifyDocument5 pagesAbilifyMary Grace Rivera Incillo-IbaanNo ratings yet
- Common Illness: Metab MuscleDocument6 pagesCommon Illness: Metab MuscleAnne Ruth OlinNo ratings yet
- OpemrazoleDocument2 pagesOpemrazoleAnne Ruth OlinNo ratings yet
- Case of OsteosarcomaDocument25 pagesCase of Osteosarcomadocs2009100% (3)
- Priorotization OsteoDocument1 pagePriorotization OsteoHannah Milca OlinNo ratings yet
- 7.nuclear Chemistry and Environmental Chemistry ExerciseDocument38 pages7.nuclear Chemistry and Environmental Chemistry ExerciseYogy YNo ratings yet
- Journey by Night EssayDocument2 pagesJourney by Night Essaystillwakingsleep100% (2)
- Translation of The Original Operating Manual: Epg-Sprint XeDocument100 pagesTranslation of The Original Operating Manual: Epg-Sprint XePatricio Exequiel Silva ColileoNo ratings yet
- Calculation of The Reorder Point For Items With Exponential and Poisson Distribution of Lead Time DemandDocument10 pagesCalculation of The Reorder Point For Items With Exponential and Poisson Distribution of Lead Time DemandRaj ChauhanNo ratings yet
- Soft Skills in The Pharmacy Curriculum: Lilian M. AzzopardiDocument14 pagesSoft Skills in The Pharmacy Curriculum: Lilian M. Azzopardishailendra patilNo ratings yet
- Performance Checklist On Cranial Nerve AssessmentDocument3 pagesPerformance Checklist On Cranial Nerve AssessmentSolsona Natl HS Maananteng100% (1)
- Pest Management Practices of Farmers in PambujanDocument13 pagesPest Management Practices of Farmers in PambujanLucille MoralesNo ratings yet
- GOVT - Departments - Contact - Details - MF-14-06-2021 UpdatedDocument32 pagesGOVT - Departments - Contact - Details - MF-14-06-2021 Updatedadf_raghuNo ratings yet
- Benefits and Limitations of GSTDocument7 pagesBenefits and Limitations of GSTGovernment Ramanarayan chellaram collageNo ratings yet
- ALKANES Quiz SheetDocument5 pagesALKANES Quiz Sheetnajifaahmed223No ratings yet
- Trail/Beaver Valley/Rossland Apr. 9, 2019Document39 pagesTrail/Beaver Valley/Rossland Apr. 9, 2019Pennywise PublishingNo ratings yet
- KT 470Document4 pagesKT 470Fabian PzvNo ratings yet
- Drilling Fluid Processing System BrochureDocument20 pagesDrilling Fluid Processing System BrochureazkNo ratings yet
- A Simple and Rapid Method For Colorimetric Determination of Histamine in Fish FleshDocument8 pagesA Simple and Rapid Method For Colorimetric Determination of Histamine in Fish Fleshmuratout3447No ratings yet
- AMAZEN Manual ForWebONLY 2 5 19 PDFDocument13 pagesAMAZEN Manual ForWebONLY 2 5 19 PDFkg27r-scribd9325100% (1)
- Surat Sponsorship Merck (Iliadin)Document1 pageSurat Sponsorship Merck (Iliadin)goblok goblokinNo ratings yet
- Prof Ed6 Intro To MetacognitionDocument83 pagesProf Ed6 Intro To MetacognitionRishane Lolo ListanaNo ratings yet
- JnaDocument34 pagesJnaDeepak KumarNo ratings yet
- Presented by M. Hassan ShafiqDocument25 pagesPresented by M. Hassan ShafiqMadiha Amna AndrabiNo ratings yet
- SAFETY DATA SHEET TECSEL ADHESIVE - Rev 01Document7 pagesSAFETY DATA SHEET TECSEL ADHESIVE - Rev 01Dairo GomezNo ratings yet
- LogDocument12 pagesLogrifaniagustinNo ratings yet
- Caldwell Schizophrenizing LacanDocument10 pagesCaldwell Schizophrenizing LacanaxisofelvisNo ratings yet
- Molykote: 111 CompoundDocument2 pagesMolykote: 111 CompoundEcosuministros ColombiaNo ratings yet
- Pulseless Arrest Algorithm For Managing AsystoleDocument1 pagePulseless Arrest Algorithm For Managing AsystoleLady MuffinsNo ratings yet
- Long Test MILDocument3 pagesLong Test MILBern PabNo ratings yet
- Analiza PESTDocument16 pagesAnaliza PESTIoana Ciobanu100% (1)
- VACCINATION LISTDocument2 pagesVACCINATION LISTRakesh KumarNo ratings yet
- Electrometallurgy NptelDocument23 pagesElectrometallurgy NptelChayon MondalNo ratings yet
- Reviewer Ansc 111Document6 pagesReviewer Ansc 111Jeric MadroñoNo ratings yet
- Math ProjectDocument18 pagesMath ProjectChar LotteNo ratings yet