You might also like
- Mtap - BacteriologyDocument11 pagesMtap - BacteriologyMoira Pauline LibroraniaNo ratings yet
- Clinical Chemistry 2 Lecture Notes in Trace ElementsDocument6 pagesClinical Chemistry 2 Lecture Notes in Trace ElementsMoira Pauline LibroraniaNo ratings yet
- Mtap - Bacteriology FinalsDocument6 pagesMtap - Bacteriology FinalsMoira Pauline LibroraniaNo ratings yet
- Smallest Viruses (The Only Dna Virus To Have Ssdna) .: Parvovirus B19Document8 pagesSmallest Viruses (The Only Dna Virus To Have Ssdna) .: Parvovirus B19AfreenNo ratings yet
- 5M Urea Test - Factor XIII DeficiencyDocument4 pages5M Urea Test - Factor XIII DeficiencyJohn TamayoNo ratings yet
- Midterm ParasitologyDocument18 pagesMidterm ParasitologyAngelic AngelesNo ratings yet
- Platelet Storage Pool Disorders PDFDocument4 pagesPlatelet Storage Pool Disorders PDFMano CempakaNo ratings yet
- Immuno-Serology & Blood Banking Case StudyDocument8 pagesImmuno-Serology & Blood Banking Case StudyRomie SolacitoNo ratings yet
- MUST To KNOW in Hematology1-1Document45 pagesMUST To KNOW in Hematology1-1Jez Mendoza ManuelNo ratings yet
- Blood Bank (2 Week) : Antibody ScreensDocument5 pagesBlood Bank (2 Week) : Antibody ScreensAngela ReyesNo ratings yet
- MictobiologyDocument26 pagesMictobiologySaransh GhimireNo ratings yet
- DermatophytesDocument1 pageDermatophytesKoo ThaNo ratings yet
- Lec 1 - IntroductionDocument3 pagesLec 1 - IntroductionHaendra Mae DapilagaNo ratings yet
- Histopathology Review BookletDocument21 pagesHistopathology Review BookletMarie Llanes100% (1)
- Bacte Day 2Document24 pagesBacte Day 2Jadey InfanteNo ratings yet
- 4th Shifting Micro Lab ReviewerDocument154 pages4th Shifting Micro Lab ReviewerJade MonrealNo ratings yet
- Disorders of Iron Kinetics and Heme MetabolismDocument12 pagesDisorders of Iron Kinetics and Heme MetabolismJoanne JardinNo ratings yet
- Virology LectureDocument16 pagesVirology LectureJuan UmiwasNo ratings yet
- Microbiology 2Document53 pagesMicrobiology 2pikachuNo ratings yet
- Incorrectly: CorrectlyDocument25 pagesIncorrectly: CorrectlypikachuNo ratings yet
- Drummelsmith - Laboratory Diagnosis and Bacterial Identification - Study GuideDocument19 pagesDrummelsmith - Laboratory Diagnosis and Bacterial Identification - Study GuideTom TsouNo ratings yet
- Staphylococcus Spp. Gram Positive. ClusteredDocument15 pagesStaphylococcus Spp. Gram Positive. ClusteredIvy NNo ratings yet
- Nematodes: 2. Enterobius VermicularisDocument2 pagesNematodes: 2. Enterobius VermicularisCia QuebecNo ratings yet
- IMHM321 Lecture Trans 3Document9 pagesIMHM321 Lecture Trans 3Brix BrixNo ratings yet
- MycobacteriumDocument11 pagesMycobacteriumskNo ratings yet
- Immunohematology & Blood Bank: Alyazeed Hussein, BSCDocument58 pagesImmunohematology & Blood Bank: Alyazeed Hussein, BSCVijay KumarNo ratings yet
- Hematology PictureDocument77 pagesHematology Pictureapi-3707883100% (6)
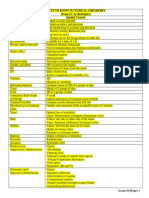
- MUST To KNOW in Clinical ChemistryDocument53 pagesMUST To KNOW in Clinical ChemistryTristan Jay CalabiaNo ratings yet
- 5.Rh Blood Group SystemDocument22 pages5.Rh Blood Group Systemjong188No ratings yet
- Sir Alvin Rey Flores: Echinococcus Granulosus, Taenia Solium)Document5 pagesSir Alvin Rey Flores: Echinococcus Granulosus, Taenia Solium)Corin LimNo ratings yet
- Clinical Chemistry IDocument8 pagesClinical Chemistry IMariel AbatayoNo ratings yet
- CELL OVERVIEW PREVENTION Notes 2015Document7 pagesCELL OVERVIEW PREVENTION Notes 2015Alexander LukashenkoNo ratings yet
- Myxoviruses: MIDTERM LESSON 2: Respiratory VirusesDocument8 pagesMyxoviruses: MIDTERM LESSON 2: Respiratory VirusesAnya IgnacioNo ratings yet
- MycoViro 2Document44 pagesMycoViro 2Ria AlcantaraNo ratings yet
- Parasitology Review NotesDocument27 pagesParasitology Review NotesMarie LlanesNo ratings yet
- CampylobacterDocument2 pagesCampylobactersarguss14No ratings yet
- Histopathologic & Cytologic TechniquesDocument171 pagesHistopathologic & Cytologic TechniquesMHEKAELLA SAMSONNo ratings yet
- Immunohematology/ Blood BankingDocument2 pagesImmunohematology/ Blood BankingSophia AmpatuanNo ratings yet
- Harrisons: Introduction To Infectious DiseasesDocument3 pagesHarrisons: Introduction To Infectious Diseasesapi-3704562No ratings yet
- Microbiology - ParasitologyDocument34 pagesMicrobiology - ParasitologySasi DharanNo ratings yet
- SPMC - Microbiology Case StudyDocument9 pagesSPMC - Microbiology Case StudyRomie SolacitoNo ratings yet
- MV Lec PDFDocument102 pagesMV Lec PDFJonas Datu100% (1)
- Virology - S1: Abbas Adel Group 4Document38 pagesVirology - S1: Abbas Adel Group 4William BufNo ratings yet
- HemaDocument59 pagesHemaSteph VeeNo ratings yet
- Molecular Diagnosis in HaematologyDocument23 pagesMolecular Diagnosis in HaematologyUmar'Farouq Oni100% (1)
- Chapter 25 - Extrinsic Defects Leading To Increased Erythrocyte Destruction - Immune Causes Final DraftDocument2 pagesChapter 25 - Extrinsic Defects Leading To Increased Erythrocyte Destruction - Immune Causes Final DraftNathaniel SimNo ratings yet
- Hematology: Dr. I. Quirt Adriana Cipolletti, Jeremy Gilbert and Susy Hota, Chapter Editors Leora Horn, Associate EditorDocument42 pagesHematology: Dr. I. Quirt Adriana Cipolletti, Jeremy Gilbert and Susy Hota, Chapter Editors Leora Horn, Associate EditorRubyrose Tagum100% (1)
- ISBB Aaaaa PDFDocument55 pagesISBB Aaaaa PDFSelena de LimaNo ratings yet
- Mycology: Rochelle D. Darlucio-Yabut, RMT, MPH Our Lady of Fatima University College of Medical Laboratory ScienceDocument59 pagesMycology: Rochelle D. Darlucio-Yabut, RMT, MPH Our Lady of Fatima University College of Medical Laboratory ScienceClaire GonoNo ratings yet
- Immuno SeroDocument80 pagesImmuno SeroDocAxi Maximo Jr AxibalNo ratings yet
- ENZYMOLOGYDocument2 pagesENZYMOLOGYCarla Lagar FloresNo ratings yet
- Test Bank Exam 3Document81 pagesTest Bank Exam 3Sajjad AhmadNo ratings yet
- Intro To Virology ReviewerDocument14 pagesIntro To Virology ReviewerJilianne Sablot100% (1)
- Clinical Microbiology 2Document20 pagesClinical Microbiology 2phuong mai leNo ratings yet
- Serologic Tests Part 1Document4 pagesSerologic Tests Part 1Joshua TrinidadNo ratings yet
- Component Therapy-Transfusion of TheDocument8 pagesComponent Therapy-Transfusion of TheGennelyn Ross Delos ReyesNo ratings yet
- CLS 400 - Test 4 (Extra Credit)Document8 pagesCLS 400 - Test 4 (Extra Credit)McNeeseInsiderNo ratings yet
- WA10015-Immune Response HIV PDFDocument1 pageWA10015-Immune Response HIV PDFLianceNo ratings yet
- Micro Introduction Normal Flora Nosocomial InfectionsDocument6 pagesMicro Introduction Normal Flora Nosocomial InfectionsPatricia Mae de JesusNo ratings yet
- MICRO GramPosBacilliMD2021Document4 pagesMICRO GramPosBacilliMD2021Patricia Mae de JesusNo ratings yet
- Micro Culture Media MD2021Document4 pagesMicro Culture Media MD2021Patricia Mae de JesusNo ratings yet
- Microbiology: Nocardia, Actinomyces, Haemophilus and BordetellaDocument3 pagesMicrobiology: Nocardia, Actinomyces, Haemophilus and BordetellaPatricia Mae de JesusNo ratings yet
- Micro - Bacterial Growth and Nutrition MD2021Document2 pagesMicro - Bacterial Growth and Nutrition MD2021Patricia Mae de JesusNo ratings yet
- Microbiology: Atypical Bacteria: Chlamydia, Mycoplasms, LegionellaDocument4 pagesMicrobiology: Atypical Bacteria: Chlamydia, Mycoplasms, LegionellaPatricia Mae de JesusNo ratings yet
- VIROLOGY HerpesviridaeDocument4 pagesVIROLOGY HerpesviridaePatricia Mae de JesusNo ratings yet
- Baby Katzung Case 1 10Document15 pagesBaby Katzung Case 1 10Danielle Sabrina LimNo ratings yet
- Special Collection ProceduresDocument6 pagesSpecial Collection ProceduresB12 Clifford GarciaNo ratings yet
- Heredity (Inheritance and Variation)Document3 pagesHeredity (Inheritance and Variation)Jazel SalesNo ratings yet
- 0-CNS MCQ's FileDocument46 pages0-CNS MCQ's Fileahmed mahamedNo ratings yet
- Microbial Toxins PDFDocument11 pagesMicrobial Toxins PDFAnonymous OPix6Tyk5INo ratings yet
- Cell Cycle-1Document6 pagesCell Cycle-1lorenoh21No ratings yet
- ABO Antibody TiterDocument21 pagesABO Antibody TiterRash PaltepNo ratings yet
- Solutions For All Your Gaseous Chlorine Dioxide Needs The Chlorine Dioxide PeopleDocument7 pagesSolutions For All Your Gaseous Chlorine Dioxide Needs The Chlorine Dioxide PeopleJesús GINo ratings yet
- MOYA, John Zeus A. (HUMANA Classwork #3 Prelim)Document41 pagesMOYA, John Zeus A. (HUMANA Classwork #3 Prelim)Suez AyomNo ratings yet
- Bioline Rapid. Urinalysis TestDocument34 pagesBioline Rapid. Urinalysis Testvan luomNo ratings yet
- Kemu A & P 3Document9 pagesKemu A & P 3malenya1No ratings yet
- mebendazole-WPS OfficeDocument6 pagesmebendazole-WPS OfficeDenvicNo ratings yet
- Med 9780190862800 Chapter 59Document8 pagesMed 9780190862800 Chapter 59ntnquynhproNo ratings yet
- Chapter 17Document15 pagesChapter 17nfnf otupyooorefnNo ratings yet
- Diseases ListDocument49 pagesDiseases ListChandra Sekhar GajulaNo ratings yet
- Abernathy 1Document2 pagesAbernathy 1api-316558435No ratings yet
- MSC Genetics SyllabusDocument36 pagesMSC Genetics SyllabusMohak SahuNo ratings yet
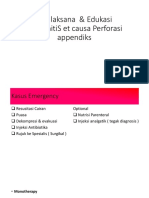
- Tatalaksana PeritonitisDocument7 pagesTatalaksana PeritonitisDavinWijayaNo ratings yet
- Essentials of Genetics 8th Edition by Klug Cummings Spencer and Palladino ISBN Test BankDocument14 pagesEssentials of Genetics 8th Edition by Klug Cummings Spencer and Palladino ISBN Test Banklester100% (24)
- ASO Article - GCDocument5 pagesASO Article - GCHaseena SaitNo ratings yet
- Pharma - SkinDocument8 pagesPharma - Skinreference books100% (1)
- Prevalence and Characterization of Shiga Toxin O157 H7 and Non O157 H7 Enterohemorrhagic Escherichia Coli Isolated From Different SourcesDocument10 pagesPrevalence and Characterization of Shiga Toxin O157 H7 and Non O157 H7 Enterohemorrhagic Escherichia Coli Isolated From Different SourcesSABA YOUNASNo ratings yet
- Mycobacterial Granulomas, Opportunistic Granulomas and Other Bacterial DiseasesDocument25 pagesMycobacterial Granulomas, Opportunistic Granulomas and Other Bacterial DiseasesBiancaNo ratings yet
- Immunology (Final) Laden SalehDocument193 pagesImmunology (Final) Laden SalehLaden SalehNo ratings yet
- MCQ in Microbiology - NoCopy-1Document23 pagesMCQ in Microbiology - NoCopy-1sharad sawantNo ratings yet
- Antibody Structure and Functions in Humoral ImmunityDocument30 pagesAntibody Structure and Functions in Humoral Immunitymohammed agungNo ratings yet
- Lecture 3 The Nervous SystemDocument11 pagesLecture 3 The Nervous SystemJanvi MehtaNo ratings yet
- Xpert HCV Viral Load ENGLISH Package Insert 301-3019 Rev BDocument24 pagesXpert HCV Viral Load ENGLISH Package Insert 301-3019 Rev BAye MaNo ratings yet
- Introduction To Proteomics and Genomics: Asma Asif FA17-BSI-002 DR IbrahimDocument3 pagesIntroduction To Proteomics and Genomics: Asma Asif FA17-BSI-002 DR IbrahimMuhammad Faizan AsifNo ratings yet
- 5.3 Neuronal Communication POWERPOINTDocument58 pages5.3 Neuronal Communication POWERPOINTLisa MillardNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (23)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)