You might also like
- Gut and Psychology Syndrome: Natural Treatment for Autism, Dyspraxia, A.D.D., Dyslexia, A.D.H.D., Depression, Schizophrenia, 2nd EditionFrom EverandGut and Psychology Syndrome: Natural Treatment for Autism, Dyspraxia, A.D.D., Dyslexia, A.D.H.D., Depression, Schizophrenia, 2nd EditionRating: 4 out of 5 stars4/5 (38)
- Chargaff DNA Data GraphingDocument2 pagesChargaff DNA Data GraphingMarie NdulueNo ratings yet
- The Fugate FamilyDocument7 pagesThe Fugate Familycaleb19941830No ratings yet
- Cell Biology LaboratoryDocument319 pagesCell Biology LaboratoryNazaqat FarooqNo ratings yet
- Dna StructureDocument23 pagesDna Structureapi-315792432No ratings yet
- Genetics & Genomics in Pediatric Primary CareDocument55 pagesGenetics & Genomics in Pediatric Primary CareAda AzotamNo ratings yet
- Uworld RationalesDocument2 pagesUworld RationalesMelissa Sapp67% (3)
- (S. Abbate) Ear Acupuncture Prescriptions and Techniques PDFDocument8 pages(S. Abbate) Ear Acupuncture Prescriptions and Techniques PDFVenom VerdinNo ratings yet
- Authentic Assessment (Genetics)Document2 pagesAuthentic Assessment (Genetics)Raquel Lizardo100% (2)
- Lesson 26 - Light Reactions of Photosynthesis OnDocument49 pagesLesson 26 - Light Reactions of Photosynthesis OnKamto EzenwamaduNo ratings yet
- Meiosis SimulationDocument6 pagesMeiosis SimulationLittle Ar-RaziNo ratings yet
- Karyotype Lab: Objective: Students Will Interpret Karyotypes To Determine The Gender of Individuals and Whether TheyDocument7 pagesKaryotype Lab: Objective: Students Will Interpret Karyotypes To Determine The Gender of Individuals and Whether Theyjeannine limoli100% (1)
- Fungi 1 RhizopusDocument1 pageFungi 1 RhizopusJeremy EvansNo ratings yet
- Genetics WorksheetsDocument3 pagesGenetics WorksheetsJohn ferdinand TamayoNo ratings yet
- CC11 12.16.20 Frosty The Snowman Genetics Activity Page FILLABLEDocument3 pagesCC11 12.16.20 Frosty The Snowman Genetics Activity Page FILLABLEHanifa Ong33% (3)
- Modeling The Cell Cycle and MitosisDocument4 pagesModeling The Cell Cycle and MitosisFroilan Mae Olado CahaponNo ratings yet
- Evidence of Evolution Choice BoardDocument1 pageEvidence of Evolution Choice Boardapi-534241952100% (1)
- Topic Outline MicroDocument3 pagesTopic Outline MicroBrent Louisse GuinitaNo ratings yet
- Micro-Organisms: LO: To Know What A Micro-Organism IsDocument13 pagesMicro-Organisms: LO: To Know What A Micro-Organism IsMy Eyes Are on YOUNo ratings yet
- A Definition of Bioethics, and Some of The Issues Generally InvolvedDocument3 pagesA Definition of Bioethics, and Some of The Issues Generally InvolvedMichael BoutsalisNo ratings yet
- Diffusion Osmosis Lab 2Document3 pagesDiffusion Osmosis Lab 2briangkentNo ratings yet
- Karyotype Stations JL 2019Document8 pagesKaryotype Stations JL 2019jeannine limoli100% (1)
- Evolution: Evidence in Fossil RecordsDocument10 pagesEvolution: Evidence in Fossil RecordsAlexa Cuevas100% (1)
- Gay Adoption - Research PaperDocument7 pagesGay Adoption - Research PaperIesha ClarkNo ratings yet
- Cell Bio Lab ManualDocument53 pagesCell Bio Lab ManualAdil Anwar100% (2)
- Egg Osmosis LabDocument2 pagesEgg Osmosis Labapi-391540671No ratings yet
- Effect of Salinity On Seed Germination, Growth and Organic Compounds of Mungbean Plant Vigna RadiataDocument10 pagesEffect of Salinity On Seed Germination, Growth and Organic Compounds of Mungbean Plant Vigna RadiatahunarsandhuNo ratings yet
- Yap vs. People (Full Text, Word Version)Document14 pagesYap vs. People (Full Text, Word Version)Emir MendozaNo ratings yet
- Bio1 - Unit 1 LectureDocument7 pagesBio1 - Unit 1 LectureCarlo Joseph MoskitoNo ratings yet
- Lecture-1, Introductio To MicrobiologyDocument35 pagesLecture-1, Introductio To MicrobiologyWaleed 1100% (1)
- EthicsDocument77 pagesEthicsAce Visuals100% (2)
- How Do Genes Affect AddictionDocument7 pagesHow Do Genes Affect AddictionIvy Maril De GuzmanNo ratings yet
- Ethics - Morality Is Not Relative - James Rachels LectureDocument17 pagesEthics - Morality Is Not Relative - James Rachels Lectureapi-278252759No ratings yet
- What Is DrugDocument9 pagesWhat Is DrugFebz CanutabNo ratings yet
- The Advantages & Disadvantages of Using Biological Weapons For TerrorismDocument6 pagesThe Advantages & Disadvantages of Using Biological Weapons For TerrorismChenideNo ratings yet
- Systemic Lupus ErythematosusDocument9 pagesSystemic Lupus ErythematosusElma GonzalesNo ratings yet
- Evolution of The Peppered MothDocument3 pagesEvolution of The Peppered MothSayed MikoNo ratings yet
- Lesson Plan Genetics: Fun With Punnett Squares: Angela SchultzDocument2 pagesLesson Plan Genetics: Fun With Punnett Squares: Angela SchultzAnne ButaslacNo ratings yet
- Genetics Unit OutlineDocument44 pagesGenetics Unit Outlineapi-28375664050% (2)
- Lesson 1 Introduction To Bacteriology History Taxonomy and Bacterial Structure ModuleDocument16 pagesLesson 1 Introduction To Bacteriology History Taxonomy and Bacterial Structure ModuleTinNo ratings yet
- Maple Syrup Urine DiseaseDocument4 pagesMaple Syrup Urine DiseaseDemetrio Mark Dela CernaNo ratings yet
- Lifespan Psych. Middy 1 Review-2Document10 pagesLifespan Psych. Middy 1 Review-2Anonymous l8Q2fJNo ratings yet
- This Lesson Will Increase Your Knowledge of Concepts Covered in The Following TEKS For BiologyDocument51 pagesThis Lesson Will Increase Your Knowledge of Concepts Covered in The Following TEKS For BiologyVaibhav KaroliyaNo ratings yet
- Bioethics SalamanesDocument2 pagesBioethics SalamanesShiella Mae SalamanesNo ratings yet
- Human Cloning: Designer BabiesDocument13 pagesHuman Cloning: Designer BabiesYou TubeNo ratings yet
- Agent Orange EpigeneticsDocument3 pagesAgent Orange EpigeneticsChildren Of Vietnam Veterans Health AllianceNo ratings yet
- LUCASSEN 2005. Families & Genetic Testing - The Case of Jane & PhyllisDocument20 pagesLUCASSEN 2005. Families & Genetic Testing - The Case of Jane & PhyllisManuel Dnte JosueNo ratings yet
- Bioethics NotesDocument11 pagesBioethics NotesDD97No ratings yet
- Organelle Card SortDocument37 pagesOrganelle Card SorttashuaneesNo ratings yet
- Genetics & Health: Alka Mishra M. Sc. Nursing 1 YearDocument63 pagesGenetics & Health: Alka Mishra M. Sc. Nursing 1 Yearpandem soniyaNo ratings yet
- Ethics in Abnormal PregnanciesDocument123 pagesEthics in Abnormal PregnanciesspicylaingNo ratings yet
- Genetic DisordersDocument26 pagesGenetic DisordersFatima SuarezNo ratings yet
- Why Fathers Really MatterDocument6 pagesWhy Fathers Really MatterTikvahNo ratings yet
- Genetic TestingDocument50 pagesGenetic TestingAshly NygilNo ratings yet
- Suaybaguio Lyndee Ann - A&D - Module 3Document15 pagesSuaybaguio Lyndee Ann - A&D - Module 3Lyndee Ann SuaybaguioNo ratings yet
- By: Suriya & Nur FatinDocument22 pagesBy: Suriya & Nur FatinSue Asyriya AsyNo ratings yet
- Chapter 4 Outline: IntroDocument9 pagesChapter 4 Outline: IntroJen BriegelNo ratings yet
- Course Unit 2 Week5Document6 pagesCourse Unit 2 Week5Big DaddyNo ratings yet
- OB (Midterms Reviewer)Document19 pagesOB (Midterms Reviewer)JULIANO, GRACHELLE A.No ratings yet
- Module 4-Ethical Issues in Genetic TestingDocument65 pagesModule 4-Ethical Issues in Genetic Testingstlcajun55No ratings yet
- List of The Advantages of Sexual ReproductionDocument10 pagesList of The Advantages of Sexual ReproductionJhonrey Kurt Buenavista AreolaNo ratings yet
- Anupama Ra NotesDocument23 pagesAnupama Ra NotesShahzeel Iftikhar100% (1)
- Direct Black 22Document4 pagesDirect Black 22DHRUVNo ratings yet
- Complete Holistic Guide To Working Out in The GymDocument218 pagesComplete Holistic Guide To Working Out in The Gympsichi21No ratings yet
- Policy That Implemented in Kota SamarahanDocument9 pagesPolicy That Implemented in Kota SamarahanIskandar IskandarNo ratings yet
- Lesson VI: Semi-Solid Dosage Form of PreparationsDocument27 pagesLesson VI: Semi-Solid Dosage Form of PreparationsEleanorNo ratings yet
- Acetic AnhydrideDocument8 pagesAcetic AnhydrideAsyraf SabriNo ratings yet
- Neurobic Excersise Impact On Cognative FunctionDocument8 pagesNeurobic Excersise Impact On Cognative FunctionZalinah Mohd YusofNo ratings yet
- A Synopsis On: Consumer's Perception Towards Packaged Cold-Pressed Juices and Brand " PVT LTDDocument3 pagesA Synopsis On: Consumer's Perception Towards Packaged Cold-Pressed Juices and Brand " PVT LTDNationalinstituteDsnrNo ratings yet
- Subject: PsychopharmacologyDocument11 pagesSubject: PsychopharmacologyAli IjazNo ratings yet
- Feline Injection-Site Sarcoma - Todays Veterinary PracticeDocument12 pagesFeline Injection-Site Sarcoma - Todays Veterinary PracticeBla bla BlaNo ratings yet
- Budget of Works in Grade 7 Health: S.Y. 2019 - 2020 Quarter Topics Objectives Activites No. of HoursDocument1 pageBudget of Works in Grade 7 Health: S.Y. 2019 - 2020 Quarter Topics Objectives Activites No. of HoursRichard MarquezNo ratings yet
- Test Bank For Mosbys Essentials For Nursing Assistants 4th Edition SorrentinoDocument24 pagesTest Bank For Mosbys Essentials For Nursing Assistants 4th Edition Sorrentinozacharymcleanpdqogjyfeb100% (47)
- Science3 Q1 W4 Proper Use HandlingDocument50 pagesScience3 Q1 W4 Proper Use HandlingGina Contalba TubeoNo ratings yet
- Complete Guide To Communication Problems After StrokeDocument22 pagesComplete Guide To Communication Problems After Strokeapi-215453798100% (1)
- Whitesboro Isd - 1995 TEXAS SCHOOL SURVEY OF DRUG AND ALCOHOL USEDocument6 pagesWhitesboro Isd - 1995 TEXAS SCHOOL SURVEY OF DRUG AND ALCOHOL USETexas School Survey of Drug and Alcohol UseNo ratings yet
- Definitions of Human SecurityDocument10 pagesDefinitions of Human SecurityClandestain Zee100% (2)
- Manual Handling DefinitionDocument2 pagesManual Handling DefinitionRaj KumarNo ratings yet
- Chapter 01Document22 pagesChapter 01kita5437100% (1)
- Bus Man Unit 3 SAC 3Document13 pagesBus Man Unit 3 SAC 3Mohamad ZackuanNo ratings yet
- Alice in Michigan: A Financial Hardship StudyDocument58 pagesAlice in Michigan: A Financial Hardship StudydaneNo ratings yet
- Common Skin Diseases in Africa: An Illustrated GuideDocument85 pagesCommon Skin Diseases in Africa: An Illustrated GuideJohn EnioladeNo ratings yet
- Cases HBSDocument40 pagesCases HBStoluene_bomb33% (9)
- Basics of Therapeutic DietsDocument12 pagesBasics of Therapeutic DietstiruchanurNo ratings yet
- 28 CryptorchidismDocument23 pages28 CryptorchidismFaisal Ibn MushtaqNo ratings yet
- Norma Ashrae 62 1989Document3 pagesNorma Ashrae 62 1989Mittzi CallejasNo ratings yet
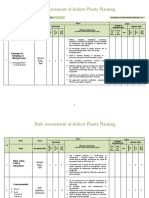
- Risk Assessment of Indoor Plants PlantingDocument5 pagesRisk Assessment of Indoor Plants Plantingطارق رضوانNo ratings yet
- Hemodynamic MonitoringDocument35 pagesHemodynamic MonitoringWiz SamNo ratings yet
- Jawad Et Al - 2021 - Implications of Armed Conflict For Maternal and Child HealthDocument18 pagesJawad Et Al - 2021 - Implications of Armed Conflict For Maternal and Child HealthIvan OliveiraNo ratings yet