You might also like
- Advanced Nutritional BiochemistryDocument90 pagesAdvanced Nutritional BiochemistryAkinleye peter100% (1)
- AP-Food List TPCM PDFDocument12 pagesAP-Food List TPCM PDFS K ChughNo ratings yet
- What Are LipoproteinsDocument18 pagesWhat Are Lipoproteinsarsal1cheema-88705No ratings yet
- Mcqs of Family LawDocument24 pagesMcqs of Family LawVenugopal Mantraratnam32% (19)
- Disorders of The Alimentary TractDocument25 pagesDisorders of The Alimentary Tract수안현100% (1)
- 1.a Superior Orbital Fissure SyndromeDocument2 pages1.a Superior Orbital Fissure SyndromeDr Sumant SharmaNo ratings yet
- FructoseDocument23 pagesFructoseManish TiwariNo ratings yet
- Uveit FosterDocument954 pagesUveit FosterEdmond IsufajNo ratings yet
- Biochemistry QuizDocument28 pagesBiochemistry Quizsanjviews100% (3)
- Md2024 Physio SamplexDocument11 pagesMd2024 Physio SamplexSHAN-SHAN CHANGNo ratings yet
- Correlation Between Strabismus and AmblyophiaDocument17 pagesCorrelation Between Strabismus and AmblyophiaAyu W. AnggreniNo ratings yet
- Life Wealth Mastery EnglishDocument12 pagesLife Wealth Mastery EnglishD.j. Ralmm100% (1)
- Joule Gym Marketing Plan for Female-Only Fitness CenterDocument23 pagesJoule Gym Marketing Plan for Female-Only Fitness CenterJeremy BadalNo ratings yet
- Hematology & Lymphoid System Study Guide - Y1 2025Document43 pagesHematology & Lymphoid System Study Guide - Y1 2025Wahaj Mujahid100% (1)
- Mineral MetabolismDocument24 pagesMineral Metabolismyasarc365No ratings yet
- 7 - Regulation and Functions of The Thyroid HormonesDocument31 pages7 - Regulation and Functions of The Thyroid HormonesVigneshwaran RavishankarNo ratings yet
- Surgery MCQ KEY: Surgery Paper MCQ’s along with KEYDocument8 pagesSurgery MCQ KEY: Surgery Paper MCQ’s along with KEYSiraj Ul IslamNo ratings yet
- Chapter 18 Endocrine SystemDocument40 pagesChapter 18 Endocrine SystemlolasparkleNo ratings yet
- Digestive SystemDocument11 pagesDigestive SystemDanesa MadoNo ratings yet
- Cholesterol and Lipoprotein MetabolismDocument32 pagesCholesterol and Lipoprotein MetabolismBenjamin PrabhuNo ratings yet
- Comparsion of Lipid Profile in Diabetic Hypertensives VS Diabetic NormotensivesDocument8 pagesComparsion of Lipid Profile in Diabetic Hypertensives VS Diabetic NormotensivesIJAR JOURNALNo ratings yet
- Renal Computation AssessmentDocument7 pagesRenal Computation AssessmentKathlene GamitNo ratings yet
- Determining Glucose Concentration and Glucose Oxidase SpecificityDocument20 pagesDetermining Glucose Concentration and Glucose Oxidase Specificitymujuni emanuelNo ratings yet
- Fight or Flight Response En-UsDocument1 pageFight or Flight Response En-Ussusie cabrillanaNo ratings yet
- A. Ground Nut Oil B. Palm Oil C. Margarine D. Soya Bean OilDocument8 pagesA. Ground Nut Oil B. Palm Oil C. Margarine D. Soya Bean Oildrpnnreddy100% (1)
- BD 1050 PartesDocument26 pagesBD 1050 PartesFelipe RojasNo ratings yet
- Ben'S Muffler RepairDocument9 pagesBen'S Muffler RepairDana LantoNo ratings yet
- Endicrine MCQ-QuestionsDocument4 pagesEndicrine MCQ-QuestionsThe White Army100% (1)
- 5 - Cardiac Output - Ass. Prof. Dalia Abd El-Salam - 2020Document6 pages5 - Cardiac Output - Ass. Prof. Dalia Abd El-Salam - 2020Hossam BaniisNo ratings yet
- ABG Practice Question AnswersDocument7 pagesABG Practice Question AnswersVidit JoshiNo ratings yet
- HW5e Beg CEFR Placement Test ADocument8 pagesHW5e Beg CEFR Placement Test AGabriel LemesNo ratings yet
- Biopolymers/Natural polymers structure and propertiesDocument78 pagesBiopolymers/Natural polymers structure and propertiesgautamahujaNo ratings yet
- Chapter 8-Mental Health and Well-Being in Middle and LateDocument15 pagesChapter 8-Mental Health and Well-Being in Middle and LateCathleen Beth100% (2)
- Chem Project Class 12 With Investigatory Project On ' Antacids'Document15 pagesChem Project Class 12 With Investigatory Project On ' Antacids'SHAHBAN55550% (1)
- Kuliah DislipidemiaDocument45 pagesKuliah DislipidemiaPaul Behring ManurungNo ratings yet
- Mojahid Sheet Complete PDFDocument176 pagesMojahid Sheet Complete PDFOsman SomiNo ratings yet
- Renukaprasad Ys - Medicine - Thesis NewDocument110 pagesRenukaprasad Ys - Medicine - Thesis NewLokesh ChopraNo ratings yet
- Biochemistry of Carbohydrate DigestionDocument10 pagesBiochemistry of Carbohydrate DigestionWaseem Abbas ShaikhNo ratings yet
- Cystic Fibrosis ResearchDocument7 pagesCystic Fibrosis ResearchElena RamblaNo ratings yet
- Digestive System Design Study GuideDocument3 pagesDigestive System Design Study Guideapi-390361165No ratings yet
- Cystic FibrosisDocument9 pagesCystic Fibrosisapi-432406854No ratings yet
- Krauses Essential HumanDocument315 pagesKrauses Essential HumanEllah MaeNo ratings yet
- MCQ ChoDocument31 pagesMCQ Choامجد حسين جواد كاظمNo ratings yet
- Basic Structure and Functions of the GI TractDocument10 pagesBasic Structure and Functions of the GI TractDwi Rezky AmaliaNo ratings yet
- Experiment To Estimate The Content of Ascorbic AcidDocument14 pagesExperiment To Estimate The Content of Ascorbic AcidDuncan KingNo ratings yet
- Exercise Metabolism PathwaysDocument31 pagesExercise Metabolism PathwaysHelmi RaisNo ratings yet
- Waxes: Structure, Composition, Occurrence and AnalysisDocument27 pagesWaxes: Structure, Composition, Occurrence and AnalysisNanda Rizky FathiyaNo ratings yet
- Acute PericarditisDocument8 pagesAcute Pericarditisalina abu rumiNo ratings yet
- Savva2016 PDFDocument8 pagesSavva2016 PDFHenry Rivero GarciaNo ratings yet
- Osmolarity vs OsmolalityDocument13 pagesOsmolarity vs OsmolalityBurhan HameedNo ratings yet
- FLUID COMPARTMENTSDocument44 pagesFLUID COMPARTMENTSO'Brien Alfred100% (1)
- Enhancement Course For Clerks Biochem Examination Part 2Document3 pagesEnhancement Course For Clerks Biochem Examination Part 2Kevin Alonzo100% (1)
- SiegenthalerDocument5 pagesSiegenthalerHeinz Purwadi Gunawan-SchoeckNo ratings yet
- Pancreatic Cancer: Pathophysiologic EtiologyDocument2 pagesPancreatic Cancer: Pathophysiologic EtiologyCharissa Magistrado De LeonNo ratings yet
- Two-Year Rural Family Medicine Residency ProgramDocument1 pageTwo-Year Rural Family Medicine Residency ProgramAlveera Zafar50% (2)
- 2.plasma ProteinsDocument5 pages2.plasma ProteinsAnusuya SNo ratings yet
- Cystic Fibrosis Diagnosis, Treatment & ManagementDocument28 pagesCystic Fibrosis Diagnosis, Treatment & ManagementAnita ThompsonNo ratings yet
- Regulation of GIT by gastrointestinal hormonesDocument13 pagesRegulation of GIT by gastrointestinal hormonesRaja Rashid IqbalNo ratings yet
- Zagazig University Pediatric ExamDocument4 pagesZagazig University Pediatric ExamSoad ShedeedNo ratings yet
- Physiology Final Exam - Glory 2017 PDFDocument14 pagesPhysiology Final Exam - Glory 2017 PDFMohammad BarakatNo ratings yet
- Regional Health Office Certificate Appearance June 2017Document1 pageRegional Health Office Certificate Appearance June 2017Jay AdamzNo ratings yet
- Hypercholesterolemia PDFDocument7 pagesHypercholesterolemia PDFkookiescreamNo ratings yet
- Pharmaa Topnotch ReviewDocument14 pagesPharmaa Topnotch ReviewArianne Joy C. TamarayNo ratings yet
- LO9&10Document13 pagesLO9&10Nine AranasNo ratings yet
- Artigo 10 - Nutrients-13-01244Document20 pagesArtigo 10 - Nutrients-13-01244Pedro AfonsoNo ratings yet
- Gill 2018Document20 pagesGill 2018Khumaira SantaNo ratings yet
- Dobrowolska-Iwanek Et-Al Hplc-Dad Method For The Quantitative Determination 2020Document7 pagesDobrowolska-Iwanek Et-Al Hplc-Dad Method For The Quantitative Determination 2020Dayanne ZeladaNo ratings yet
- Hydrochloric Acid: Material Safety Data SheetDocument7 pagesHydrochloric Acid: Material Safety Data Sheetpanji ajaNo ratings yet
- Anorganik 2Document31 pagesAnorganik 2SofiNo ratings yet
- Anorganik 2Document31 pagesAnorganik 2SofiNo ratings yet
- Perkenalan DLM B. IngDocument1 pagePerkenalan DLM B. IngSofiNo ratings yet
- Membran Plasma: Struktur Dan FungsiDocument7 pagesMembran Plasma: Struktur Dan FungsiSofiNo ratings yet
- Mitosis Meiosis Pka PDFDocument24 pagesMitosis Meiosis Pka PDFSofiNo ratings yet
- The Multiple Roles of Histidine in Protein Interactions: Researcharticle Open AccessDocument12 pagesThe Multiple Roles of Histidine in Protein Interactions: Researcharticle Open AccessSofiNo ratings yet
- Structure-Based Drug Design Studies of UDP-N-acetylglucosamine Pyrophosphosrylase, A Key Enzyme For The Control of Witches ' Broom DiseaseDocument7 pagesStructure-Based Drug Design Studies of UDP-N-acetylglucosamine Pyrophosphosrylase, A Key Enzyme For The Control of Witches ' Broom DiseaseSofiNo ratings yet
- Uganda National Urban ProfileDocument74 pagesUganda National Urban ProfileUnited Nations Human Settlements Programme (UN-HABITAT)No ratings yet
- Casa de Moda DolcegabbanaDocument4 pagesCasa de Moda Dolcegabbanadianaionelav23No ratings yet
- Listing of Equipment For Network DesignDocument3 pagesListing of Equipment For Network DesignJake D La MadridNo ratings yet
- Practicum HandbookDocument12 pagesPracticum HandbookChikezie NwankworNo ratings yet
- Complementary Therapies in Clinical Practice: Effect of Aromatherapy On Post-Partum Complications: A Systematic ReviewDocument7 pagesComplementary Therapies in Clinical Practice: Effect of Aromatherapy On Post-Partum Complications: A Systematic ReviewAras PinantiNo ratings yet
- RS9923 - Grade 12 Compulsory Subjects - Test Specification Chart and Model Questions - FinalDocument32 pagesRS9923 - Grade 12 Compulsory Subjects - Test Specification Chart and Model Questions - FinalPrince JaiswalNo ratings yet
- A Study On Satisfaction Level of Employees With Special Reference Textile IndustryDocument12 pagesA Study On Satisfaction Level of Employees With Special Reference Textile Industrysai kiran bade100% (1)
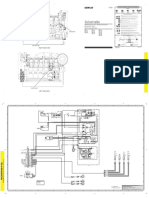
- Plano Grupo ElectrogenoDocument2 pagesPlano Grupo Electrogenoluis alberto rodriguezNo ratings yet
- DC-FAST 1.000, 2.000, 3.000, 5.000, 6.000 e 7.000 - New Project - 2021 - PT - BRDocument65 pagesDC-FAST 1.000, 2.000, 3.000, 5.000, 6.000 e 7.000 - New Project - 2021 - PT - BRCentrifugal SeparatorNo ratings yet
- Master FormDocument62 pagesMaster FormsamsulNo ratings yet
- Continuous Renal Replacement TherapyDocument9 pagesContinuous Renal Replacement Therapydoc_next_doorNo ratings yet
- Causes of Poverty - Presentation On Poverty - Poverty in PakistanDocument20 pagesCauses of Poverty - Presentation On Poverty - Poverty in PakistanTop_Sledger92% (12)
- Chapter 11 Post-Emulsified Fluorescent (Hydrophilic & Lipophilic)Document13 pagesChapter 11 Post-Emulsified Fluorescent (Hydrophilic & Lipophilic)maxpan maxNo ratings yet
- Rear Derailleur: Important Notice Names of PartsDocument1 pageRear Derailleur: Important Notice Names of PartsRyan MulyanaNo ratings yet
- Work Immersion PortfolioDocument15 pagesWork Immersion PortfolioKaye Irish RosauroNo ratings yet
- Help to Buy ISA GuideDocument4 pagesHelp to Buy ISA GuidefsdesdsNo ratings yet
- Report On PantaloonsDocument63 pagesReport On PantaloonsKashish AroraNo ratings yet
- MEH B1 Video Book Answer KeyDocument6 pagesMEH B1 Video Book Answer KeyTru CallingNo ratings yet
- Laporan FaalDocument25 pagesLaporan FaalAgnes NathaniaNo ratings yet
- AU440-36V-MH: DimensionsDocument2 pagesAU440-36V-MH: DimensionsJohnny FucahoriNo ratings yet
- Arthur Kleinman The Illness Narratives Suffering Healing and The Human ConditionDocument46 pagesArthur Kleinman The Illness Narratives Suffering Healing and The Human Conditionperdidalma62% (13)
- Jadwal Oral Presentation Peserta FIT-VIIIDocument26 pagesJadwal Oral Presentation Peserta FIT-VIIIKlinik FellitaNo ratings yet
- Warm Vs Cold ShockDocument8 pagesWarm Vs Cold ShockmarleeramirezNo ratings yet