You might also like
- Trigeminal Nerve: Anatomy and Pathology: Pictorial ReviewDocument10 pagesTrigeminal Nerve: Anatomy and Pathology: Pictorial Reviewbdalcin5512No ratings yet
- Lesion Del Tracto Cortico - Espinal InglesDocument14 pagesLesion Del Tracto Cortico - Espinal InglesCarolina Andrea Daza CharrisNo ratings yet
- Suprachoroidal Space InterventionsFrom EverandSuprachoroidal Space InterventionsShohista SaidkasimovaNo ratings yet
- Cranial Nerves Tomandl FinalDocument6 pagesCranial Nerves Tomandl FinalGaltieri OtavioNo ratings yet
- Referral of Diagnosis and Management of Erb-Duchenne PalsyDocument22 pagesReferral of Diagnosis and Management of Erb-Duchenne PalsyAshielaNo ratings yet
- Pediatric Neuroradiology, Part 2: Embryologic Basis For Inherited Neurological Disease and Congenital NeoplasmDocument8 pagesPediatric Neuroradiology, Part 2: Embryologic Basis For Inherited Neurological Disease and Congenital Neoplasmnsirakov77No ratings yet
- Neuroimaging Evaluation of Cerebral PalsDocument28 pagesNeuroimaging Evaluation of Cerebral PalsEntin KartiniNo ratings yet
- Clinical Approach To Brainstem LesionsDocument10 pagesClinical Approach To Brainstem LesionsJosé SánchezNo ratings yet
- Traumatic Medial Temporal Lobe Epilepsy Associated With A Subcortical Lesion in The Internal Capsule - A Case ReportDocument0 pagesTraumatic Medial Temporal Lobe Epilepsy Associated With A Subcortical Lesion in The Internal Capsule - A Case ReportAyu Ersya WindiraNo ratings yet
- Brainstem Stroke: Anatomy, Clinical and Radiological FindingsDocument11 pagesBrainstem Stroke: Anatomy, Clinical and Radiological FindingsMetta WitariNo ratings yet
- Neuro4Nurses Cerebellar StrokeDocument2 pagesNeuro4Nurses Cerebellar StrokeAisyahNurjannahNo ratings yet
- Cerebellar Ataxia Pathophysiology and RehabilitationDocument23 pagesCerebellar Ataxia Pathophysiology and RehabilitationMikail AtiyehNo ratings yet
- Brainsci 10 00538Document12 pagesBrainsci 10 00538Charles MorrisonNo ratings yet
- 2012 Cerebellar Ataxia - Pathophysiology and RehabilitationDocument22 pages2012 Cerebellar Ataxia - Pathophysiology and RehabilitationJefe de Escuela PsicologiaNo ratings yet
- Neuroanatomy Q 1 - 7: EANS/UEMS European Examination in NeurosurgeryDocument14 pagesNeuroanatomy Q 1 - 7: EANS/UEMS European Examination in NeurosurgeryAdel Saleh100% (1)
- Anatomy of Plexus BranchialisDocument24 pagesAnatomy of Plexus BranchialisAri Julian SaputraNo ratings yet
- Neuroimaging of Pediatric Brain InfectionsDocument52 pagesNeuroimaging of Pediatric Brain InfectionsTun Paksi SarehartoNo ratings yet
- Neuroanatomy Through Clinical Cases, 2E PDFDocument3 pagesNeuroanatomy Through Clinical Cases, 2E PDFjwongggg55140% (6)
- BMC Cardiovascular Disorders: Mönckeberg's Sclerosis - Is The Artery The Only Target of Calcification?Document8 pagesBMC Cardiovascular Disorders: Mönckeberg's Sclerosis - Is The Artery The Only Target of Calcification?Jonathan PanchiNo ratings yet
- Govaert2009 Prenatal StrokeDocument17 pagesGovaert2009 Prenatal StrokeModou NianeNo ratings yet
- MRI Imaging Reveals Meningitis and Ventriculitis ComplicationsDocument27 pagesMRI Imaging Reveals Meningitis and Ventriculitis ComplicationsLuis Diego López ManjarresNo ratings yet
- Anatomia InglesDocument12 pagesAnatomia InglesGerson SantosNo ratings yet
- Neuroanatomy, Pyramidal Tract - StatPearls - NCBI BookshelfDocument3 pagesNeuroanatomy, Pyramidal Tract - StatPearls - NCBI Bookshelfhermalina sabruNo ratings yet
- Orbital Pathology, EJR 2004Document38 pagesOrbital Pathology, EJR 2004Mauricio FrancoNo ratings yet
- Imaging of OrbitDocument69 pagesImaging of OrbitFaisal ShembeshNo ratings yet
- Causes of Stroke PDFDocument16 pagesCauses of Stroke PDFEmmanuel AguilarNo ratings yet
- Cerebellar StrokeDocument12 pagesCerebellar StrokewhitecloudsNo ratings yet
- REVIEW OF THE PHENOMENON OF DIASCHISIS IN CEREBRAL VASCULAR DISEASEDocument5 pagesREVIEW OF THE PHENOMENON OF DIASCHISIS IN CEREBRAL VASCULAR DISEASEEva Sala RenauNo ratings yet
- Distribution and Causes of Ischemic StrokesDocument11 pagesDistribution and Causes of Ischemic StrokesMatheus Nucci RiccettoNo ratings yet
- Seram2012 S-0118Document67 pagesSeram2012 S-0118RICARDO HUAMANNo ratings yet
- Role of Diffusion-Weighted Imaging and Proton MR Spectroscopy in Distinguishing Between Pyogenic Brain Abscess and Necrotic Brain TumorDocument7 pagesRole of Diffusion-Weighted Imaging and Proton MR Spectroscopy in Distinguishing Between Pyogenic Brain Abscess and Necrotic Brain TumorLulu SupergirlNo ratings yet
- Adult Traumatic Brachial Plexus Injury: J.J. RankineDocument8 pagesAdult Traumatic Brachial Plexus Injury: J.J. RankineSuhartiniNo ratings yet
- Causas de Isquemia Na MedulaDocument12 pagesCausas de Isquemia Na MeduladianaNo ratings yet
- Radiology SignsDocument99 pagesRadiology SignsPartha GanesanNo ratings yet
- Thalamic Stroke and BehaviourDocument9 pagesThalamic Stroke and BehaviourparkdhingraNo ratings yet
- Clinical Imaging: Jared Narvid, Jason F. Talbott, Christine M. GlastonburyDocument10 pagesClinical Imaging: Jared Narvid, Jason F. Talbott, Christine M. GlastonburyIrina TurcanuNo ratings yet
- Neonatal Head UltrasoundDocument8 pagesNeonatal Head Ultrasoundvera dianaNo ratings yet
- Ecr2013 C-2557Document33 pagesEcr2013 C-2557olaNo ratings yet
- Multiple Cranial Nerve PalsiesDocument11 pagesMultiple Cranial Nerve PalsiesVijay BabuNo ratings yet
- Malak 2021Document19 pagesMalak 2021Firmansyah FirmansyahNo ratings yet
- Pure Thalamic Infarctions Clinical FindingsDocument11 pagesPure Thalamic Infarctions Clinical FindingsshofidhiaaaNo ratings yet
- Neuroimaging Patterns of Intracranial Infections Meningitis, Cerebritis, and Their ComplicationsDocument31 pagesNeuroimaging Patterns of Intracranial Infections Meningitis, Cerebritis, and Their ComplicationsMauro Oscar Soares De Souza LimaNo ratings yet
- New Perspectives by Imaging Modalities For An Old Illness: Rheumatic Mitral StenosisDocument13 pagesNew Perspectives by Imaging Modalities For An Old Illness: Rheumatic Mitral StenosisNasriNo ratings yet
- EPIDURAL HEMATOM Kel 3Document15 pagesEPIDURAL HEMATOM Kel 3Rizka Desti AyuniNo ratings yet
- J Neurol Neurosurg Psychiatry 1993 Ropper 932 5Document5 pagesJ Neurol Neurosurg Psychiatry 1993 Ropper 932 5Anonymous 6iwMFwNo ratings yet
- Spine and Spinal Cord Injury Guide: Causes, Symptoms and TreatmentsDocument47 pagesSpine and Spinal Cord Injury Guide: Causes, Symptoms and TreatmentsAde Zulfiah100% (1)
- A Beginner's Guide To Brain CT in Acute Stroke: Poster No.: Congress: Type: Authors: KeywordsDocument34 pagesA Beginner's Guide To Brain CT in Acute Stroke: Poster No.: Congress: Type: Authors: KeywordsHasbi Ash ShiddiqieNo ratings yet
- Radio Logical Finding PCNSLDocument12 pagesRadio Logical Finding PCNSLKhushalchand KanjiNo ratings yet
- Stroke in The Newborn: Terrie E. Inder Joseph J. VolpeDocument33 pagesStroke in The Newborn: Terrie E. Inder Joseph J. VolpeHaveezhNo ratings yet
- Distribution Territories and Causative MechanismsDocument12 pagesDistribution Territories and Causative MechanismsIkhsan FebriansyahNo ratings yet
- CPA Lesion Imaging Guide: Enhancing Extra-Axial MassesDocument11 pagesCPA Lesion Imaging Guide: Enhancing Extra-Axial MassesKhương Hà NguyễnNo ratings yet
- Imaging Appearances of Unusual Conditions of The Middle and Inner EarDocument11 pagesImaging Appearances of Unusual Conditions of The Middle and Inner EarKieda MaliqiNo ratings yet
- Spinal CordDocument15 pagesSpinal Cordsimi y100% (1)
- Cerebral Vein and Dural Sinus ThrombosisDocument32 pagesCerebral Vein and Dural Sinus ThrombosisdwiNo ratings yet
- Dolgorjav Radiology Skull Base LangeDocument66 pagesDolgorjav Radiology Skull Base LangeodonchimegNo ratings yet
- Anatomy of Plexus Branchialis PDFDocument24 pagesAnatomy of Plexus Branchialis PDFGemantri veyonda ZikryNo ratings yet
- A Quick Guide For Neuroimaging of Common Dementias Seen in Clinical PracticeDocument8 pagesA Quick Guide For Neuroimaging of Common Dementias Seen in Clinical PracticeAndika ResaNo ratings yet
- Extra Aksial Brain TumorsDocument15 pagesExtra Aksial Brain TumorsPPDSNeuroUnsri RSMH0% (1)
- ASH TTP RituximabDocument6 pagesASH TTP RituximabJulius Dominique L. AnjaoNo ratings yet
- Ash TTP RefractoryDocument8 pagesAsh TTP RefractoryJulius Dominique L. AnjaoNo ratings yet
- Artigo de Revisao Purpura Trombocitopenica TromboticaDocument11 pagesArtigo de Revisao Purpura Trombocitopenica TromboticaPlaneta SosNo ratings yet
- Typhoid Case PresentationDocument79 pagesTyphoid Case PresentationJulius Dominique L. AnjaoNo ratings yet
- Emailing CPG-E PDFDocument206 pagesEmailing CPG-E PDFCarlos H. AcuñaNo ratings yet
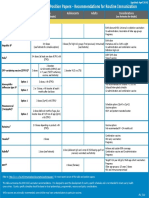
- Immunization Routine Table1 PDFDocument11 pagesImmunization Routine Table1 PDFSelvi ChandranNo ratings yet
- A Local Case of Mri-Diagnosed Horseshoe Perianal Fistula in A 38 Year Old MaleDocument12 pagesA Local Case of Mri-Diagnosed Horseshoe Perianal Fistula in A 38 Year Old MaleJulius Dominique L. AnjaoNo ratings yet
- Tropho Pharma PDFDocument2 pagesTropho Pharma PDFJulius Dominique L. AnjaoNo ratings yet
- Nervous SYSTESTDocument19 pagesNervous SYSTESTedwalk1250% (2)
- 2 The Sound-Producing SystemDocument2 pages2 The Sound-Producing SystemRoberto Carlos Sosa BadilloNo ratings yet
- CT Neck Anatomy DemystifiedDocument26 pagesCT Neck Anatomy DemystifiedTapi imaging centre Vyara dist TapiNo ratings yet
- The Fetal SkullDocument36 pagesThe Fetal SkullSubhada Gosavi100% (1)
- Oral Anatomy & Physiology TestDocument34 pagesOral Anatomy & Physiology TestEliza EllieNo ratings yet
- Método Canto E Delle SedieDocument196 pagesMétodo Canto E Delle SedieSsue30No ratings yet
- Anato TestDocument69 pagesAnato Testeyash.6No ratings yet
- Anatomy and Physiology of LarynxDocument13 pagesAnatomy and Physiology of LarynxAmin MasromNo ratings yet
- TBI QuizletDocument4 pagesTBI QuizletLoraine CometaNo ratings yet
- General Surgery MCQDocument9 pagesGeneral Surgery MCQSAlemsa88% (8)
- Ceu Revalida Ga Oa GPF OpfDocument97 pagesCeu Revalida Ga Oa GPF OpfPAULINE BERNARDONo ratings yet
- Chapter 3 - Structure of The Nervous SystemDocument8 pagesChapter 3 - Structure of The Nervous Systemmanilyn dacoNo ratings yet
- Lecture 3 - Sept 14 - CH 2 Part 2 - Neuronal Basis For Cognition - REVISED POSTED SLIDESDocument29 pagesLecture 3 - Sept 14 - CH 2 Part 2 - Neuronal Basis For Cognition - REVISED POSTED SLIDESnathanagbeyi772000No ratings yet
- Preauricular SineDocument5 pagesPreauricular SineAldy BimaNo ratings yet
- Chapter 4. Movement and Learning: Teaching With The Brain in Mind, 2nd EditionDocument3 pagesChapter 4. Movement and Learning: Teaching With The Brain in Mind, 2nd EditionJason Oscar RobertsNo ratings yet
- Anatomy and Physiology of The Respiratory TractDocument49 pagesAnatomy and Physiology of The Respiratory TractshvnagaNo ratings yet
- Surgery SLE MCQDocument34 pagesSurgery SLE MCQAsif NewazNo ratings yet
- Material Downloaded From SUPERCOPDocument6 pagesMaterial Downloaded From SUPERCOPfast-track for n2021No ratings yet
- Mental NerveDocument5 pagesMental NerveAyitiYonLotImajNo ratings yet
- Nervous System Reaction PaperDocument3 pagesNervous System Reaction PaperJohn Ruel Sanchez IINo ratings yet
- Bone Marking Table KpattonDocument3 pagesBone Marking Table Kpattontdionysakopoulos100% (2)
- THE SPEAKING PROCESS BREATHING, PHONATION, RESONATION & ARTICULATIONDocument2 pagesTHE SPEAKING PROCESS BREATHING, PHONATION, RESONATION & ARTICULATIONJames William100% (1)
- Anatomyofthe Annexesofthe Digestive TractDocument67 pagesAnatomyofthe Annexesofthe Digestive TractsreedamNo ratings yet
- Anatomia e Njeriut - N. Behxhet, S. Cerkezi, A. Muca, Me Bp.Document208 pagesAnatomia e Njeriut - N. Behxhet, S. Cerkezi, A. Muca, Me Bp.Rinor Mujaj91% (129)
- © NGSS Life Science 2015Document3 pages© NGSS Life Science 2015Iram AzizNo ratings yet
- Department of Hormones: TSH 1.1 mIU/LDocument1 pageDepartment of Hormones: TSH 1.1 mIU/LSankar KsNo ratings yet
- Human Anatomy & Physiology: Chapter 21-1Document103 pagesHuman Anatomy & Physiology: Chapter 21-1AngelyNo ratings yet
- Right Hemisphere Cognitive Functions - From Clinical and Anatomical Bases To Brain Mapping During Awake Craniotomy Part II - Neuropsychological Tasks and Brain MappingDocument8 pagesRight Hemisphere Cognitive Functions - From Clinical and Anatomical Bases To Brain Mapping During Awake Craniotomy Part II - Neuropsychological Tasks and Brain MappingHellen SantosNo ratings yet
- Audiometer Chapter 2 CorrectedDocument13 pagesAudiometer Chapter 2 CorrectedseunNo ratings yet
- Ent Midterms SamplexDocument7 pagesEnt Midterms SamplexdeevoncNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)