You might also like
- BRAINSTEM II Clinical CorrelatesDocument6 pagesBRAINSTEM II Clinical CorrelatesrizaNo ratings yet
- Neuro AnatomyDocument4 pagesNeuro AnatomyMarianne Abnasan100% (1)
- Horner Syndrome: Kelly A. Walton and Lawrence M. BuonoDocument7 pagesHorner Syndrome: Kelly A. Walton and Lawrence M. BuonoEgi NabilaNo ratings yet
- Crim Medicine2013-296874Document3 pagesCrim Medicine2013-296874Batra AldigaNo ratings yet
- Disorders of The Spinal Cord and RootsDocument9 pagesDisorders of The Spinal Cord and RootsMariana Hoyos GallegoNo ratings yet
- Tables NurologyDocument5 pagesTables NurologyRazan AlayedNo ratings yet
- Nervioso First AidDocument62 pagesNervioso First Aidadrenalina1238No ratings yet
- Neurology and Special Senses: High-Yield SystemsDocument72 pagesNeurology and Special Senses: High-Yield SystemsMahmoud Abu MayalehNo ratings yet
- Cerebrovascular Accident or Stroke (Also: Called Brain Attack) Results From SuddenDocument2 pagesCerebrovascular Accident or Stroke (Also: Called Brain Attack) Results From Suddenskullem18No ratings yet
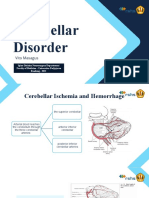
- ISMT12 - Day 457 - Vito - Cerebellar DisorderDocument17 pagesISMT12 - Day 457 - Vito - Cerebellar DisorderVito MasagusNo ratings yet
- Pituitaria SEMINARSDocument12 pagesPituitaria SEMINARSNathaly CantorNo ratings yet
- Emrbyo Lab Whole Mount: HR Chick ReviewerDocument7 pagesEmrbyo Lab Whole Mount: HR Chick ReviewerDimple May Gianne DumaguitNo ratings yet
- 1.3 Neural Development and Neurogenesis (Final)Document4 pages1.3 Neural Development and Neurogenesis (Final)Austin CabreraNo ratings yet
- CNS - Infections F2022 OVER VIEWDocument18 pagesCNS - Infections F2022 OVER VIEWMadison MillwoodNo ratings yet
- Cedees Smart Notes - General Surgery Part 2Document43 pagesCedees Smart Notes - General Surgery Part 2MohitNo ratings yet
- Emrbyo Lab Whole Mount: 48 HR Chick ReviewerDocument6 pagesEmrbyo Lab Whole Mount: 48 HR Chick ReviewerChristine Mae DelimaNo ratings yet
- Orientation Agnosia in Pentagon CopyingDocument22 pagesOrientation Agnosia in Pentagon CopyingasasakopNo ratings yet
- Ward Roger2001Document6 pagesWard Roger2001AntonyNo ratings yet
- NeuroDocument71 pagesNeuroSaily JaquezNo ratings yet
- Brainstem Stroke SyndromesDocument43 pagesBrainstem Stroke SyndromesSarah Choo Qian RouNo ratings yet
- Cerebellum & DiencephalonDocument21 pagesCerebellum & Diencephalonprasun_vNo ratings yet
- Featured Applied Radiology Article: Pediatric Neuroradiology Part 1 - Embryo Logic Basis For Brain MalformationDocument12 pagesFeatured Applied Radiology Article: Pediatric Neuroradiology Part 1 - Embryo Logic Basis For Brain MalformationradRounds Radiology NetworkNo ratings yet
- Topognosis of Facial Nerve LesionsDocument11 pagesTopognosis of Facial Nerve LesionsAudiologiaNo ratings yet
- An Intresting Case of TremorDocument3 pagesAn Intresting Case of TremorGopi Krishnan RNo ratings yet
- Etchevers Et Al., 1999Document11 pagesEtchevers Et Al., 1999Fabiana R.No ratings yet
- Clinical Neurology: Module 1: Identifying Ischemic Locales Module 2: StrokeDocument19 pagesClinical Neurology: Module 1: Identifying Ischemic Locales Module 2: Strokealix dayNo ratings yet
- Tentorial IncisuraDocument23 pagesTentorial Incisurabodeadumitru9261100% (1)
- Mrcs NeurosurgeryDocument28 pagesMrcs NeurosurgeryAdebisiNo ratings yet
- Neuroanatomy: Prelim Term ExamDocument34 pagesNeuroanatomy: Prelim Term ExamPi NgNo ratings yet
- Neuro AvesDocument23 pagesNeuro AvesMiriam CaramicoNo ratings yet
- Chapters 27 28 TrippleDocument9 pagesChapters 27 28 TripplegeorgefrombaNo ratings yet
- Acute and Chronic Pain Following Craniotomy: A Review: ReviewarticleDocument12 pagesAcute and Chronic Pain Following Craniotomy: A Review: ReviewarticleКулик АндрійNo ratings yet
- Where Da Lesion atDocument5 pagesWhere Da Lesion atDeeWallyNo ratings yet
- An Update On Cutaneous Tumours With Neural DifferentiationDocument24 pagesAn Update On Cutaneous Tumours With Neural DifferentiationAdriana Gabriela Ugarte MacíasNo ratings yet
- Introduc On: Jonardi Prissilma Tania, Chan Abdul Aziz, Putri Kuncoro Rahmadinda, Puspowa AdiDocument1 pageIntroduc On: Jonardi Prissilma Tania, Chan Abdul Aziz, Putri Kuncoro Rahmadinda, Puspowa AdiPrissilma TaniaNo ratings yet
- Pictorial Review: Congenital Spine and Spinal Cord MalformationsDocument12 pagesPictorial Review: Congenital Spine and Spinal Cord MalformationsDr.Samreen SulthanaNo ratings yet
- Chapter 7 THE MENINGESDocument16 pagesChapter 7 THE MENINGESRoger Fernando Abril DiazNo ratings yet
- NeurologyDocument33 pagesNeurologyjhqmpzg7sjNo ratings yet
- Peripheral Nerve Injury: Relevant Anatomy: Peripheral Neuroanatomy andDocument7 pagesPeripheral Nerve Injury: Relevant Anatomy: Peripheral Neuroanatomy andJulia SalvioNo ratings yet
- Clinicopathologic Features of Brain Herniation in AnimalsDocument7 pagesClinicopathologic Features of Brain Herniation in AnimalsDesNo ratings yet
- Benedict SyndromeDocument5 pagesBenedict SyndromeSora KerovaNo ratings yet
- NBSS CASE 6 - Cerebral Palsy and Mental RetardationDocument28 pagesNBSS CASE 6 - Cerebral Palsy and Mental RetardationbungadielaNo ratings yet
- Wallerian of Brain:MRI and CT Findings: DegenerationDocument3 pagesWallerian of Brain:MRI and CT Findings: Degenerationneela kantaNo ratings yet
- Neurulation: Ormation of Neural Tube-The Best Studied Example of OrganogenesisDocument5 pagesNeurulation: Ormation of Neural Tube-The Best Studied Example of OrganogenesisKhushbuNo ratings yet
- General Pathology 4.03 Endocrine System Super SummaryDocument15 pagesGeneral Pathology 4.03 Endocrine System Super SummaryJade MonrealNo ratings yet
- Coma and Related Disorders of ConsciousnessDocument46 pagesComa and Related Disorders of ConsciousnessdeliarelaNo ratings yet
- Neuroanatomy PDFDocument12 pagesNeuroanatomy PDFM D100% (2)
- Diploma in Occupational TherapyDocument47 pagesDiploma in Occupational TherapyAzmi Plus100% (2)
- Diseases of The Spinal CordDocument15 pagesDiseases of The Spinal CordBai Aishwayra Haylee DalidigNo ratings yet
- Somatosensory Evoked Potentials: Root Traverse Root ToDocument15 pagesSomatosensory Evoked Potentials: Root Traverse Root ToSadaf IrfanNo ratings yet
- 17174-Imging of Cerebellopontine Angle - Prof El BeltagiDocument10 pages17174-Imging of Cerebellopontine Angle - Prof El BeltagiPugazhenthi CNo ratings yet
- Neuroscience II: CerebellumDocument13 pagesNeuroscience II: CerebellumTrina CardonaNo ratings yet
- Multiple SclerosisDocument8 pagesMultiple SclerosisRivera CharmaineNo ratings yet
- NEURO2 3.05 Neurosurgical Management of Stroke and CNS Infection - Dr. Domingo PDFDocument3 pagesNEURO2 3.05 Neurosurgical Management of Stroke and CNS Infection - Dr. Domingo PDFPatricia Nicole AlcarazNo ratings yet
- SistemendokrinDocument26 pagesSistemendokrinNazwa AuliaNo ratings yet
- Diseases of The Peripheral Facial Nerve: Khristine T. Girado - Pizarro, MD, FPSO-HNSDocument29 pagesDiseases of The Peripheral Facial Nerve: Khristine T. Girado - Pizarro, MD, FPSO-HNSAria Jean MostajoNo ratings yet
- Neuron2 0331Document77 pagesNeuron2 0331baharehNo ratings yet
- Arterial Supply of The Thalamus - A Comprehensive ReviewDocument9 pagesArterial Supply of The Thalamus - A Comprehensive Reviewمحمد رؤوف خير الدينNo ratings yet
- Excitable Cells: Monographs in Modern Biology for Upper School and University CoursesFrom EverandExcitable Cells: Monographs in Modern Biology for Upper School and University CoursesNo ratings yet
- Cerebral Circulation DimalNPM Final 051221Document80 pagesCerebral Circulation DimalNPM Final 051221Chok ArgoniaNo ratings yet
- The Grasp and Other Primitive Reflexes: Review: Physical SignsDocument3 pagesThe Grasp and Other Primitive Reflexes: Review: Physical SignsNommandurNo ratings yet
- Wami Chizarum Project For BuhrecDocument29 pagesWami Chizarum Project For BuhrecMarvellous OkonobohNo ratings yet
- Official USMLE Step 1 Sample Test Questions 2010Document53 pagesOfficial USMLE Step 1 Sample Test Questions 2010Usmle TakerNo ratings yet
- Truncus Cerebri: Bagian Anatomi Fkik-Uin Alauddin MakassarDocument37 pagesTruncus Cerebri: Bagian Anatomi Fkik-Uin Alauddin MakassaryuyuNo ratings yet
- Why Humans Like Junk Food Steven WitherlyDocument208 pagesWhy Humans Like Junk Food Steven WitherlyAndra GanaiteNo ratings yet
- Personal Medical History: Doctor Visit ChecklistDocument11 pagesPersonal Medical History: Doctor Visit ChecklistValentina VillarrealNo ratings yet
- (Healthy Ageing and Longevity, 18) Anita Jagota - Sleep and Clocks in Aging and Longevity-Springer (2023)Document552 pages(Healthy Ageing and Longevity, 18) Anita Jagota - Sleep and Clocks in Aging and Longevity-Springer (2023)amrjano.ajNo ratings yet
- Dos 773 Csi Plan Study-1Document7 pagesDos 773 Csi Plan Study-1api-504593245No ratings yet
- Brain ReprogrammingDocument50 pagesBrain Reprogramminghohgch100% (4)
- Mental and Elemental NutrientsDocument21 pagesMental and Elemental NutrientsGilbert RivaNo ratings yet
- Basal Ganglia-KreitzerDocument51 pagesBasal Ganglia-KreitzerresearchphysioNo ratings yet
- Consciousness: The Last 50 Years (And The Next) : Anil K. SethDocument6 pagesConsciousness: The Last 50 Years (And The Next) : Anil K. SethadrianomarramirezNo ratings yet
- 2015 Bookmatter FundamentalsOfNeurologicDiseasDocument18 pages2015 Bookmatter FundamentalsOfNeurologicDiseasSabrin BadarneNo ratings yet
- Featured Applied Radiology Article: Pediatric Neuroradiology Part 1 - Embryo Logic Basis For Brain MalformationDocument12 pagesFeatured Applied Radiology Article: Pediatric Neuroradiology Part 1 - Embryo Logic Basis For Brain MalformationradRounds Radiology NetworkNo ratings yet
- Theories and TherapiesDocument15 pagesTheories and TherapiesKRAZEL MICAH NazarenoNo ratings yet
- Silva Life System WorkbookDocument66 pagesSilva Life System WorkbookGeorge Stefanakidis92% (26)
- LiteratureReview-trauma Sensitive Approach PDFDocument40 pagesLiteratureReview-trauma Sensitive Approach PDFhanabbechara100% (1)
- Genes and BehaviourDocument11 pagesGenes and BehaviourRutuja BhoyarNo ratings yet
- Meditation - Kamlesh Patel in HFN Magazine-Issue 2-2015 PDFDocument1 pageMeditation - Kamlesh Patel in HFN Magazine-Issue 2-2015 PDFanon_630497556No ratings yet
- Skenario 2 Saraf & PerilakuDocument30 pagesSkenario 2 Saraf & PerilakuPrima Eriawan PutraNo ratings yet
- Per Dev ReviewerDocument5 pagesPer Dev ReviewerIshie De GuzmanNo ratings yet
- Behaviorism and Mind: B. F. SkinnerDocument15 pagesBehaviorism and Mind: B. F. SkinnerDavid DennenNo ratings yet
- Ring The Alarm! - PreviewDocument34 pagesRing The Alarm! - PreviewNikolai Pizarro de JesusNo ratings yet
- Üds 2008 Sağlık Sonbahar EkimDocument15 pagesÜds 2008 Sağlık Sonbahar EkimDr. Hikmet ŞahinerNo ratings yet
- Grade V CBSE Compiled Q PaperDocument101 pagesGrade V CBSE Compiled Q PaperrajeshragavanNo ratings yet
- XI Term 1 QPDocument7 pagesXI Term 1 QPstwilfred primaryNo ratings yet
- Introduction To Laplacian Montages: American Journal of Electroneurodiagnostic TechnologyDocument6 pagesIntroduction To Laplacian Montages: American Journal of Electroneurodiagnostic TechnologyCarlos AcostaNo ratings yet
- Lindquist Etal BBS2012Document82 pagesLindquist Etal BBS2012deboorerdiepinNo ratings yet
- Neuroanatomy QbankDocument27 pagesNeuroanatomy Qbankbbbanyi67% (3)