You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- 10 Things I've Learned About Bitch Management, Pimp PDFDocument5 pages10 Things I've Learned About Bitch Management, Pimp PDFyhcrxv6n3j13No ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- 10 Ways To Sell 100,000 Copies of Your Book PDFDocument6 pages10 Ways To Sell 100,000 Copies of Your Book PDFyhcrxv6n3j13No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- AfterburnerDocument1 pageAfterburneryhcrxv6n3j13No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- 10 Things I've Learned About Bitch Management, Pimp PDFDocument5 pages10 Things I've Learned About Bitch Management, Pimp PDFyhcrxv6n3j13No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- D:s Negotiation Questions-1Document5 pagesD:s Negotiation Questions-1yhcrxv6n3j13100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Creative BDSM Toy SourcesDocument2 pagesCreative BDSM Toy Sourcesyhcrxv6n3j13100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Caring DominationDocument149 pagesCaring DominationAugusto Benevenuto MachadoNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- CBT Handout PDFDocument6 pagesCBT Handout PDFyhcrxv6n3j13No ratings yet
- Spinning Spin Plate Theory - The Rational MaleDocument13 pagesSpinning Spin Plate Theory - The Rational Maleyhcrxv6n3j13No ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Binding The Family JewelsDocument9 pagesBinding The Family Jewelsyhcrxv6n3j1350% (2)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Interrogation Approaches Direct ApproachDocument20 pagesInterrogation Approaches Direct Approachyhcrxv6n3j13No ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Constance Pennington Smythe - Female Domination 101 (2008) PDFDocument32 pagesConstance Pennington Smythe - Female Domination 101 (2008) PDFFluti67% (9)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- How To Deal With The Other Women Question - by Black Dragon PDFDocument15 pagesHow To Deal With The Other Women Question - by Black Dragon PDFyhcrxv6n3j13100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- High Protocol Manual For Philly Parties - FINALDocument18 pagesHigh Protocol Manual For Philly Parties - FINALyhcrxv6n3j13100% (3)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Sex Clubs Non Monogamy and GameDocument120 pagesSex Clubs Non Monogamy and Gameyhcrxv6n3j13100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Argumentative Essay Draft 2Document4 pagesArgumentative Essay Draft 2api-285282547No ratings yet
- Patients Rights: Presented By: Ederlyn Papa-Destura, RN, ManDocument57 pagesPatients Rights: Presented By: Ederlyn Papa-Destura, RN, ManteuuuuNo ratings yet
- Workout RoutineDocument2 pagesWorkout RoutineSudeep SinghalNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Management of Overweight and Obesity in Primary CareDocument13 pagesManagement of Overweight and Obesity in Primary CarezenNo ratings yet
- UntitledDocument417 pagesUntitledFatima VelazcoNo ratings yet
- MCM Youth E-Nnovation Summit (MCM YES)Document6 pagesMCM Youth E-Nnovation Summit (MCM YES)z permruruNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Module 1.1 Introduction To Physical EducationDocument10 pagesModule 1.1 Introduction To Physical EducationRG MendozaNo ratings yet
- Phenyl Methyl Silicone OilDocument7 pagesPhenyl Methyl Silicone OilatjaiNo ratings yet
- Stones HealingDocument11 pagesStones HealingMarijanaLončarDesančićNo ratings yet
- Medicatia Ulcer GastricDocument26 pagesMedicatia Ulcer GastricNatalia MelnicNo ratings yet
- Mop - Perbaikan Instalasi Pipa Air Bersih - Cyber 1Document4 pagesMop - Perbaikan Instalasi Pipa Air Bersih - Cyber 1GUSTIAN HERMANANo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Reep Esl Curriculum For Adults Going To The DoctorDocument3 pagesReep Esl Curriculum For Adults Going To The DoctorMetztli Ximena MonteroNo ratings yet
- APA Research Proposal 2021Document14 pagesAPA Research Proposal 2021med wardNo ratings yet
- General Chemistry 1: First Quarter-Module 2: Atomic StructureDocument26 pagesGeneral Chemistry 1: First Quarter-Module 2: Atomic StructureAlessandra Gabrielle GarezNo ratings yet
- Case Study 2Document29 pagesCase Study 2falguni mondalNo ratings yet
- JoeWellerFit Transformation Guide (Copyright Joe Weller 2022)Document19 pagesJoeWellerFit Transformation Guide (Copyright Joe Weller 2022)yzd26xf2gtNo ratings yet
- LESSON 1 EED Spec 322Document5 pagesLESSON 1 EED Spec 322Jhezmae Rose Pasion AlonzoNo ratings yet
- MSLSS Multidimensional Student Life Satisfaction ScaleDocument3 pagesMSLSS Multidimensional Student Life Satisfaction ScaleChris Gabriel Ucol100% (1)
- Complete Guide To The Philippine Med Licensure ExamsDocument62 pagesComplete Guide To The Philippine Med Licensure ExamsanonymousNo ratings yet
- ASPERGER'SDocument4 pagesASPERGER'SJohana NyagayaNo ratings yet
- Theories Human DevelopmentDocument37 pagesTheories Human DevelopmentEdgar Alan Poe92% (13)
- TFN Comprehensive Exam (Rationalization) Flashcards QuizletDocument1 pageTFN Comprehensive Exam (Rationalization) Flashcards QuizletOnefur TriiNo ratings yet
- Contrasting Contemporary Population Issues Geofile 521Document3 pagesContrasting Contemporary Population Issues Geofile 521reservoirgeogsNo ratings yet
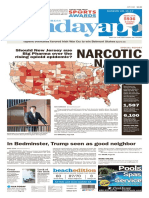
- Asbury Park Press Front Page, Sunday, June 11, 2017Document1 pageAsbury Park Press Front Page, Sunday, June 11, 2017Asbury Park PressNo ratings yet
- Group3 - BSN1-6 - Therapeutic Communication in The Helping Relationship - PresentationDocument16 pagesGroup3 - BSN1-6 - Therapeutic Communication in The Helping Relationship - PresentationRalf FiedalinoNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- SSC Home Learning Plan Week 4Document9 pagesSSC Home Learning Plan Week 4Dangay National High SchoolNo ratings yet
- CANTEEN SERVICES AND STUDENTS SATISFACTION OF 2ND YEAR STUDENTS OF BACHELOR IN NURSING AT CSPC (BTVTEd3A) - ACTIVITY 1Document2 pagesCANTEEN SERVICES AND STUDENTS SATISFACTION OF 2ND YEAR STUDENTS OF BACHELOR IN NURSING AT CSPC (BTVTEd3A) - ACTIVITY 1Yessamin Villadares PetchayNo ratings yet
- Hostel LifeDocument4 pagesHostel LifeSumanNo ratings yet
- Part IDocument8 pagesPart IMj Ong Pierson GarboNo ratings yet
- 2nd Mid Term Exam Date Sheet by SHM Updated Final 2023Document1 page2nd Mid Term Exam Date Sheet by SHM Updated Final 2023Dipendra YadavNo ratings yet