You might also like
- Risk Assesssment IG2 ReportDocument18 pagesRisk Assesssment IG2 ReportRashid Jamil25% (4)
- Implant Placement and Loading ProtocolsDocument3 pagesImplant Placement and Loading ProtocolsFikrat0% (2)
- 7 RetainerinorthodonticsDocument6 pages7 RetainerinorthodonticsSahana RangarajanNo ratings yet
- Treatment Planning Single Maxillary Anterior Implants for DentistsFrom EverandTreatment Planning Single Maxillary Anterior Implants for DentistsNo ratings yet
- Occlusion in FPD and IMPLANTSDocument68 pagesOcclusion in FPD and IMPLANTSDRSH100% (1)
- Functionally Generated PathDocument37 pagesFunctionally Generated PathsabnoorNo ratings yet
- Intracoronal Attachments For Removable Partial DenturesDocument18 pagesIntracoronal Attachments For Removable Partial Denturesapi-3710948100% (6)
- Objectives of Impression MakingDocument24 pagesObjectives of Impression MakingMadiha ZufaNo ratings yet
- Implantfailurepankajfinal 160120192933Document104 pagesImplantfailurepankajfinal 160120192933DrIbrahimShaikh100% (1)
- 3137 01 3RP AFP tcm143-665835Document12 pages3137 01 3RP AFP tcm143-665835jcarbonesNo ratings yet
- Facebow Calliper ReviewDocument5 pagesFacebow Calliper ReviewFaheemuddin Muhammad100% (3)
- Provisionals in Dentistry - From Past To Recent Advances: Rohitraghavan, Shajahan P A, NeenakunjumonDocument6 pagesProvisionals in Dentistry - From Past To Recent Advances: Rohitraghavan, Shajahan P A, Neenakunjumonnavdeep100% (1)
- Precision Attachments For The 21st CenturyDocument6 pagesPrecision Attachments For The 21st CenturyMohsin Habib67% (3)
- Mandibular MovementDocument56 pagesMandibular MovementSahana RangarajanNo ratings yet
- Posterior Palatal Seal 1st SeminarDocument62 pagesPosterior Palatal Seal 1st SeminarMayank AggarwalNo ratings yet
- Occlusal Consideration in Implant ProsthesisDocument59 pagesOcclusal Consideration in Implant ProsthesisDrFarha NazNo ratings yet
- Review: Types of Finish Lines or Gingival Margins Intooth PreparationDocument6 pagesReview: Types of Finish Lines or Gingival Margins Intooth PreparationSahana RangarajanNo ratings yet
- Retention in Complete DentureDocument53 pagesRetention in Complete DentureVikas Aggarwal67% (3)
- Exam in Community Engagement Solidarity & CitizenshipDocument4 pagesExam in Community Engagement Solidarity & Citizenshiplovelyjanemartin100% (8)
- Prostho Rehabilitation - HypodontiaDocument24 pagesProstho Rehabilitation - HypodontiaAmniAzmiNo ratings yet
- Treatment Planning For Fixed Partial DenturesDocument3 pagesTreatment Planning For Fixed Partial DenturesfarafznNo ratings yet
- ARTICULATORSDocument161 pagesARTICULATORSNikita ParasrampuuriaNo ratings yet
- Precision Attachments.Document92 pagesPrecision Attachments.unifiles100% (2)
- 3D Printing Industry Roadmap - India (Aerospace) Summit DocumentDocument19 pages3D Printing Industry Roadmap - India (Aerospace) Summit DocumentSahana RangarajanNo ratings yet
- 2 Partial Denture Design FayadDocument53 pages2 Partial Denture Design FayadMostafa Fayad100% (3)
- Dr. Omkar Shetty - ProsthoDocument7 pagesDr. Omkar Shetty - ProsthoSyed NooraniNo ratings yet
- Treatment Options For The Free End SaddleDocument5 pagesTreatment Options For The Free End SaddleBakr Ahmed40% (5)
- Supra-Gingival Minimally Invasive Dentistry: A Healthier Approach to Esthetic RestorationsFrom EverandSupra-Gingival Minimally Invasive Dentistry: A Healthier Approach to Esthetic RestorationsRating: 5 out of 5 stars5/5 (1)
- Occlusal Considerations in ImplantDocument11 pagesOcclusal Considerations in ImplantRolzilah RohaniNo ratings yet
- Hinge Axis: Presenter B.Alekhya Iiyrpg Moderator Dr. KamalDocument80 pagesHinge Axis: Presenter B.Alekhya Iiyrpg Moderator Dr. Kamalbharathi krishnaNo ratings yet
- Retention in Maxillofacial Prosthesis: A Literature ReviewDocument9 pagesRetention in Maxillofacial Prosthesis: A Literature ReviewIJAR JOURNALNo ratings yet
- 6.clinical Case ReportMultidisciplinary Approach For Rehabilitation of Debilitated Anterior ToothDocument6 pages6.clinical Case ReportMultidisciplinary Approach For Rehabilitation of Debilitated Anterior ToothSahana RangarajanNo ratings yet
- ACR Channel AMCDocument40 pagesACR Channel AMCVikram ReddyNo ratings yet
- Different Types of Tooth PreparationDocument56 pagesDifferent Types of Tooth PreparationSahana Rangarajan100% (1)
- Single Complete Denture FinalDocument15 pagesSingle Complete Denture FinalVikas AggarwalNo ratings yet
- Occlusion in Complete DentureDocument57 pagesOcclusion in Complete DentureSahana Rangarajan100% (1)
- Stresses Induced by Removoble Partial DentureDocument85 pagesStresses Induced by Removoble Partial DentureSimran Sahni100% (2)
- The Complete Guide to Dental Implants: All About DentistryFrom EverandThe Complete Guide to Dental Implants: All About DentistryNo ratings yet
- Notice - Return To WorkDocument2 pagesNotice - Return To WorkJhony Martin Alba100% (1)
- Clinical Cases in Restorative and Reconstructive DentistryFrom EverandClinical Cases in Restorative and Reconstructive DentistryRating: 5 out of 5 stars5/5 (1)
- Cami OriginalDocument22 pagesCami OriginalSantiago OsorioNo ratings yet
- Articulators PDFDocument30 pagesArticulators PDFAhmed M. Nageeb100% (1)
- Hobos PhilosophyDocument190 pagesHobos Philosophysapna100% (1)
- A Clinical Overview of Removable Prostheses - Introduction 1.factors To Consider in Planning A Removable Partial DentureDocument6 pagesA Clinical Overview of Removable Prostheses - Introduction 1.factors To Consider in Planning A Removable Partial DentureCristi PapandopolNo ratings yet
- Basic Principles of Obturator Design For Partially Edentulous Patients. Part I: ClassificationDocument69 pagesBasic Principles of Obturator Design For Partially Edentulous Patients. Part I: ClassificationDrFarha NazNo ratings yet
- Restoration of The Worn Dentition. Part 2Document7 pagesRestoration of The Worn Dentition. Part 2Isharajini Prasadika Subhashni GamageNo ratings yet
- Clinical Success in Resin Bonded Bridges PDFDocument7 pagesClinical Success in Resin Bonded Bridges PDFNajeeb UllahNo ratings yet
- Cu Sil DenturesDocument6 pagesCu Sil Denturessiddu76No ratings yet
- Project Augustine AbisolaDocument59 pagesProject Augustine AbisolaRoseline Omoare100% (1)
- Prosthodontics Book ListDocument3 pagesProsthodontics Book ListDentist Here100% (1)
- Support in Complete DentureDocument30 pagesSupport in Complete DentureSahana Rangarajan100% (2)
- Full Mouth Rehabilitation: A Smooth Pathway For Complex JourneyDocument8 pagesFull Mouth Rehabilitation: A Smooth Pathway For Complex JourneySkAliHassanNo ratings yet
- ObturatorsDocument79 pagesObturatorsPremshith CpNo ratings yet
- Apta Lab Values Resource 2013Document3 pagesApta Lab Values Resource 2013api-293223028No ratings yet
- Single DentureDocument37 pagesSingle DentureDentist Dina SamyNo ratings yet
- The Osteoperiosteal Flap: A Simplified Approach to Alveolar Bone ReconstructionFrom EverandThe Osteoperiosteal Flap: A Simplified Approach to Alveolar Bone ReconstructionRating: 4 out of 5 stars4/5 (1)
- Intraoral Gothic Arch Tracing PDFDocument5 pagesIntraoral Gothic Arch Tracing PDFSamuel Flores CalderonNo ratings yet
- Open-Bite Malocclusion: Treatment and StabilityFrom EverandOpen-Bite Malocclusion: Treatment and StabilityGuilherme JansonRating: 5 out of 5 stars5/5 (1)
- Section 006 Incisal GuidanceDocument14 pagesSection 006 Incisal GuidanceAmar BhochhibhoyaNo ratings yet
- OVERDENTURESDocument15 pagesOVERDENTURESAditya SavirmathNo ratings yet
- Occlusion in Complete DentureDocument64 pagesOcclusion in Complete Denturepuja singhNo ratings yet
- Retainers in FPDDocument153 pagesRetainers in FPDAmit Bhargav88% (8)
- Spacer DesignDocument44 pagesSpacer Designyabhatia100% (1)
- Occlusion For Fixed Prosthodontics - Final PDFDocument16 pagesOcclusion For Fixed Prosthodontics - Final PDFdrgayen6042No ratings yet
- Fixed Prosthodontics - Types of Dental Bridges (FPD)Document22 pagesFixed Prosthodontics - Types of Dental Bridges (FPD)Jessa Mae FerolinoNo ratings yet
- CV Mrunal-Doiphode Some WebsiteDocument3 pagesCV Mrunal-Doiphode Some WebsiteMrunal DoiphodeNo ratings yet
- OverdentureDocument227 pagesOverdentureEazhil RajNo ratings yet
- Prostho Lec - OverdenturesDocument14 pagesProstho Lec - Overdenturesdrgayen6042No ratings yet
- Restoration of THE Endodonticall Y Treated Tooth: Amith Babu Amrita Dora Ganesh O.R Praveen J Ourvind SinghDocument100 pagesRestoration of THE Endodonticall Y Treated Tooth: Amith Babu Amrita Dora Ganesh O.R Praveen J Ourvind SinghCahyani CahyaniNo ratings yet
- Dynamic Navigation in Dental Implantology: The Influence of Surgical Experience On Implant Placement Accuracy and Operating Time. An in Vitro StudyDocument9 pagesDynamic Navigation in Dental Implantology: The Influence of Surgical Experience On Implant Placement Accuracy and Operating Time. An in Vitro StudySahana RangarajanNo ratings yet
- Support in Complete DentureDocument16 pagesSupport in Complete DentureSahana RangarajanNo ratings yet
- 7 Shreeprada Dash IJPHRDDecember 2018 IssueDocument7 pages7 Shreeprada Dash IJPHRDDecember 2018 IssueSahana RangarajanNo ratings yet
- Clinical Report Rehabilitation of Maxillary Surgical Defect With A Cast Partial Denture ObturatorDocument4 pagesClinical Report Rehabilitation of Maxillary Surgical Defect With A Cast Partial Denture ObturatorSahana RangarajanNo ratings yet
- Finishing and Polishing Agents: - Presented by DR Arpita DuttaDocument89 pagesFinishing and Polishing Agents: - Presented by DR Arpita DuttaSahana RangarajanNo ratings yet
- Factors Affecting Shade of All Ceramic Restorations - A Literature ReviewDocument8 pagesFactors Affecting Shade of All Ceramic Restorations - A Literature ReviewSahana RangarajanNo ratings yet
- Fulltext - Jda v5 Id1107Document3 pagesFulltext - Jda v5 Id1107Sahana RangarajanNo ratings yet
- Long-Term Follow-Up of Maxillary Fixed Retention: Survival Rate and Periodontal HealthDocument7 pagesLong-Term Follow-Up of Maxillary Fixed Retention: Survival Rate and Periodontal HealthSahana RangarajanNo ratings yet
- A Hollow Bulb Obturator For Maxillary Resection in A Completely Edentulous PatientDocument6 pagesA Hollow Bulb Obturator For Maxillary Resection in A Completely Edentulous PatientSahana RangarajanNo ratings yet
- Significance of Facebow For Dental RestorationsDocument5 pagesSignificance of Facebow For Dental RestorationsSahana RangarajanNo ratings yet
- Mouth Guards in Dentistry-A Review: September 2018Document6 pagesMouth Guards in Dentistry-A Review: September 2018Sahana RangarajanNo ratings yet
- Prosthodontics Horizontal Jaw Relation: Dr. Firas AbdulameerDocument6 pagesProsthodontics Horizontal Jaw Relation: Dr. Firas AbdulameerSahana RangarajanNo ratings yet
- Elegant Galaxy Background Breakthrough by SlidesgoDocument48 pagesElegant Galaxy Background Breakthrough by SlidesgoSahana RangarajanNo ratings yet
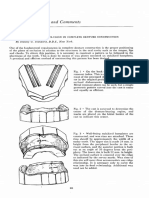
- Cases and Comments: by Stanley G. Standard, D.D.S., New YorkDocument3 pagesCases and Comments: by Stanley G. Standard, D.D.S., New YorkSahana RangarajanNo ratings yet
- Sauser 1957Document9 pagesSauser 1957Sahana RangarajanNo ratings yet
- Gothic Arch TrachingDocument7 pagesGothic Arch TrachingSahana RangarajanNo ratings yet
- Literature Review On Consumer AttitudeDocument8 pagesLiterature Review On Consumer Attitudeaflspyogf100% (1)
- Till June Zedc ExpiryDocument15 pagesTill June Zedc ExpiryRahul DhawaleNo ratings yet
- Article 1593160469Document6 pagesArticle 1593160469kirtiNo ratings yet
- Mapeh - P.E. 6: First Quarter-Module 3 Topic: Skills Involved in Playing GamesDocument8 pagesMapeh - P.E. 6: First Quarter-Module 3 Topic: Skills Involved in Playing GamesNICOLE ALANA100% (1)
- Affidavit of UndertakingDocument2 pagesAffidavit of Undertakingallan babadNo ratings yet
- Common Course Outline For: EXSC 2305 Exercise Physiology A. Course DescriptionDocument2 pagesCommon Course Outline For: EXSC 2305 Exercise Physiology A. Course DescriptionZedy GullesNo ratings yet
- HypospadiasDocument11 pagesHypospadiasmustikaweniNo ratings yet
- Organizational Behavior: Managing YourselfDocument18 pagesOrganizational Behavior: Managing YourselfKavita VermaNo ratings yet
- DT - UM - Q Manual Dexxum TDocument48 pagesDT - UM - Q Manual Dexxum TScribdTranslationsNo ratings yet
- AFFECTIVE TARGETS: AttitudeDocument19 pagesAFFECTIVE TARGETS: AttitudeJaika SedoroNo ratings yet
- Lesson PlanDocument45 pagesLesson PlanHarman GillNo ratings yet
- Lab On AssertivenessDocument6 pagesLab On AssertivenessPooja VarmaNo ratings yet
- 1179 ID Pengaruh Keselamatan Dan Kesehatan Kerja Terhadap Kinerja Karyawan Studi Pada deDocument11 pages1179 ID Pengaruh Keselamatan Dan Kesehatan Kerja Terhadap Kinerja Karyawan Studi Pada deAhmad RifaiNo ratings yet
- A Study To Assess The Effectiveness of Interventional Module On Stress Levels Among Infertile Women Attending Infertility Clinics of Selected Hospitals at BagalkotDocument8 pagesA Study To Assess The Effectiveness of Interventional Module On Stress Levels Among Infertile Women Attending Infertility Clinics of Selected Hospitals at BagalkotInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Concept Paper B3 SinagTalaDocument8 pagesConcept Paper B3 SinagTalaVenice De los ReyesNo ratings yet
- Learning Guide No 2Document23 pagesLearning Guide No 2henokNo ratings yet
- Oxygen, Compressed: Safety Data SheetDocument9 pagesOxygen, Compressed: Safety Data SheetRianAwanggaNo ratings yet
- Medical Nutrition Therapy A Case Study Approach 5Th Edition Nelms Solutions Manual Full Chapter PDFDocument29 pagesMedical Nutrition Therapy A Case Study Approach 5Th Edition Nelms Solutions Manual Full Chapter PDFStephanieMckayeqwr100% (8)
- Familymedicine Revisedcurriculumfinaldraft November2020Document85 pagesFamilymedicine Revisedcurriculumfinaldraft November2020Opubo BrownNo ratings yet
- Concept of CurriculumDocument81 pagesConcept of CurriculumtalentNo ratings yet
- Paulo C. Campos: (July 7, 1921 - June 2, 2007)Document3 pagesPaulo C. Campos: (July 7, 1921 - June 2, 2007)NanceNo ratings yet
- Chen 2021Document13 pagesChen 2021Aitor UzkudunNo ratings yet