You might also like
- Chemicals Can: Safe Handling of ChemicalsDocument1 pageChemicals Can: Safe Handling of ChemicalsJavier Quintero SaavedraNo ratings yet
- HSE Slides For PresentationDocument4 pagesHSE Slides For PresentationpjosesmNo ratings yet
- Safety Orientation: Rigging Equipment Engineering ON 24 SEPTEMBER 2017Document11 pagesSafety Orientation: Rigging Equipment Engineering ON 24 SEPTEMBER 2017Hse DepartmenNo ratings yet
- Dust PostersDocument5 pagesDust PostersAli MohdNo ratings yet
- 3 Lecture 2 N 3-1 Fundamentals of SafetyDocument29 pages3 Lecture 2 N 3-1 Fundamentals of SafetyArjan GhoshNo ratings yet
- Basic Safety AwarenessDocument12 pagesBasic Safety AwarenessAkuabataNo ratings yet
- Machinery Safety CheckDocument3 pagesMachinery Safety CheckYuva samaj sewa TrustNo ratings yet
- Evaluation of Camp OHS Risks AssessmentDocument3 pagesEvaluation of Camp OHS Risks Assessmenthasanhse640No ratings yet
- OSHA Environmental Controls Subpart D - Medical, Sanitation, Noise, RadiationDocument2 pagesOSHA Environmental Controls Subpart D - Medical, Sanitation, Noise, RadiationJohn Vem BansagNo ratings yet
- 0I. Accident Causes and PreventionDocument52 pages0I. Accident Causes and PreventionGregor CleganeNo ratings yet
- HSE Manual Unlimited EnergyDocument74 pagesHSE Manual Unlimited Energysangar sabirNo ratings yet
- Safety ProceduresDocument7 pagesSafety ProceduresRuwan MadhushankaNo ratings yet
- Noise & Vibration Learning OutcomesDocument45 pagesNoise & Vibration Learning OutcomesRoshan RajasNo ratings yet
- First Aid & BLS 2Document23 pagesFirst Aid & BLS 2Nate JulongbayanNo ratings yet
- Installation & Safety Guide for Waste Compactors & Recycling SystemsDocument21 pagesInstallation & Safety Guide for Waste Compactors & Recycling SystemsVuong BuiNo ratings yet
- Inspection Procedure: Grillon LanyardDocument5 pagesInspection Procedure: Grillon LanyardUlviyye ElesgerovaNo ratings yet
- Positif Jsa HMCFDDocument4 pagesPositif Jsa HMCFDBryant TorresNo ratings yet
- Rajda Industries & Exports Pvt. LTD Fire Safety Checklist SA8000:2014Document6 pagesRajda Industries & Exports Pvt. LTD Fire Safety Checklist SA8000:2014AVISEK GHOSHNo ratings yet
- HSE Safety AuditsDocument3 pagesHSE Safety Auditsvlad100% (1)
- ERT Team Management & Emergency Evacuation ProcedureDocument23 pagesERT Team Management & Emergency Evacuation ProcedureAsif Jamil ChowdhuryNo ratings yet
- EHS Manual - EngDocument149 pagesEHS Manual - EngEduardo GarzaNo ratings yet
- COVID-19 Table-Top Information PDFDocument143 pagesCOVID-19 Table-Top Information PDFigor_239934024No ratings yet
- 1 EvacuationGuideDocument17 pages1 EvacuationGuideEmine GençNo ratings yet
- Amrut Sop Book FinalDocument32 pagesAmrut Sop Book FinalLord KrsnikNo ratings yet
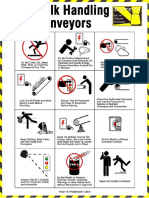
- Conveyor safety guideDocument7 pagesConveyor safety guideazim kazi100% (1)
- Inspection ChecklistDocument78 pagesInspection ChecklistEfari BahchevanNo ratings yet
- Pest ControlDocument3 pagesPest ControldeshankarunarathneNo ratings yet
- Noise MonitoringDocument1 pageNoise MonitoringSAMEER JAVEDNo ratings yet
- Employee Orientation Checklist Areas To Be Covered Description CompletedDocument2 pagesEmployee Orientation Checklist Areas To Be Covered Description Completedeast100% (1)
- MSDS Cement PDFDocument5 pagesMSDS Cement PDFHendrik SimatupangNo ratings yet
- Radiation Types, Effects and ControlsDocument34 pagesRadiation Types, Effects and ControlsRoshan Rajas100% (1)
- Procedure Accident RepDocument12 pagesProcedure Accident RepSanatan PanigrahiNo ratings yet
- Welcome To Emarat: Heat StressDocument19 pagesWelcome To Emarat: Heat StressSYED NEYAZ AHMADNo ratings yet
- Pest Control Risk Assessment Indoor and OutdoorDocument72 pagesPest Control Risk Assessment Indoor and OutdoorarmkarthickNo ratings yet
- Field Level Risk Assessment Manager’s HandbookDocument31 pagesField Level Risk Assessment Manager’s HandbookAaquil RaziNo ratings yet
- Grinding Wheel ReplacementDocument2 pagesGrinding Wheel ReplacementAshok Suresh100% (1)
- H2S Safety Program SummaryDocument5 pagesH2S Safety Program SummaryomarNo ratings yet
- Exide: Refno.: Eil/Sec/2023-24/32Document42 pagesExide: Refno.: Eil/Sec/2023-24/32Javed KhanNo ratings yet
- Commercial Electrical Inspection ChecklistsDocument1 pageCommercial Electrical Inspection ChecklistsRao UmarNo ratings yet
- Safety With Asbestos - Information SheetDocument4 pagesSafety With Asbestos - Information SheetAli MohdNo ratings yet
- Discharge Standards For DubaiDocument6 pagesDischarge Standards For DubaiHRK65No ratings yet
- Effluent Discharge Mock Emergency and Evalaution ReportDocument3 pagesEffluent Discharge Mock Emergency and Evalaution Reportremember0% (1)
- UAE Law No. - 21 - of 2005 Concerning Waste Management in Abu Dhabi Emirate EngDocument9 pagesUAE Law No. - 21 - of 2005 Concerning Waste Management in Abu Dhabi Emirate EngwholenumberNo ratings yet
- Elevated Work Rev.Document40 pagesElevated Work Rev.Anthony BasantaNo ratings yet
- OSHA Noise StandardDocument4 pagesOSHA Noise StandardDhaval MistryNo ratings yet
- 0400E-CHB - Sulfuric AcidDocument1 page0400E-CHB - Sulfuric AcidVeralord De VeraNo ratings yet
- FR - HSE - 061 - en Permit To Work Audit ChecklistDocument2 pagesFR - HSE - 061 - en Permit To Work Audit ChecklistNibu P ShajiNo ratings yet
- Permit To Work Form WordDocument1 pagePermit To Work Form WordMohamed ElnagdyNo ratings yet
- Hatching EggDocument19 pagesHatching EggPoultry HubNo ratings yet
- Chemical and MSDS RegisterDocument5 pagesChemical and MSDS RegisterRhen HalfferzrheinsNo ratings yet
- OSHA 511 Sub I PPEDocument33 pagesOSHA 511 Sub I PPEAhmed Hassan SabryNo ratings yet
- Daily HSEReport FormatDocument7 pagesDaily HSEReport Formatsufiyan sskNo ratings yet
- SHE Appointment PosterDocument1 pageSHE Appointment PosterVictorNo ratings yet
- Confined Spaces CardsDocument1 pageConfined Spaces CardsJafar KhanNo ratings yet
- Brand Analysis India Private Limited Risk Assessment: Risk Risk Impact C I A Risk Value Threat Miltigation PlanDocument2 pagesBrand Analysis India Private Limited Risk Assessment: Risk Risk Impact C I A Risk Value Threat Miltigation PlanTrivesh SNo ratings yet
- Risk Assessment TunnelDocument2 pagesRisk Assessment TunnelShauna LaycockNo ratings yet
- Integr Ted Business Re S: at SourceDocument14 pagesIntegr Ted Business Re S: at SourcecyclopsoctopusNo ratings yet
- Safety InspectionDocument45 pagesSafety InspectionKladees WorldNo ratings yet
- 7 Respiratory Protection July2014Document1 page7 Respiratory Protection July2014joker batmanNo ratings yet
- 4.4.2.4B General OHS Induction VisitorsDocument2 pages4.4.2.4B General OHS Induction VisitorsSeeiso MasienyaneNo ratings yet
- Physical Therapy Initial Evaluation Form: Patient InformationDocument2 pagesPhysical Therapy Initial Evaluation Form: Patient InformationPraveenkumar CrNo ratings yet
- Concerto Piano Violon Bwv1041 No2 Violon - J.S BachDocument2 pagesConcerto Piano Violon Bwv1041 No2 Violon - J.S Bachcontrax8No ratings yet
- Concerto Piano Violon Bwv1041 No2 Violon - J.S BachDocument2 pagesConcerto Piano Violon Bwv1041 No2 Violon - J.S Bachcontrax8No ratings yet
- Phalaborwa - ZBS Upgrade ProjectDocument2 pagesPhalaborwa - ZBS Upgrade Projectcontrax8100% (1)
- Phalaborwa - ZBS Upgrade ProjectDocument3 pagesPhalaborwa - ZBS Upgrade Projectcontrax8No ratings yet
- Phalaborwa - ZBS Upgrade Project S&D ConsortiumDocument2 pagesPhalaborwa - ZBS Upgrade Project S&D Consortiumcontrax8No ratings yet
- Phalaborwa - ZBS Upgrade ProjectDocument3 pagesPhalaborwa - ZBS Upgrade Projectcontrax8No ratings yet
- Phalaborwa - ZBS Upgrade ProjectDocument3 pagesPhalaborwa - ZBS Upgrade Projectcontrax8No ratings yet
- Phalaborwa - ZBS Upgrade Project S&D ConsortiumDocument2 pagesPhalaborwa - ZBS Upgrade Project S&D Consortiumcontrax8No ratings yet
- Phalaborwa - ZBS Upgrade Project S&D ConsortiumDocument2 pagesPhalaborwa - ZBS Upgrade Project S&D Consortiumcontrax8No ratings yet
- Phalaborwa - ZBS Upgrade ProjectDocument3 pagesPhalaborwa - ZBS Upgrade Projectcontrax8No ratings yet
- Sop OPOP - 050 - Breath Analyser, Alcohol and DrugsDocument5 pagesSop OPOP - 050 - Breath Analyser, Alcohol and Drugscontrax8100% (1)
- Phalaborwa - ZBS Upgrade Project S&D ConsortiumDocument2 pagesPhalaborwa - ZBS Upgrade Project S&D Consortiumcontrax8No ratings yet
- Phalaborwa - ZBS Upgrade ProjectDocument3 pagesPhalaborwa - ZBS Upgrade Projectcontrax8No ratings yet
- Phalaborwa - ZBS Upgrade Project S&D ConsortiumDocument2 pagesPhalaborwa - ZBS Upgrade Project S&D Consortiumcontrax8No ratings yet
- Phalaborwa - ZBS Upgrade Project S&D ConsortiumDocument2 pagesPhalaborwa - ZBS Upgrade Project S&D Consortiumcontrax8No ratings yet
- Phalaborwa - ZBS Upgrade Project S&D ConsortiumDocument2 pagesPhalaborwa - ZBS Upgrade Project S&D Consortiumcontrax8No ratings yet
- SHEQ Systems ProceduresDocument26 pagesSHEQ Systems Procedurescontrax8No ratings yet
- Sop OPOP Eng 007 - Operating Diesel Bowsers and TanksDocument8 pagesSop OPOP Eng 007 - Operating Diesel Bowsers and Tankscontrax8100% (1)
- Sop OPOP - 078 - Control Room Call-Out ProcedureDocument4 pagesSop OPOP - 078 - Control Room Call-Out Procedurecontrax8No ratings yet
- C-SMS-4.2. PolicyDocument4 pagesC-SMS-4.2. Policycontrax8No ratings yet
- Sop OPOP - 013 - Sewage DisposalDocument5 pagesSop OPOP - 013 - Sewage Disposalcontrax8No ratings yet
- Preventing Contraband in Blast AreasDocument6 pagesPreventing Contraband in Blast Areascontrax8No ratings yet
- Safety, Health and Environmental Manual: Safe Work Procedure - BlankDocument1 pageSafety, Health and Environmental Manual: Safe Work Procedure - Blankcontrax8No ratings yet
- C-SMS-4.4.3.2. - Participation and ConsultationDocument4 pagesC-SMS-4.4.3.2. - Participation and Consultationcontrax8No ratings yet
- C-SMS-4.3.1.5 Management of ChangeDocument8 pagesC-SMS-4.3.1.5 Management of Changecontrax8No ratings yet
- C-SMS-4.4.3.1. - CommunicationDocument5 pagesC-SMS-4.4.3.1. - Communicationcontrax8No ratings yet
- SAFETY MANAGEMENT ROLESDocument7 pagesSAFETY MANAGEMENT ROLEScontrax8No ratings yet
- C-SMS-4.3.2. Legal & Other RequirementsDocument4 pagesC-SMS-4.3.2. Legal & Other Requirementscontrax8No ratings yet
- Health Assessment Reveals Stomach Cancer RiskDocument4 pagesHealth Assessment Reveals Stomach Cancer RiskKurt DanielNo ratings yet
- Drop Foot, An Unexpected Complication of Vaginal HysterectomyDocument4 pagesDrop Foot, An Unexpected Complication of Vaginal HysterectomySandraSaracNo ratings yet
- Screenshot 2023-09-03 at 1.27.00 AMDocument8 pagesScreenshot 2023-09-03 at 1.27.00 AMhuzaifaawais27No ratings yet
- DSS AIIMS OBG Practice TestDocument13 pagesDSS AIIMS OBG Practice TestDr-Sanjay SinghaniaNo ratings yet
- TOLC 2016-2017 Enrollment Form PDFDocument3 pagesTOLC 2016-2017 Enrollment Form PDFAnonymous C11nDANo ratings yet
- Masseter Muscle Reattachment After Mandibular Angle SurgeryDocument4 pagesMasseter Muscle Reattachment After Mandibular Angle Surgery洪侊增No ratings yet
- Pharmacological Management of Cardiac Arrhythmias in The Fetal andDocument16 pagesPharmacological Management of Cardiac Arrhythmias in The Fetal andcristhian mendezNo ratings yet
- How To Do Kegel Exercises PDFDocument2 pagesHow To Do Kegel Exercises PDFAyu Maindra100% (1)
- Causes, Incidence, and Risk Factors: Hepatitis A Hepatitis C Hepatitis DDocument41 pagesCauses, Incidence, and Risk Factors: Hepatitis A Hepatitis C Hepatitis DAmber ShrivastavaNo ratings yet
- Nursing Reflection on the Importance of ResearchDocument1 pageNursing Reflection on the Importance of ResearchXye Cinches AlberastineNo ratings yet
- Point Lift - Point Lift - Point - Point - Point - Point: A Clinician's Guide ToDocument13 pagesPoint Lift - Point Lift - Point - Point - Point - Point: A Clinician's Guide TovictoriaNo ratings yet
- The Charcot Foot. The British Editorial Society of Bone & Joint Surgery. 2016Document5 pagesThe Charcot Foot. The British Editorial Society of Bone & Joint Surgery. 2016Jose Fernando DiezNo ratings yet
- Mental HygieneDocument18 pagesMental Hygienechester chesterNo ratings yet
- Antiviral and Anti-Fungal DrugsDocument8 pagesAntiviral and Anti-Fungal DrugsAhmed HadeerNo ratings yet
- PonstanDocument5 pagesPonstan--bolabolaNo ratings yet
- CT - Week 16Document3 pagesCT - Week 16PAOLA LUZ CRUZNo ratings yet
- Digital Healthcare Data - Electronic Medical Records for Improved Patient OutcomesDocument18 pagesDigital Healthcare Data - Electronic Medical Records for Improved Patient Outcomesbpk riNo ratings yet
- Clinical Nutrition in Gerontology: Chronic Renal Disorders of The Dog and CatDocument8 pagesClinical Nutrition in Gerontology: Chronic Renal Disorders of The Dog and CatKhairul Ihsan Pengusaha MudaNo ratings yet
- Sids PresentationDocument10 pagesSids Presentationapi-257403826No ratings yet
- May 20151Document17 pagesMay 20151Hany Rasheed Mohamed50% (2)
- Association Between Mir Let-7g Gene Expression and The Risk of Cervical Cancer in Human Papilloma Virus-Infected PatientsDocument8 pagesAssociation Between Mir Let-7g Gene Expression and The Risk of Cervical Cancer in Human Papilloma Virus-Infected PatientsGICELANo ratings yet
- Set v. Care of Clients With Physiologic and Psychosocial Alterations C (Answers)Document11 pagesSet v. Care of Clients With Physiologic and Psychosocial Alterations C (Answers)Yaj CruzadaNo ratings yet
- Outpatient Programs - Adult Rehabilitation Island HealthDocument8 pagesOutpatient Programs - Adult Rehabilitation Island HealthCorey Jay ParkerNo ratings yet
- Meddra Coding: - Jhansi BogoluDocument18 pagesMeddra Coding: - Jhansi BogolujhansiNo ratings yet
- Dosage Form ExamDocument9 pagesDosage Form ExamsongaNo ratings yet
- PERIOPERATIVE NURSING OVERVIEWDocument93 pagesPERIOPERATIVE NURSING OVERVIEWJoel Santos100% (1)
- RadioDocument4 pagesRadioSawsan Z. JwaiedNo ratings yet
- Pediatrics Drugs-1Document3 pagesPediatrics Drugs-1seemahasheesh93No ratings yet
- The Perfect ClerkDocument3 pagesThe Perfect ClerkKrystel BatinoNo ratings yet
- Renal Replacement Therapy LectureDocument26 pagesRenal Replacement Therapy Lectureadwait marhattaNo ratings yet