You might also like
- Pharmacy Calculation Workbook: 250 Questions to Prepare for the NAPLEX and PTCB ExamFrom EverandPharmacy Calculation Workbook: 250 Questions to Prepare for the NAPLEX and PTCB ExamRating: 5 out of 5 stars5/5 (1)
- Common ICU DripsDocument1 pageCommon ICU DripsSunshine Willis100% (2)
- Drug Infusions in ICU Made Simple 2016 by MansdocsDocument28 pagesDrug Infusions in ICU Made Simple 2016 by Mansdocsabdullah almatary0% (1)
- London Cancer Methylene Blue Guideline v1Document5 pagesLondon Cancer Methylene Blue Guideline v1Tan Wei Lin33% (3)
- EDP Mitotane Protocol V1.0Document8 pagesEDP Mitotane Protocol V1.0Andrei BuruianăNo ratings yet
- R-Codox M: Patients With Good Performance StatusDocument6 pagesR-Codox M: Patients With Good Performance StatusALEXANDER AVILANo ratings yet
- EC-DH Epirubicin Cyclophosphamide Followed by Docetaxel With Trastuzumab Protocol V1.1Document11 pagesEC-DH Epirubicin Cyclophosphamide Followed by Docetaxel With Trastuzumab Protocol V1.1smokkerNo ratings yet
- Sumup Toxi OsDocument21 pagesSumup Toxi OsSelma MutiaraNo ratings yet
- GCC Anti Emetic Guidelines 2003Document2 pagesGCC Anti Emetic Guidelines 2003damondouglasNo ratings yet
- Obat UKMPPDDocument54 pagesObat UKMPPDMuh.ikhsan zainalNo ratings yet
- BFM 2000 Treatment SchemaDocument2 pagesBFM 2000 Treatment SchemaAnonymous 9dVZCnTXSNo ratings yet
- (Sumber: NHL-BFM 90 Protokol) : Anaplastic Large-Cell Lymphoma ProtocolDocument6 pages(Sumber: NHL-BFM 90 Protokol) : Anaplastic Large-Cell Lymphoma ProtocolFandi ArgiansyaNo ratings yet
- Dilution FormulaDocument2 pagesDilution FormulaFazilah ShahromNo ratings yet
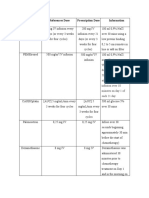
- Drugs Name References Dose Prescription Dose InformationDocument2 pagesDrugs Name References Dose Prescription Dose InformationSanithaaaNo ratings yet
- Antibiotik: Dosis Nama Dagang Sediaan Keterangan Anak Dewasa AmoxicilinDocument6 pagesAntibiotik: Dosis Nama Dagang Sediaan Keterangan Anak Dewasa AmoxicilinaandhiiraaNo ratings yet
- Dosis Obat EmergencyDocument1 pageDosis Obat EmergencyCharida IrawanNo ratings yet
- Case Parade Dr. Wella - ITADocument8 pagesCase Parade Dr. Wella - ITAFADHILA SANDYNo ratings yet
- Komposisi Dosis Nama Obat: AntibiotikaDocument12 pagesKomposisi Dosis Nama Obat: Antibiotikahilman fauzanNo ratings yet
- Nursing Cheat SheetDocument1 pageNursing Cheat Sheetramesh kumarNo ratings yet
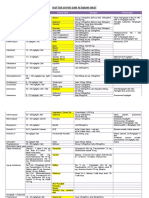
- Daftar Dosis Dan Sediaan ObatDocument7 pagesDaftar Dosis Dan Sediaan Obatdoru ubungNo ratings yet
- Pallia NotesDocument8 pagesPallia NotesStella ApaNo ratings yet
- Pallia NotesDocument8 pagesPallia NotesStella ApaNo ratings yet
- RBHSC Paediatric Drug Calculator V2.7 LockedDocument2 pagesRBHSC Paediatric Drug Calculator V2.7 LockedAhmed IsmailNo ratings yet
- Drugs and Dosage Drugs and Dosage: Atropine Sulfate 1Mg/MlDocument3 pagesDrugs and Dosage Drugs and Dosage: Atropine Sulfate 1Mg/MlIna RamosNo ratings yet
- Cyclophosphamide (Cyclovid) - Epirubicin - VincristineDocument1 pageCyclophosphamide (Cyclovid) - Epirubicin - VincristineEma Ratna KartinawatiNo ratings yet
- SedationDocument1 pageSedationratnamalaramasamyNo ratings yet
- Asthama Copd DosesDocument4 pagesAsthama Copd DosesAymen BekirNo ratings yet
- CALGB Schema FinalDocument1 pageCALGB Schema FinalMohamed MahmoudNo ratings yet
- Jpho 2019 02 07 Resham Jpho-18-291r sdc1Document1 pageJpho 2019 02 07 Resham Jpho-18-291r sdc1Naman KhalidNo ratings yet
- Primary Therapy-Chronic Smoldering: ContinuedDocument2 pagesPrimary Therapy-Chronic Smoldering: ContinuedYuliana Eka RusdiyantiNo ratings yet
- Pdrugs Print 1-1Document26 pagesPdrugs Print 1-1Endah SetyaningsihNo ratings yet
- Computation FormulasDocument1 pageComputation FormulasNicole cuencosNo ratings yet
- Paclitaxel With EC Adjuvant or Neoadjuvant Protocol V1.1Document7 pagesPaclitaxel With EC Adjuvant or Neoadjuvant Protocol V1.1smokkerNo ratings yet
- ABVD (Hodgkin's Lymphoma) : IV InfusionDocument4 pagesABVD (Hodgkin's Lymphoma) : IV InfusionSindu SankarNo ratings yet
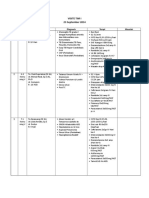
- Visite Tim I 23 Sep-1Document3 pagesVisite Tim I 23 Sep-1Frans JobethNo ratings yet
- Drug Therapy For PicuDocument32 pagesDrug Therapy For PicuNeethu Mariya MathewNo ratings yet
- Antibiotik: Generik Nama Paten Indikasi Dosis Bumil As. Clavulanat + AmoxycillinDocument8 pagesAntibiotik: Generik Nama Paten Indikasi Dosis Bumil As. Clavulanat + AmoxycillinVeve PujiNo ratings yet
- Drug Amount of Drug Diluted To 50ml 1ml/hr Dose Range: Picu Drug Infusion ChartDocument1 pageDrug Amount of Drug Diluted To 50ml 1ml/hr Dose Range: Picu Drug Infusion ChartIndria febriani0% (1)
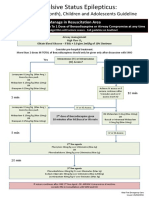
- Status Epilepticus A3v2Document1 pageStatus Epilepticus A3v2afalfitraNo ratings yet
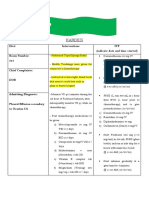
- Kardex: Diet: Interventions IVF (Indicate Date and Time Started) Room Number: 313Document2 pagesKardex: Diet: Interventions IVF (Indicate Date and Time Started) Room Number: 313kuro hanabusaNo ratings yet
- Daftar Dosis Dan Sediaan Obat AnakDocument4 pagesDaftar Dosis Dan Sediaan Obat AnaklayaliaNo ratings yet
- 24 Feb 24 Distribusi Pasien Visite Besar Ilmu Bedah FK ULMDocument11 pages24 Feb 24 Distribusi Pasien Visite Besar Ilmu Bedah FK ULMWildan'z CreedNo ratings yet
- Rotor SpinningDocument14 pagesRotor SpinningAnindya GhoshNo ratings yet
- Drugs by Dr.i̇brahim Taha &DR - Khald BadrDocument10 pagesDrugs by Dr.i̇brahim Taha &DR - Khald BadrAya HagagNo ratings yet
- Paediatric Critical Care Infusions Intubation DrugsDocument2 pagesPaediatric Critical Care Infusions Intubation DrugsА. Сосорбарам100% (1)
- Drug Dosages KTHDocument20 pagesDrug Dosages KTHQazi Saadullah LatifNo ratings yet
- DRIPSDocument7 pagesDRIPSKim Alvarez100% (2)
- Pre-Operative Orders Post-Op Orders (Ga)Document3 pagesPre-Operative Orders Post-Op Orders (Ga)Alissandra OcampoNo ratings yet
- Input Data Project Job Refrence Rev. Client Prep'd Title DateDocument25 pagesInput Data Project Job Refrence Rev. Client Prep'd Title DateImran KhanNo ratings yet
- SopDocument7 pagesSopAryo WibisonoNo ratings yet
- نسخة Infusion rate of emergency drugsDocument4 pagesنسخة Infusion rate of emergency drugsMohammed FathiNo ratings yet
- No. Identitas Diagnosis R. Tindakan Terapi DPJPDocument4 pagesNo. Identitas Diagnosis R. Tindakan Terapi DPJPjuita surbaktiNo ratings yet
- Hodgkin Lymphoma RegimensDocument5 pagesHodgkin Lymphoma RegimensLuana MNo ratings yet
- Adrenaline Infusion - Dopamine - OthersDocument1 pageAdrenaline Infusion - Dopamine - OthersMahmoud ismailNo ratings yet
- DrugsDocument4 pagesDrugsShirmayne TangNo ratings yet
- Paclitaxel Trastuzumab Breast Cancer ProtocolDocument9 pagesPaclitaxel Trastuzumab Breast Cancer ProtocolsmokkerNo ratings yet
- Case Parade Ruangan - Dr. Valerinna Yogibuana, SP - JP (K)Document24 pagesCase Parade Ruangan - Dr. Valerinna Yogibuana, SP - JP (K)FADHILA SANDYNo ratings yet
- Mms-Diseases and ProtocolDocument8 pagesMms-Diseases and ProtocolWeb Any100% (1)
- جرعات الاطفالDocument50 pagesجرعات الاطفالWael Hamdy100% (1)
- Carboplatin With Pemetrexed Pembrolizumab Non Squamous Non-Small Cell Lung Cancer Protocol V1.1Document8 pagesCarboplatin With Pemetrexed Pembrolizumab Non Squamous Non-Small Cell Lung Cancer Protocol V1.1Olaru DianaNo ratings yet
- MappingDocument4 pagesMappingRina SyafritaNo ratings yet
- SSC Statements Sepsis Definitions 3 2016Document2 pagesSSC Statements Sepsis Definitions 3 2016Satbir SinghNo ratings yet
- SSC BundleDocument2 pagesSSC BundleFrancisco MañánNo ratings yet
- SSC BundleDocument2 pagesSSC BundleFrancisco MañánNo ratings yet
- Insulin Therapy For Type 2 DiabetesMellitusDocument11 pagesInsulin Therapy For Type 2 DiabetesMellitusJoseph TrevinoNo ratings yet
- Protokol SarcomaDocument4 pagesProtokol SarcomaHep PutNo ratings yet
- Methylene Blue - Pharmacokinetics and Organ Distribution of Intravenous and OralDocument4 pagesMethylene Blue - Pharmacokinetics and Organ Distribution of Intravenous and OralMari AprileNo ratings yet
- Presented by Andrew LamDocument20 pagesPresented by Andrew LamAndrew LamNo ratings yet
- IFOSFAMIDEDocument4 pagesIFOSFAMIDEErza GenatrikaNo ratings yet
- IfosfamideDocument4 pagesIfosfamideNurkholis AminNo ratings yet
- Chemotherapy ProtocolsDocument6 pagesChemotherapy ProtocolsDenny LukasNo ratings yet
- Mesna PM ENG v4.0 011218Document23 pagesMesna PM ENG v4.0 011218Vimal NishadNo ratings yet
- Holoxan Pi PDFDocument18 pagesHoloxan Pi PDFKarol IonasNo ratings yet
- Doxorubicin and Ifosfamide Sarcoma Protocol V1.0Document8 pagesDoxorubicin and Ifosfamide Sarcoma Protocol V1.0Joseph TrevinoNo ratings yet
- SAAI Protocol KankerDocument4 pagesSAAI Protocol KankerSadha MahardhikaNo ratings yet