You might also like
- Liver and ElectrolytesDocument7 pagesLiver and ElectrolytesDaniel LamasonNo ratings yet
- Level of Bilirubin To Cause Jaundice in Older Children and AdultsDocument2 pagesLevel of Bilirubin To Cause Jaundice in Older Children and AdultsSerious LeoNo ratings yet
- J Mpsur 2017 09 012Document7 pagesJ Mpsur 2017 09 012riffarsyad100% (1)
- Ictericia Diagnostico Ravindran2020Document7 pagesIctericia Diagnostico Ravindran2020Francisco CarpioNo ratings yet
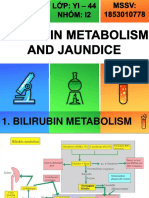
- Bilirubin Metabolism: Hd. - Msc. (Biochemistry)Document18 pagesBilirubin Metabolism: Hd. - Msc. (Biochemistry)MuhamadMarufNo ratings yet
- BIOCHEM Jaundice FinalDocument54 pagesBIOCHEM Jaundice FinalJohnRobynDiezNo ratings yet
- 57-Overview of Approach To HyperbilirubinemiaDocument21 pages57-Overview of Approach To Hyperbilirubinemiakushraj khandelwalNo ratings yet
- Heme DegradationDocument26 pagesHeme DegradationDerick SemNo ratings yet
- Jaundice and AscitesDocument15 pagesJaundice and AscitesJosiah Noella BrizNo ratings yet
- Jaundice FinalDocument30 pagesJaundice FinalFrances GrefalNo ratings yet
- Https:/emedicine - Medscape.com/article/178841 PrintDocument41 pagesHttps:/emedicine - Medscape.com/article/178841 PrinthellokayNo ratings yet
- IctericiaDocument19 pagesIctericiadavid pinedaNo ratings yet
- Clinical ChemistryDocument3 pagesClinical ChemistryHazel Loren GrandeNo ratings yet
- Biochemistry 10 BilirubinDocument34 pagesBiochemistry 10 BilirubinKmo mastnNo ratings yet
- 5 - JaundiceDocument16 pages5 - JaundiceHamzehNo ratings yet
- Neonatal JaundiceDocument48 pagesNeonatal JaundiceRemy MartinsNo ratings yet
- Jaundice in The Adult PatientDocument6 pagesJaundice in The Adult Patientrbatjun576No ratings yet
- Catabolism of HemeDocument34 pagesCatabolism of HemeGlen Jacobs Sumadihardja100% (2)
- Neonatal Indirect HyperbilirubinemiaDocument14 pagesNeonatal Indirect HyperbilirubinemiaValen CadenaNo ratings yet
- 212 Spring 2005 Heme DegradationDocument17 pages212 Spring 2005 Heme Degradationcockatoo_whiteNo ratings yet
- JaundiceDocument14 pagesJaundiceAnuradha NanayakkaraNo ratings yet
- Care of Neonate With HyperbilirubinemiaDocument11 pagesCare of Neonate With HyperbilirubinemiaKakali ChakrabortyNo ratings yet
- Core Concepts:: Bilirubin MetabolismDocument9 pagesCore Concepts:: Bilirubin MetabolismManasye AlanNo ratings yet
- PathologyDocument19 pagesPathologyAfrin AkhtarNo ratings yet
- The Biochemistry of JaundiceDocument29 pagesThe Biochemistry of JaundiceeminemizenNo ratings yet
- cc2 Lectures AllDocument256 pagescc2 Lectures AllJayson Dagohoy SudioNo ratings yet
- Jaundice NotesDocument8 pagesJaundice NotesDanielle Jann Manio ConcepcionNo ratings yet
- 8 BilirubinDocument25 pages8 BilirubinTagreed DerarNo ratings yet
- 9.1 Liver Function TestsDocument8 pages9.1 Liver Function TestsGio Joaquin SantosNo ratings yet
- Bilirubin: Conjugated UnconjugatedDocument2 pagesBilirubin: Conjugated UnconjugatedOrhan AsdfghjklNo ratings yet
- Core Concepts Bilirrubin MetabolismDocument9 pagesCore Concepts Bilirrubin MetabolismAngelina ChunNo ratings yet
- Pediatrics - Neonatal Jaundice PDFDocument2 pagesPediatrics - Neonatal Jaundice PDFJasmine KangNo ratings yet
- Conjugated Hyperbilirubinemia:: Screening and Treatment in Older Infants and ChildrenDocument11 pagesConjugated Hyperbilirubinemia:: Screening and Treatment in Older Infants and ChildrendjebrutNo ratings yet
- Neonatal JaundiceDocument6 pagesNeonatal JaundiceDoc Prince CaballeroNo ratings yet
- Catabolism of HemeDocument10 pagesCatabolism of Hemermsaeed09No ratings yet
- 1 Core Concepts Bilirubin MetabolismDocument9 pages1 Core Concepts Bilirubin Metabolismlink0105No ratings yet
- HB Degradation and Related ProblemDocument23 pagesHB Degradation and Related ProblemHatim AlnourNo ratings yet
- Heme Degradation & HyperbilirubinemiasDocument30 pagesHeme Degradation & HyperbilirubinemiasSubhi MishraNo ratings yet
- #19 GASMEN, Cyrille F. MED-1C Biochemical - Genetic Case 14Document2 pages#19 GASMEN, Cyrille F. MED-1C Biochemical - Genetic Case 14Cyrille GasmenNo ratings yet
- Neonatal Hyperbilirubinemia: Mahlet Abayneh Assistant Professor of PediatricsDocument41 pagesNeonatal Hyperbilirubinemia: Mahlet Abayneh Assistant Professor of PediatricsBegashawNo ratings yet
- Jaundice: in Older Children and AdolescentsDocument10 pagesJaundice: in Older Children and AdolescentsjoslinmtggmailcomNo ratings yet
- Jaundice: From Wikipedia, The Free EncyclopediaDocument27 pagesJaundice: From Wikipedia, The Free Encyclopediacherryann_calinogNo ratings yet
- Jaundice: in Older Children and AdolescentsDocument10 pagesJaundice: in Older Children and AdolescentshectorNo ratings yet
- L9 - Pathogenesis of JaundiceDocument23 pagesL9 - Pathogenesis of JaundicetrcfghNo ratings yet
- Liver Function Lecture NotesDocument9 pagesLiver Function Lecture NotesMarie Bernadette DigoNo ratings yet
- Heme Degradation & HyperbilirubinemiasDocument27 pagesHeme Degradation & HyperbilirubinemiasIMDCBiochemNo ratings yet
- Neonatal Jaundice CmeDocument39 pagesNeonatal Jaundice CmeGideon K. Mutai100% (1)
- Presentation 6Document12 pagesPresentation 6Hoàng TrúcNo ratings yet
- Physiology and Pathology BILIRUBIN SINTESISDocument9 pagesPhysiology and Pathology BILIRUBIN SINTESISIda Bagus SaktianaNo ratings yet
- Assignment 3 BilirubbinDocument5 pagesAssignment 3 Bilirubbinhaseeb ShafaatNo ratings yet
- Billirubin Metabolism (Prof. Taufiq)Document18 pagesBillirubin Metabolism (Prof. Taufiq)maudiaNo ratings yet
- Neonatal Hyperbilirubinemia PATHOPHYSIOLOGYDocument11 pagesNeonatal Hyperbilirubinemia PATHOPHYSIOLOGYG Trinity DeepakNo ratings yet
- Refer atDocument28 pagesRefer atAngga NuralamNo ratings yet
- BilirubinDocument40 pagesBilirubinAnisetiyowatiNo ratings yet
- Liver FunctionDocument30 pagesLiver FunctionAra ShirikaNo ratings yet
- Liver Function Tests (LFTS)Document18 pagesLiver Function Tests (LFTS)farkad rawiNo ratings yet
- 06 Bilirubin Metabolism016Document28 pages06 Bilirubin Metabolism016Arif NabeelNo ratings yet
- Kernicterus, (Bilirubin Encephalopathy) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandKernicterus, (Bilirubin Encephalopathy) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Jaundice, (Hyperbilirubinemia) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandJaundice, (Hyperbilirubinemia) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Gilbert's Syndrome: Causes, Tests and Treatment OptionsFrom EverandGilbert's Syndrome: Causes, Tests and Treatment OptionsRating: 4 out of 5 stars4/5 (1)
- Clinical Chemistry 1-Nonprotein Nitrogenous (NPN) CompoundsDocument12 pagesClinical Chemistry 1-Nonprotein Nitrogenous (NPN) CompoundsGeorge Carr PlazaNo ratings yet
- AssyriaDocument10 pagesAssyriaGeorge Carr PlazaNo ratings yet
- Methods Research DesignDocument4 pagesMethods Research DesignGeorge Carr PlazaNo ratings yet
- Data and Results F. Sakaguchi Test: Experiment Result - Positive - Red in Color - Presnt of Guadinine Group in ArginineDocument1 pageData and Results F. Sakaguchi Test: Experiment Result - Positive - Red in Color - Presnt of Guadinine Group in ArginineGeorge Carr PlazaNo ratings yet
- EthicsDocument2 pagesEthicsGeorge Carr PlazaNo ratings yet
- Name of The Test: ACROLEIN TEST: B. Results and InterpretationDocument2 pagesName of The Test: ACROLEIN TEST: B. Results and InterpretationGeorge Carr PlazaNo ratings yet
- Nervous System WorksheetDocument2 pagesNervous System WorksheetRoda Aranquez RabinoNo ratings yet
- CC Lab M1 7Document99 pagesCC Lab M1 7CDNo ratings yet
- 1BI0 1H Rms 20220224Document32 pages1BI0 1H Rms 20220224Musyoka DanteNo ratings yet
- Development of The Nervous System 3rd Edition Sanes Test BankDocument12 pagesDevelopment of The Nervous System 3rd Edition Sanes Test Bankdrerindavisddsybrqsdmajp100% (16)
- Evaluation of Filter Papers As A Novel Method For Transportation of Specimen For Diagnosis of Brucellosis in AnimalsDocument1 pageEvaluation of Filter Papers As A Novel Method For Transportation of Specimen For Diagnosis of Brucellosis in AnimalskotasurendraNo ratings yet
- Wheat Rust EnglishDocument10 pagesWheat Rust EnglishAanand JhaNo ratings yet
- General Microbiology Questions-2 PDFDocument36 pagesGeneral Microbiology Questions-2 PDFAntar Inenigog67% (3)
- Acfrogdny3we1zkabz7ooaocl2 Ryjfdmxsgfsf7vnow4ocsgtpvej h7bxmqxkr351cdggvxshhx1sl Msjslh-Ebntbyvzq6uu9yry0p N7jy-Iz5bs K03fa70qjwmowd-6zokqasm-NlwyliDocument35 pagesAcfrogdny3we1zkabz7ooaocl2 Ryjfdmxsgfsf7vnow4ocsgtpvej h7bxmqxkr351cdggvxshhx1sl Msjslh-Ebntbyvzq6uu9yry0p N7jy-Iz5bs K03fa70qjwmowd-6zokqasm-NlwyliRosario RomeroNo ratings yet
- Brochure BactAlertDocument2 pagesBrochure BactAlertCorporativo DRLABNo ratings yet
- Living Donor Lobar Lung Transplantation (LDLLT) : PolicyDocument6 pagesLiving Donor Lobar Lung Transplantation (LDLLT) : PolicySherif EldegwyNo ratings yet
- Case Report Herpes Zoster Regio Th11 - L5Document37 pagesCase Report Herpes Zoster Regio Th11 - L5fatqur28No ratings yet
- Liu2017 EhpDocument6 pagesLiu2017 EhpmokengNo ratings yet
- Drugs Used To Treat AnemiaDocument36 pagesDrugs Used To Treat AnemiaMoxie Macado100% (1)
- DM Type 1Document14 pagesDM Type 1Yogi SetiawanNo ratings yet
- Crossword-9 Lrat MVRPDocument2 pagesCrossword-9 Lrat MVRPFrancis ValdezNo ratings yet
- Ab Dosis NeonatusDocument6 pagesAb Dosis NeonatusAditya WicaksonoNo ratings yet
- Biosafety ppt-12Document56 pagesBiosafety ppt-12Pramod50% (2)
- Cbcs Syllabus Botany 2017-2020Document45 pagesCbcs Syllabus Botany 2017-2020Rajesh Kumar SahuNo ratings yet
- Insulin, Glucagon, and Diabetes MellitusDocument58 pagesInsulin, Glucagon, and Diabetes MellituschayChay gapolNo ratings yet
- Farmakoterapi StrokeDocument37 pagesFarmakoterapi StrokeRaizel DNo ratings yet
- Recombinant DNA TechnologyDocument80 pagesRecombinant DNA TechnologyRaizza Mae CorderoNo ratings yet
- Atellica Solution: Assays OverviewDocument8 pagesAtellica Solution: Assays OverviewDarshana JuvekarNo ratings yet
- T0610e PDFDocument344 pagesT0610e PDFShofli Yazid Khoirul RoziqinNo ratings yet
- Dr. Engku Ibrahim SyubliDocument45 pagesDr. Engku Ibrahim SyubliRUSLI OTHMANNo ratings yet
- Evaluation of Liver FunctionDocument20 pagesEvaluation of Liver FunctionWill RiañoNo ratings yet
- Nervous System WorksheetDocument4 pagesNervous System WorksheetjamesNo ratings yet
- Detection of Avian Encephalomyelitis VirusDocument4 pagesDetection of Avian Encephalomyelitis VirusAline FerreiraNo ratings yet
- Bacterial and Fungal Study of 100 Cases of Chronic Suppurative Otitis MediaDocument4 pagesBacterial and Fungal Study of 100 Cases of Chronic Suppurative Otitis MediaMelanie McguireNo ratings yet
- Makubi MSD Fullfield Report .Document18 pagesMakubi MSD Fullfield Report .Makubi majura100% (1)
- Meat PreservationDocument28 pagesMeat PreservationSameh GhareebNo ratings yet