You might also like
- AGA Institute Review of Endoscopic SedationDocument27 pagesAGA Institute Review of Endoscopic Sedationnohora parradoNo ratings yet
- Pre-Anesthesia Evaluation GuideDocument5 pagesPre-Anesthesia Evaluation GuideSarah GoNo ratings yet
- Preoperative evaluation and considerations in childrenDocument24 pagesPreoperative evaluation and considerations in childrenArshan AliNo ratings yet
- Critical Care Medicine OutlineDocument76 pagesCritical Care Medicine OutlineMiss KNo ratings yet
- Anesthesiology ManualDocument131 pagesAnesthesiology ManualHarlyn Magsino100% (1)
- Articulo. DIAGNOSTICO DEL PACIENTE INTOXICADODocument7 pagesArticulo. DIAGNOSTICO DEL PACIENTE INTOXICADOJosé Rafael Reyes NavaNo ratings yet
- Akukwata SeminarDocument22 pagesAkukwata SeminarjenniferNo ratings yet
- Palfa BoneDocument38 pagesPalfa Bonemadara ëNo ratings yet
- 02evaluation Before AnesthesiaDocument34 pages02evaluation Before Anesthesiasimple livingNo ratings yet
- 3. 麻醉前访视Document34 pages3. 麻醉前访视simple livingNo ratings yet
- Persiapan Pra Operasi: Bagian/ SMF Anestesiologi Rs Islam Sultan Agung/ Fakultas Kedokteran Unissula 2007Document22 pagesPersiapan Pra Operasi: Bagian/ SMF Anestesiologi Rs Islam Sultan Agung/ Fakultas Kedokteran Unissula 2007ariahenkusNo ratings yet
- General AnaesthesiaDocument10 pagesGeneral AnaesthesiaAlfiatuz ZahroNo ratings yet
- Guideline For Pediatric Procedural Sedation and Analgesia in The Emergency DepartmentDocument23 pagesGuideline For Pediatric Procedural Sedation and Analgesia in The Emergency DepartmentSantosa TandiNo ratings yet
- Linnen Et Al. (2011) - Depression and Essential Health Risk Factors in Surgical Patients in The Preoperative Anaesthesiological Assessment ClinicDocument9 pagesLinnen Et Al. (2011) - Depression and Essential Health Risk Factors in Surgical Patients in The Preoperative Anaesthesiological Assessment Clinicfabienne czechNo ratings yet
- (Surg2) 5.1a Introduction To Anesthesia Part 1Document21 pages(Surg2) 5.1a Introduction To Anesthesia Part 1AlloiBialbaNo ratings yet
- HP May00 Sedat PDFDocument9 pagesHP May00 Sedat PDFSaurabh SatheNo ratings yet
- 157 - Clinical Trials Adverse Events ChaDocument6 pages157 - Clinical Trials Adverse Events ChaWoo Rin ParkNo ratings yet
- Preoperative Period Evaluation GuideDocument3 pagesPreoperative Period Evaluation GuideStepyn SalvadorNo ratings yet
- Ketut Suryana Ketut SuardamanaDocument46 pagesKetut Suryana Ketut SuardamanaYogiswara KarangNo ratings yet
- Principles and ConceptsDocument83 pagesPrinciples and ConceptsAndrea HernandezNo ratings yet
- Clinical Medicine Ashok ChandraDocument52 pagesClinical Medicine Ashok ChandraVaishnavi Agrawal100% (1)
- 20.matsota PKDocument19 pages20.matsota PKChristian YonathanNo ratings yet
- Monitoring Efek Samping Obat 12Document36 pagesMonitoring Efek Samping Obat 12Novitra Dewi100% (1)
- HshsjneDocument5 pagesHshsjneyunia habsariNo ratings yet
- Effect Observation of Electro Acupunctute AnesthesiaDocument7 pagesEffect Observation of Electro Acupunctute Anesthesiaadink mochammadNo ratings yet
- Practice Advisory For Preanesthesia Evaluation. An Updated Report by The American Society of Anesthesiologists Task Force On PreanesthesiaDocument12 pagesPractice Advisory For Preanesthesia Evaluation. An Updated Report by The American Society of Anesthesiologists Task Force On PreanesthesiaMadalina TalpauNo ratings yet
- Kuliah 11 IBUV Anestesi Pada Hewan Besar PDFDocument29 pagesKuliah 11 IBUV Anestesi Pada Hewan Besar PDFElsi RahmadhaniNo ratings yet
- Induction of AnaesthesiaDocument7 pagesInduction of AnaesthesiaMiguel Angel CabezasNo ratings yet
- Essentials of Anesthesia For Medical Students FinalDocument82 pagesEssentials of Anesthesia For Medical Students FinalEs LamNo ratings yet
- Clinical and Experimental Allergy: BSACI Guidelines For The Management of Drug AllergyDocument19 pagesClinical and Experimental Allergy: BSACI Guidelines For The Management of Drug AllergyJair Edu100% (1)
- Chap1 MageeDocument83 pagesChap1 MageeSerenela PiazzaNo ratings yet
- ICU ProtocolsDocument35 pagesICU ProtocolsJohn Reynolds100% (6)
- Lee 2014Document7 pagesLee 2014Santosa TandiNo ratings yet
- Lee 2014Document7 pagesLee 2014Santosa TandiNo ratings yet
- General AnesthesiaDocument11 pagesGeneral AnesthesiaGERSON RYANTONo ratings yet
- Jose Martinez Care PlanDocument7 pagesJose Martinez Care PlanJulia BrownNo ratings yet
- BSN Compiled Notes - PharmacologyDocument6 pagesBSN Compiled Notes - PharmacologyAbigail RegaladoNo ratings yet
- Clinical Pharmacy 2nd MidDocument65 pagesClinical Pharmacy 2nd Midsmart hussainNo ratings yet
- Bases Farmacológicas de La Anestesia General Endovenosa de Corta Duración en El EquinoDocument26 pagesBases Farmacológicas de La Anestesia General Endovenosa de Corta Duración en El EquinoflorthyNo ratings yet
- Emergency Medicine in MBBSDocument85 pagesEmergency Medicine in MBBSPATHMAPRIYA GANESANNo ratings yet
- Introduction To Pharmacology 2020 UpdatedDocument21 pagesIntroduction To Pharmacology 2020 Updatedاحمد علىNo ratings yet
- Analgesia en Apendicitis AgudaDocument3 pagesAnalgesia en Apendicitis Agudasilvia barbosaNo ratings yet
- Autonomic Testing, Methods and TechniquesDocument15 pagesAutonomic Testing, Methods and TechniquesYanina Pérez de VillarrealNo ratings yet
- Tham 2010Document13 pagesTham 2010Santosa TandiNo ratings yet
- Epilepsia - 2018 - Hocker - Anesthetic Drugs For The Treatment of Status EpilepticusDocument5 pagesEpilepsia - 2018 - Hocker - Anesthetic Drugs For The Treatment of Status EpilepticusKikie Rizky HeningNo ratings yet
- Effects of Aromatherapy Acupressure On Hemiplegic Shoulder Pain and Motor Power in Stroke Patients: A Pilot StudyDocument6 pagesEffects of Aromatherapy Acupressure On Hemiplegic Shoulder Pain and Motor Power in Stroke Patients: A Pilot StudyAnggelia jopa sariNo ratings yet
- MED II 21 Poisoning Drug Overdose and EnvenomationDocument10 pagesMED II 21 Poisoning Drug Overdose and Envenomationreedon quinanNo ratings yet
- Introduction To Oral Manifestations of Systemic DiseasesDocument8 pagesIntroduction To Oral Manifestations of Systemic DiseasesVitória SilvaNo ratings yet
- DR Makam Sri Harsha ThesisDocument33 pagesDR Makam Sri Harsha ThesissumitNo ratings yet
- (KULIAH 5) Reaksi AnafilaksisDocument30 pages(KULIAH 5) Reaksi AnafilaksisArtawa Darma YudaNo ratings yet
- Appendicitis Case StudyDocument23 pagesAppendicitis Case StudyB1. Rosalinda Angelika PutriNo ratings yet
- Anesthesia and Analgesia Book 1Document104 pagesAnesthesia and Analgesia Book 1Alan Alvaro Salazar GarciaNo ratings yet
- White Et Al 2021 Evaluation of Medications Used for Hospitalized Patients With Sleep Disturbances a Frequency AnalysisDocument13 pagesWhite Et Al 2021 Evaluation of Medications Used for Hospitalized Patients With Sleep Disturbances a Frequency AnalysisFrancisco Javier Diaz PincheiraNo ratings yet
- 1.04 (Surgery) Anesthesiology Part 1Document5 pages1.04 (Surgery) Anesthesiology Part 1Leo Mari Go LimNo ratings yet
- Krishnaswamy 2021 - Critical Care Management of The Patient With Anaphylaxis - A Concise Definitive ReviewDocument20 pagesKrishnaswamy 2021 - Critical Care Management of The Patient With Anaphylaxis - A Concise Definitive ReviewKhanh Ha NguyenNo ratings yet
- Sexton 2011Document19 pagesSexton 2011koushikNo ratings yet
- Patton Et Al 2018 AnaesthesiaDocument9 pagesPatton Et Al 2018 AnaesthesiadiegoNo ratings yet
- Pre-Anesthetic Care and Patients Optimization: Presenter: Dr. Mwasapi P. PDocument96 pagesPre-Anesthetic Care and Patients Optimization: Presenter: Dr. Mwasapi P. PfadhiliNo ratings yet
- 01 Clinical Anesthesiology OverviewDocument2 pages01 Clinical Anesthesiology OverviewJim Jose AntonyNo ratings yet
- Chapter4 - Analysis of EQ Loads Acting On StructuresDocument4 pagesChapter4 - Analysis of EQ Loads Acting On StructureshNo ratings yet
- Entrepreneurship Final Module StuDocument180 pagesEntrepreneurship Final Module Studagmawi girmaNo ratings yet
- Chapter3 - Analysis Ofwind Loads Acting On StructuresDocument6 pagesChapter3 - Analysis Ofwind Loads Acting On Structuresdagmawi girmaNo ratings yet
- Best Practice Manual For Thin Bituminous Surfacings 2013 PDFDocument145 pagesBest Practice Manual For Thin Bituminous Surfacings 2013 PDFashe zinabNo ratings yet
- Multi PageDocument75 pagesMulti Pagedagmawi girmaNo ratings yet
- Batcoda Technical SpecificationDocument10 pagesBatcoda Technical Specificationdagmawi girmaNo ratings yet
- Batcoda Technical SpecificationDocument10 pagesBatcoda Technical Specificationdagmawi girmaNo ratings yet
- YesDocument1 pageYesdagmawi girmaNo ratings yet
- Useful Relations in Quantum Field TheoryDocument30 pagesUseful Relations in Quantum Field TheoryDanielGutierrez100% (1)
- Komatsud65ex 16dozerbulldozerservicerepairmanualsn80001andup 200727063646Document26 pagesKomatsud65ex 16dozerbulldozerservicerepairmanualsn80001andup 200727063646juan santa cruzNo ratings yet
- Boala Cronica Obstructive: BpocDocument21 pagesBoala Cronica Obstructive: BpocNicoleta IliescuNo ratings yet
- SMEs, Trade Finance and New TechnologyDocument34 pagesSMEs, Trade Finance and New TechnologyADBI EventsNo ratings yet
- Liquid Analysis v3 Powell-Cumming 2010 StanfordgwDocument28 pagesLiquid Analysis v3 Powell-Cumming 2010 StanfordgwErfanNo ratings yet
- Indonesia Banks Bank Mandiri Trading Buy on Strong 9M21 EarningsDocument8 pagesIndonesia Banks Bank Mandiri Trading Buy on Strong 9M21 EarningsdkdehackerNo ratings yet
- Technology Consulting: Amruta Kulkarni Anu Abraham Rajat JainDocument9 pagesTechnology Consulting: Amruta Kulkarni Anu Abraham Rajat JainRajat JainNo ratings yet
- Business StrategiesDocument2 pagesBusiness Strategiesthristanlexter694No ratings yet
- Tirfor: Lifting and Pulling Machines With Unlimited Wire RopeDocument26 pagesTirfor: Lifting and Pulling Machines With Unlimited Wire RopeGreg ArabazNo ratings yet
- Ek Pardesi Mera Dil Le Gaya Lyrics English Translation - Lyrics GemDocument1 pageEk Pardesi Mera Dil Le Gaya Lyrics English Translation - Lyrics Gemmahsa.molaiepanahNo ratings yet
- Smart EE June 2022 - PackageDocument19 pagesSmart EE June 2022 - PackageMercy FeNo ratings yet
- Inspection and Acceptance Report: Stock No. Unit Description QuantityDocument6 pagesInspection and Acceptance Report: Stock No. Unit Description QuantityAnj LeeNo ratings yet
- MECHANICAL PROPERTIES OF SOLIDSDocument39 pagesMECHANICAL PROPERTIES OF SOLIDSAbdul Musavir100% (1)
- Philippine Police Report Suicide InvestigationDocument2 pagesPhilippine Police Report Suicide InvestigationPAUL ALDANA82% (34)
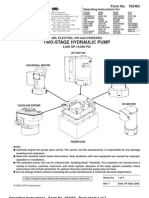
- Power Team PE55 ManualDocument13 pagesPower Team PE55 ManualTitanplyNo ratings yet
- An Overview of The FUPLA 2 Tools: Project DatabaseDocument2 pagesAn Overview of The FUPLA 2 Tools: Project DatabaseJulio Cesar Rojas SaavedraNo ratings yet
- GastrectomyDocument19 pagesGastrectomyCyrus GarciaNo ratings yet
- Multivariate Analysis Homework QuestionsDocument2 pagesMultivariate Analysis Homework Questions歐怡君No ratings yet
- DLL Grade7 First 1solutions ConcentrationDocument5 pagesDLL Grade7 First 1solutions ConcentrationJaneth de JuanNo ratings yet
- Telecommunications TechnicianDocument4 pagesTelecommunications Technicianapi-78381064No ratings yet
- Hisar CFC - Approved DPRDocument126 pagesHisar CFC - Approved DPRSATYAM KUMARNo ratings yet
- Masterbatch Buyers Guide PDFDocument8 pagesMasterbatch Buyers Guide PDFgurver55No ratings yet
- PBS-P100 Facilities Standards GuideDocument327 pagesPBS-P100 Facilities Standards Guidecessna5538cNo ratings yet
- The Interview: P F T IDocument14 pagesThe Interview: P F T IkkkkccccNo ratings yet
- Mechanical Engineer with Experience in Heavy Mining Machinery MaintenanceDocument1 pageMechanical Engineer with Experience in Heavy Mining Machinery MaintenanceCertified Rabbits LoverNo ratings yet
- Astm D 664 - 07Document8 pagesAstm D 664 - 07Alfonso MartínezNo ratings yet
- Jotrun TDSDocument4 pagesJotrun TDSBiju_PottayilNo ratings yet
- Decembermagazine 2009Document20 pagesDecembermagazine 2009maria_diyah4312No ratings yet
- Sia Mock+Test 1 Csat Updated CompressedDocument216 pagesSia Mock+Test 1 Csat Updated Compressedpooja bhatiNo ratings yet
- Appliance Saver Prevents OverheatingDocument2 pagesAppliance Saver Prevents OverheatingphilipNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)