You might also like
- Design and Analysis of Intez Type Water Tank Using SAP 2000 SoftwareDocument7 pagesDesign and Analysis of Intez Type Water Tank Using SAP 2000 SoftwareIJRASETPublicationsNo ratings yet
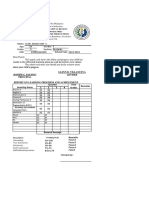
- Hrpta Financial ReportDocument5 pagesHrpta Financial ReportQueen Crystl100% (1)
- ISO 27005 Risk Manager - Four Page BrochureDocument4 pagesISO 27005 Risk Manager - Four Page BrochurePECBCERTIFICATIONNo ratings yet
- Dirty Class RecordDocument2 pagesDirty Class RecordDominic HawangNo ratings yet
- Ffs-su-5217-A - Design of Fixed Platform StructuresDocument134 pagesFfs-su-5217-A - Design of Fixed Platform StructuresBolarinwa100% (1)
- Kra 1 Kra 3 Kra 1 Kra 3Document2 pagesKra 1 Kra 3 Kra 1 Kra 3KRIZZIE JOY CAILINGNo ratings yet
- Extraction of Furfural From Bagasse PDFDocument2 pagesExtraction of Furfural From Bagasse PDFAmanda100% (1)
- Matab AngNHS Accomplishment Report CFSSDocument3 pagesMatab AngNHS Accomplishment Report CFSSKRIZZIE JOY CAILING100% (8)
- Cordova National High School: Report On AttendanceDocument11 pagesCordova National High School: Report On AttendanceR TECHNo ratings yet
- Diagnostic Test Technical DraftingDocument4 pagesDiagnostic Test Technical DraftingKRIZZIE JOY CAILINGNo ratings yet
- BATO NHS CFSS Accomplishment ReportDocument9 pagesBATO NHS CFSS Accomplishment ReportKRIZZIE JOY CAILINGNo ratings yet
- 9 Garolacan - H8DD-IIIb-c-17 NewDocument17 pages9 Garolacan - H8DD-IIIb-c-17 NewKRIZZIE JOY CAILINGNo ratings yet
- Pre Observation Information ANDROLYN P. RODRIGUEZDocument2 pagesPre Observation Information ANDROLYN P. RODRIGUEZKRIZZIE JOY CAILING100% (2)
- ANNEX A Masterlists of School Based Immunization 2019Document24 pagesANNEX A Masterlists of School Based Immunization 2019KRIZZIE JOY CAILINGNo ratings yet
- Masterlist of ChildrenDocument8 pagesMasterlist of ChildrenJoena Balicao0% (1)
- TOSgrade4 2nd SINING MALLARI RAMIREZ COLARDocument4 pagesTOSgrade4 2nd SINING MALLARI RAMIREZ COLARbenz cadiongNo ratings yet
- No. 013 PDFDocument10 pagesNo. 013 PDFJ Drew NayaradaNo ratings yet
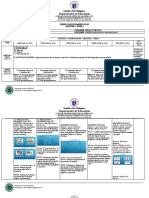
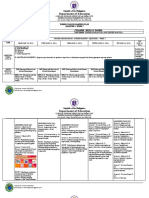
- 10-31 To 11-04-2022 - DLL - Science 8Document3 pages10-31 To 11-04-2022 - DLL - Science 8Daniel ManuelNo ratings yet
- Department of Education: Republic of The PhilippinesDocument7 pagesDepartment of Education: Republic of The PhilippinesMhelba Erfe PedrozoNo ratings yet
- Baseline EditeddDocument85 pagesBaseline EditeddSylvia N. CantoriaNo ratings yet
- Distribution and Retrieval 2022Document5 pagesDistribution and Retrieval 2022Ai AiNo ratings yet
- Grade 10 GradeSheet 2023-24Document132 pagesGrade 10 GradeSheet 2023-24Krizzie Joy CailingNo ratings yet
- History of Barangay DDocument7 pagesHistory of Barangay DDiovic TanNo ratings yet
- Form Xiv: Luray Ii Barangay High School Luray Ii Barangay High SchoolDocument14 pagesForm Xiv: Luray Ii Barangay High School Luray Ii Barangay High SchoolKrizzie Jade CailingNo ratings yet
- Consolidated Mean PL SD Average of Grade 8Document6 pagesConsolidated Mean PL SD Average of Grade 8JP BotorNo ratings yet
- Grade 7 SF1 OFFICIALDocument25 pagesGrade 7 SF1 OFFICIALPeterClomaJr.No ratings yet
- TOSgrade4 2nd SINING MALLARI RAMIREZ COLARDocument6 pagesTOSgrade4 2nd SINING MALLARI RAMIREZ COLARbenz cadiongNo ratings yet
- ClorDocument2 pagesClorAngel May S. ClorNo ratings yet
- Department of Education: Republic of The PhilippinesDocument6 pagesDepartment of Education: Republic of The PhilippinesMhelba Erfe PedrozoNo ratings yet
- FERRANDODocument2 pagesFERRANDOtatski cabcabNo ratings yet
- Department of Education: Republic of The PhilippinesDocument7 pagesDepartment of Education: Republic of The PhilippinesMhelba Erfe PedrozoNo ratings yet
- MNHS WifaDocument30 pagesMNHS WifaMyrna MendozaNo ratings yet
- Project Proposal - Concreting Pathway (SPTA2023) - ScribDocument2 pagesProject Proposal - Concreting Pathway (SPTA2023) - ScribMary Jean Dela CruzNo ratings yet
- Module Monitoring Form Distribution and Retrieval 1St Quarter Week 1Document10 pagesModule Monitoring Form Distribution and Retrieval 1St Quarter Week 1FLORDELIZA ALBANO PAGLINAWANNo ratings yet
- Final ProjectDocument56 pagesFinal ProjectPrachi SharmaNo ratings yet
- Department of Education: Republic of The PhilippinesDocument8 pagesDepartment of Education: Republic of The PhilippinesMhelba Erfe PedrozoNo ratings yet
- School Form 2 Daily Attendance Report of Learners For Senior High School (SF2-SHS)Document26 pagesSchool Form 2 Daily Attendance Report of Learners For Senior High School (SF2-SHS)Mary Gretel OntingNo ratings yet
- Monitoring of Returning Overseas Filipino Workers (Ofws) Iloilo CityDocument104 pagesMonitoring of Returning Overseas Filipino Workers (Ofws) Iloilo CityJe Re MaeNo ratings yet
- Personal Data Sheet: Nursing ProgramDocument2 pagesPersonal Data Sheet: Nursing ProgramJrose CuerpoNo ratings yet
- Ranking 9bDocument65 pagesRanking 9bDanilo de MesaNo ratings yet
- Grade 8 Sf1 Official 2022Document25 pagesGrade 8 Sf1 Official 2022PeterClomaJr.No ratings yet
- Grade 11 SF2 ICTDocument11 pagesGrade 11 SF2 ICTCeasar Ryan AsuncionNo ratings yet
- Sf2 - 2022 - Automated by Sir Jeson SiblagDocument21 pagesSf2 - 2022 - Automated by Sir Jeson SiblagDarlene MotaNo ratings yet
- PRK - Saging, Lower Dicayas, Dipolog City Mobile #: 09500983024Document1 pagePRK - Saging, Lower Dicayas, Dipolog City Mobile #: 09500983024Kevin Lee PoracanNo ratings yet
- Complete Projrct Proposal (1) .Docx NewDocument11 pagesComplete Projrct Proposal (1) .Docx Newcacay cayNo ratings yet
- Learner'S Anecdotal RecordDocument3 pagesLearner'S Anecdotal RecordGlenn Mar DomingoNo ratings yet
- SF 5B Grade 11 Charity HUMSSDocument29 pagesSF 5B Grade 11 Charity HUMSSJoan Mangente GinggoNo ratings yet
- Scoping Exercise Draft of Molteno 2023Document24 pagesScoping Exercise Draft of Molteno 2023Eastern BachelorNo ratings yet
- Revised TDP Form 2020 2021Document2 pagesRevised TDP Form 2020 2021Mark Darryl Mansay DeloriaNo ratings yet
- School Form 2 (SF2) Daily Attendance Report of Learners: Male - Total Per DayDocument11 pagesSchool Form 2 (SF2) Daily Attendance Report of Learners: Male - Total Per DayJonah Marie Therese BurlazaNo ratings yet
- Form 2 Shs - February2017 - 2018 - 1Document89 pagesForm 2 Shs - February2017 - 2018 - 1Geraldo N. QuillaoNo ratings yet
- Don Felix T. Lacson Memorial National High SchoolDocument12 pagesDon Felix T. Lacson Memorial National High SchoolCeasar Ryan AsuncionNo ratings yet
- 2nd Quarter 08 Quartz Baladad Maquel PDFDocument2 pages2nd Quarter 08 Quartz Baladad Maquel PDFarmand bayoranNo ratings yet
- Deped Form 18 - ADocument2 pagesDeped Form 18 - Acorazon ignacioNo ratings yet
- Barts W21 Kids PDFDocument69 pagesBarts W21 Kids PDFvasile0% (1)
- Self-Learning Modules and Learning Activity Sheets Grade 11-Tvl 1B (Home Economics)Document2 pagesSelf-Learning Modules and Learning Activity Sheets Grade 11-Tvl 1B (Home Economics)Ma Eloiza Kaye BroñolaNo ratings yet
- 10-10 To 14-2022 - DLL - Science 8Document3 pages10-10 To 14-2022 - DLL - Science 8Daniel ManuelNo ratings yet
- I. Personal Information A. Personal Data: (To Be Filled in by APPLICANT)Document1 pageI. Personal Information A. Personal Data: (To Be Filled in by APPLICANT)Glinn CaspeNo ratings yet
- 35 Baybayon Buyongmaribago LLC ML Dar NHA ValMLDocument10 pages35 Baybayon Buyongmaribago LLC ML Dar NHA ValMLJube Kathreen ObidoNo ratings yet
- SF2 August Artemis HumssDocument4 pagesSF2 August Artemis Humssalfred naveaNo ratings yet
- School ID 102106 2019-2020 June, 2019 Name of School Gonzales ES Grade Level Grade 6 Section Grade 6 School Year Report For The Month ofDocument4 pagesSchool ID 102106 2019-2020 June, 2019 Name of School Gonzales ES Grade Level Grade 6 Section Grade 6 School Year Report For The Month ofAnalisa Cada MapiliNo ratings yet
- SF2 - 2021 - Grade 10 (Year IV) - GALILEIDocument6 pagesSF2 - 2021 - Grade 10 (Year IV) - GALILEIJeannie TingaNo ratings yet
- Republic of The Philippines Department of Education National Capital Region Division of Quezon City District 1Document1 pageRepublic of The Philippines Department of Education National Capital Region Division of Quezon City District 1December-Anne CabatlaoNo ratings yet
- ACES CLASSROOM INVENTORY 2022 TemplateDocument3 pagesACES CLASSROOM INVENTORY 2022 TemplateMELISSA PANAGANo ratings yet
- 2Q Group1 2A CV Project 4 WEEK 2Document1 page2Q Group1 2A CV Project 4 WEEK 2joselyn medinaNo ratings yet
- School-Based Weekly Iron Folic Acid (WIFA) Supplementation: Form 1 - Classroom Level Annex A1Document1 pageSchool-Based Weekly Iron Folic Acid (WIFA) Supplementation: Form 1 - Classroom Level Annex A1JeffAndradaNo ratings yet
- City Schools Division of Pagadian Deborok Elementary SchoolDocument5 pagesCity Schools Division of Pagadian Deborok Elementary SchoolQueen CrystlNo ratings yet
- Visayas AbpDocument6 pagesVisayas AbpEdil MendozaNo ratings yet
- Krizzie Joy D. Cailing 727Document2 pagesKrizzie Joy D. Cailing 727KRIZZIE JOY CAILINGNo ratings yet
- Glipa Session 3 Providing Warmth and StructureDocument1 pageGlipa Session 3 Providing Warmth and StructureKRIZZIE JOY CAILINGNo ratings yet
- RPMS - Portfolio - Design 2 ObjectivesDocument19 pagesRPMS - Portfolio - Design 2 ObjectivesKRIZZIE JOY CAILINGNo ratings yet
- Level of Dimensions of Classroom Managment Questionaire 10222020Document5 pagesLevel of Dimensions of Classroom Managment Questionaire 10222020KRIZZIE JOY CAILINGNo ratings yet
- Grade: Grade Viii Subject: Technical Drafting Grading Period: 1st DateDocument1 pageGrade: Grade Viii Subject: Technical Drafting Grading Period: 1st DateKRIZZIE JOY CAILING100% (1)
- Workweek Plan Individual Iwp Josie Lou H. Juarez 11-09-11!13!20Document1 pageWorkweek Plan Individual Iwp Josie Lou H. Juarez 11-09-11!13!20KRIZZIE JOY CAILINGNo ratings yet
- Obj Ecti Ve 1Document31 pagesObj Ecti Ve 1KRIZZIE JOY CAILINGNo ratings yet
- Deworming GRADE 8 ELSIEDocument4 pagesDeworming GRADE 8 ELSIEKRIZZIE JOY CAILINGNo ratings yet
- Sectioning by Barangay As of August 25 2020Document97 pagesSectioning by Barangay As of August 25 2020KRIZZIE JOY CAILINGNo ratings yet
- Group Project 0011D - Bus5111Document4 pagesGroup Project 0011D - Bus5111Franklyn Doh-NaniNo ratings yet
- IIMBA-90, Ma Kyu Kyu, MIS Moderation AssignmentDocument7 pagesIIMBA-90, Ma Kyu Kyu, MIS Moderation AssignmentChan Myae PaingNo ratings yet
- Reading 5-M-9Document7 pagesReading 5-M-9YuliNo ratings yet
- MEM 18.7A Maintain and Repair Mechanical Drives and Mechanical TransmissionDocument24 pagesMEM 18.7A Maintain and Repair Mechanical Drives and Mechanical TransmissionMick EastleyNo ratings yet
- MSI DocumentDocument1 pageMSI DocumentjuballerNo ratings yet
- ECD Engagement Session: - Route To Professional EngineerDocument1 pageECD Engagement Session: - Route To Professional EngineerKevin LowNo ratings yet
- Fire Incident Reporting System: Near Real Time Data and Geospatial Analysis ApproachDocument6 pagesFire Incident Reporting System: Near Real Time Data and Geospatial Analysis ApproachJhoy Espinosa LunarNo ratings yet
- DOWSIL™ 3-1944 RTV Coating: Features & BenefitsDocument4 pagesDOWSIL™ 3-1944 RTV Coating: Features & Benefitsquang trinhNo ratings yet
- CV Exim RudiDocument1 pageCV Exim RudiPrimantara SentosaNo ratings yet
- Examples - Shafts: B. Free Body Diagram of Forces A. Chain Drive AssemblyDocument4 pagesExamples - Shafts: B. Free Body Diagram of Forces A. Chain Drive AssemblyHarish Mohankrishnan NairNo ratings yet
- Wankat, Chapter 13, p.424 Seader and Henley, Chapter 8, Pp. 308 - 315Document39 pagesWankat, Chapter 13, p.424 Seader and Henley, Chapter 8, Pp. 308 - 315Anonymous CYvLZR29bNo ratings yet
- This Study Resource Was: Lab Report#11Document6 pagesThis Study Resource Was: Lab Report#11malik jarrarNo ratings yet
- Strategic Management and EntrepreneurshipDocument3 pagesStrategic Management and EntrepreneurshipLuke AdriaanNo ratings yet
- Indian Institution of Engineers: Chartered EngineerDocument1 pageIndian Institution of Engineers: Chartered EngineerKapil VermaNo ratings yet
- ĐỀDocument34 pagesĐỀThành PhátNo ratings yet
- Futurist ManifestoDocument5 pagesFuturist ManifestoChloe KnopfNo ratings yet
- Varietal Screening of Cucumber in Sundarharaicha Municipality, Morang, NepalDocument8 pagesVarietal Screening of Cucumber in Sundarharaicha Municipality, Morang, NepalMamta AgarwalNo ratings yet
- A 217Document1 pageA 217AnuranjanNo ratings yet
- Iron Kingdoms Roleplaying Game Character SheetDocument2 pagesIron Kingdoms Roleplaying Game Character Sheetjoshua vogelNo ratings yet
- Awpl Product BroucherDocument19 pagesAwpl Product BroucherBikash KumarNo ratings yet
- Revised Trade Message Broadcast ArchitectureDocument90 pagesRevised Trade Message Broadcast ArchitectureprashantgoruleNo ratings yet
- JOTUN TDS - Penguard E50Document5 pagesJOTUN TDS - Penguard E50Sachin SinghalNo ratings yet
- Lenovo V330 15IKB Platform SpecificationDocument1 pageLenovo V330 15IKB Platform SpecificationgcirviniNo ratings yet
- CMIT-602-COM-00.08-210001 Execution Management Plan - 0Document17 pagesCMIT-602-COM-00.08-210001 Execution Management Plan - 0Santo KuolNo ratings yet
- Ecopass From GI V2 14Document10 pagesEcopass From GI V2 14Achmad Diky IrawanNo ratings yet
- Arcelor Mittal HistarDocument32 pagesArcelor Mittal HistarAnonymous uNhWGqNzNo ratings yet