You might also like
- Portal Hypertension: (Surgical Complications)Document50 pagesPortal Hypertension: (Surgical Complications)api-19916399100% (1)
- Portal HypertensionDocument13 pagesPortal HypertensionEmmaNo ratings yet
- Esophageal VaricesDocument4 pagesEsophageal Varicesbrian3442No ratings yet
- Esophageal VaricesDocument9 pagesEsophageal VaricesErina WahyuniNo ratings yet
- Upper GI BleedingDocument15 pagesUpper GI BleedingShishir ShresthaNo ratings yet
- Upper and Lower GI Bleeding DR LC 21 May 2019Document36 pagesUpper and Lower GI Bleeding DR LC 21 May 2019jialeongNo ratings yet
- Chronic Liver Disease Decompensated N PDFDocument6 pagesChronic Liver Disease Decompensated N PDFmzhao230No ratings yet
- Portal HypertensionDocument11 pagesPortal Hypertensionsaeid seyedraoufiNo ratings yet
- Gastrointestinal BleedingDocument3 pagesGastrointestinal BleedingmatsuleaNo ratings yet
- Portal Hypotension: Clinical AssignmentDocument8 pagesPortal Hypotension: Clinical AssignmentM shayan JavedNo ratings yet
- Esophageal-Varices 20240201 124908 0000Document25 pagesEsophageal-Varices 20240201 124908 0000Eurika P OrolfoNo ratings yet
- Upper GI Bleeding ManagementDocument30 pagesUpper GI Bleeding ManagementBibek GhimireNo ratings yet
- Portal Hypertension AssignmentDocument8 pagesPortal Hypertension AssignmentAhmed ImranNo ratings yet
- Cirrhosis and Its ComplicationsDocument3 pagesCirrhosis and Its ComplicationsMahaNo ratings yet
- Upper Gastrointestinal Bleeding: Anthony Alexander University of The West Indies at MonaDocument40 pagesUpper Gastrointestinal Bleeding: Anthony Alexander University of The West Indies at MonaAy Alex0% (1)
- Portal hypertension diagnosis and managementDocument23 pagesPortal hypertension diagnosis and managementSumathi Gopinath100% (1)
- Portal HypertensionDocument60 pagesPortal HypertensionParul VarshneyNo ratings yet
- 09 Portal HypertensionDocument51 pages09 Portal HypertensionAna TudosieNo ratings yet
- Portal HypertensionDocument103 pagesPortal Hypertensionsolysan50% (2)
- UGIB HanifDocument90 pagesUGIB HanifHanif KhairudinNo ratings yet
- Acute Gastrointestinal Bleeding GuideDocument47 pagesAcute Gastrointestinal Bleeding GuideJohn Clements Galiza100% (1)
- Portal HypertensionDocument65 pagesPortal HypertensionVenu MadhavNo ratings yet
- Portal Hypertension: Gabriel Quah Group 86Document12 pagesPortal Hypertension: Gabriel Quah Group 86bryan-teoh-9027No ratings yet
- Acute Renal FailureDocument31 pagesAcute Renal FailureODONG MARTINNo ratings yet
- Portal HypertensionDocument22 pagesPortal Hypertensionsara.sherif099No ratings yet
- Prepared by Inzar Yasin Ammar LabibDocument47 pagesPrepared by Inzar Yasin Ammar LabibdiaNo ratings yet
- Major Complication of CirrhosisDocument6 pagesMajor Complication of CirrhosisAlya Putri KhairaniNo ratings yet
- Portal HypertensionDocument23 pagesPortal HypertensionSumathi GopinathNo ratings yet
- Gi Emergencies SeminarDocument122 pagesGi Emergencies SeminarShubham gaurNo ratings yet
- Approach To Acute Upper Gastrointestinal Bleeding in Adults - UpToDateDocument48 pagesApproach To Acute Upper Gastrointestinal Bleeding in Adults - UpToDateDũng Hoàng Nghĩa TríNo ratings yet
- Gastrointestinal Bleeding - StatPearls - NCBI BookshelfDocument7 pagesGastrointestinal Bleeding - StatPearls - NCBI BookshelfAdam GenturNo ratings yet
- IPD - SirosisDocument30 pagesIPD - SirosisRahmat AzimiNo ratings yet
- Esophageal VaricesDocument4 pagesEsophageal VaricesSnapeSnapeNo ratings yet
- Esophageal varicesDocument12 pagesEsophageal varicesgemergencycareNo ratings yet
- Managing Upper GI BleedingDocument20 pagesManaging Upper GI BleedingMoses Jr KazevuNo ratings yet
- Liver CirrhosisDocument9 pagesLiver CirrhosismedsmracelisNo ratings yet
- Upper Gi BleedDocument43 pagesUpper Gi BleedPreethi GudipalliNo ratings yet
- Nursing Management of Portal HypertensionDocument32 pagesNursing Management of Portal HypertensionPoova RagavanNo ratings yet
- Gastroesophagal VaricesDocument21 pagesGastroesophagal VaricesNurulasyikin MAANo ratings yet
- Manage Upper GI Bleed in 33yo Hotel ReceptionistDocument42 pagesManage Upper GI Bleed in 33yo Hotel ReceptionistMuhammad Naveed AslamNo ratings yet
- Esophageal and Gastric VaricesDocument15 pagesEsophageal and Gastric VaricesDumbo D' CatNo ratings yet
- Acute Liver Failure-1Document40 pagesAcute Liver Failure-1elizabethNo ratings yet
- Indications For TransplantDocument4 pagesIndications For TransplantDorina EfrosNo ratings yet
- Rami Dwairi, MD: Internal Medicine, HSDocument22 pagesRami Dwairi, MD: Internal Medicine, HSraed faisalNo ratings yet
- Pathohysiology of Ascites: Waleed Al-HamoudiDocument36 pagesPathohysiology of Ascites: Waleed Al-Hamoudiarina31No ratings yet
- VaricesDocument34 pagesVaricesapi-19641337No ratings yet
- Perdarahan Saluran Cerna Bagian Atas (SCBA) : HAM. AkilDocument43 pagesPerdarahan Saluran Cerna Bagian Atas (SCBA) : HAM. AkilEmeraldyModyNo ratings yet
- Sirosis Hepatis: Sigit Widyatmoko Fakultas Kedokteran UMSDocument66 pagesSirosis Hepatis: Sigit Widyatmoko Fakultas Kedokteran UMSArif Rahman DmNo ratings yet
- Liver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisDocument35 pagesLiver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisMohd Johari Mohd ShafuwanNo ratings yet
- Portal Hypertension in Adults - UpToDateDocument14 pagesPortal Hypertension in Adults - UpToDateEdwin VileloNo ratings yet
- Cirrhosis and Its Complications Part 1 LenchoDocument76 pagesCirrhosis and Its Complications Part 1 Lenchoosman nurNo ratings yet
- Gastric Emergencies: Principles of Critical Care ModuleDocument32 pagesGastric Emergencies: Principles of Critical Care ModuleDeni AdriansyahNo ratings yet
- Portal Hypertension and AscitesDocument5 pagesPortal Hypertension and AscitesHưng Nguyễn KiềuNo ratings yet
- 1.5 - GI BleedingDocument2 pages1.5 - GI BleedingFlowerNo ratings yet
- Portal Vein Thrombosis Should We Bust The Clot?: Dr. Mohammed Said Noor Fy1 Mr. Esam Aboutaleb SPRDocument33 pagesPortal Vein Thrombosis Should We Bust The Clot?: Dr. Mohammed Said Noor Fy1 Mr. Esam Aboutaleb SPREsam AboutalebNo ratings yet
- GI Bleeding Causes, Risk Factors, Diagnosis and ManagementDocument32 pagesGI Bleeding Causes, Risk Factors, Diagnosis and Managementmohamedeen hamzaNo ratings yet
- W J C M P R: Orld Ournal of Urrent Edical and Harmaceutical EsearchDocument3 pagesW J C M P R: Orld Ournal of Urrent Edical and Harmaceutical EsearchVivi DeviyanaNo ratings yet
- Mu 35Document7 pagesMu 35Trung TạNo ratings yet
- Differential Diagnosis of Neck Swellings PDFDocument3 pagesDifferential Diagnosis of Neck Swellings PDFSiddharth KatyalNo ratings yet
- 2.15 Interpretasi Darah 3 Sudah Di Stabilo PDFDocument1 page2.15 Interpretasi Darah 3 Sudah Di Stabilo PDFalodiaNo ratings yet
- Chronic Mesenteric IschaemiaDocument2 pagesChronic Mesenteric IschaemiaMike GNo ratings yet
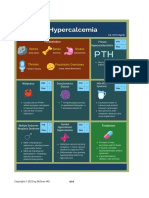
- HypercalcemiaDocument1 pageHypercalcemiaMike GNo ratings yet
- Neuro Dementia 2022Document5 pagesNeuro Dementia 2022Mike GNo ratings yet
- Immediate management of life-threatening abdominal problemsDocument3 pagesImmediate management of life-threatening abdominal problemsMike GNo ratings yet
- Approach To Jundiced PatientDocument2 pagesApproach To Jundiced Patientmelinda SilalahiNo ratings yet
- Antaomy of GITDocument5 pagesAntaomy of GITMike GNo ratings yet
- CBC DiffDocument8 pagesCBC DiffMike GNo ratings yet
- Classification of ShockDocument3 pagesClassification of ShockYogi drNo ratings yet
- Solid Visceral Injuries Solid Visceral Injuries Solid Visceral InjuriesDocument2 pagesSolid Visceral Injuries Solid Visceral Injuries Solid Visceral InjuriesMike GNo ratings yet
- Gastrointestinal Bleeding PDFDocument1 pageGastrointestinal Bleeding PDFYogi drNo ratings yet
- Thyroid Gland MCQ: The Ultimate QuizDocument17 pagesThyroid Gland MCQ: The Ultimate QuizMike GNo ratings yet
- Acute Coronary SyndromeDocument1 pageAcute Coronary SyndromeMike GNo ratings yet
- Small Intenstine MedCosmos Surgery - MCQDocument29 pagesSmall Intenstine MedCosmos Surgery - MCQMike GNo ratings yet
- Vascular Surgery MedCosmos Surgery - MCQDocument34 pagesVascular Surgery MedCosmos Surgery - MCQMike GNo ratings yet
- Chapter 33 Plastic and Reconstructive SurgeryDocument4 pagesChapter 33 Plastic and Reconstructive SurgeryMike GNo ratings yet
- Stomach-Esophagus MedCosmos Surgery - MCQDocument39 pagesStomach-Esophagus MedCosmos Surgery - MCQMike G100% (1)
- Trauma and Burns MedCosmos Surgery - MCQDocument32 pagesTrauma and Burns MedCosmos Surgery - MCQMike GNo ratings yet
- Chapter 34 Pediatric SurgeryDocument11 pagesChapter 34 Pediatric SurgeryMike G100% (1)
- Spleen MedCosmos Surgery - MCQDocument11 pagesSpleen MedCosmos Surgery - MCQMike GNo ratings yet
- Chapter 1 Cell Physiology and StructureDocument4 pagesChapter 1 Cell Physiology and StructureMike GNo ratings yet
- Chapter 36 Intracranial and Spinal TraumaDocument5 pagesChapter 36 Intracranial and Spinal TraumaMike GNo ratings yet
- Chapter 2 Surgical NutritionDocument3 pagesChapter 2 Surgical NutritionMike GNo ratings yet
- Section 11 - Selected Topics in General and Internal MedicineDocument65 pagesSection 11 - Selected Topics in General and Internal MedicineMike GNo ratings yet
- Chapter 39 Obstetrics and GynecologyDocument3 pagesChapter 39 Obstetrics and GynecologyMike GNo ratings yet
- Chapter 35 NeurosurgeryDocument11 pagesChapter 35 NeurosurgeryMike GNo ratings yet
- Chapter 60: Headache: Section 10: NeurologyDocument16 pagesChapter 60: Headache: Section 10: NeurologyAnonymous Xmb6QQvRNo ratings yet
- Hopkins Medicine Review Oncology Section PDFDocument39 pagesHopkins Medicine Review Oncology Section PDFaliaaNo ratings yet
- Hopkins Medicine Review HematologyDocument35 pagesHopkins Medicine Review HematologyGuna Babu100% (1)
- Why Do We Digest LowerDocument2 pagesWhy Do We Digest LowerSaima UsmanNo ratings yet
- Hemorrhoidectomy: Prepared By: Kristine Anne M. Lacorte BSN Iii-CDocument13 pagesHemorrhoidectomy: Prepared By: Kristine Anne M. Lacorte BSN Iii-CRita Honrade HernandezNo ratings yet
- ApdDocument33 pagesApdPriyanka Jose100% (1)
- OmeprazoleDocument2 pagesOmeprazoleBASHArnNo ratings yet
- Obscure Gi BleedingDocument76 pagesObscure Gi Bleedingbittuhimi24No ratings yet
- July 27, 2009 Exploratory Laparotomy and Transverse Loop Colostomy 1.Document8 pagesJuly 27, 2009 Exploratory Laparotomy and Transverse Loop Colostomy 1.MaRVNo ratings yet
- Gastric Outlet Obstruction: Its Surgical ManagementDocument40 pagesGastric Outlet Obstruction: Its Surgical ManagementGudeta shegerNo ratings yet
- Small Bowel Obstruction System - DisorderDocument1 pageSmall Bowel Obstruction System - DisorderMarina Wasem Netzlaff0% (1)
- Colorectal CancerDocument48 pagesColorectal CancerAndre F SusantioNo ratings yet
- Gastroenterology: Student NameDocument8 pagesGastroenterology: Student Namemishal zikriaNo ratings yet
- The Digestive System and its ProcessesDocument5 pagesThe Digestive System and its ProcessesRavenApigoNo ratings yet
- PeritoneumDocument39 pagesPeritoneumtuhinsinghNo ratings yet
- Salivary GlandDocument38 pagesSalivary GlandWasfe BarzaqNo ratings yet
- PneumoperitoneumDocument15 pagesPneumoperitoneumMuhammad Dimas PangestuNo ratings yet
- Fulminant Hepatic FailureDocument10 pagesFulminant Hepatic FailureAira Anne Tonee VillaminNo ratings yet
- Hemorragia Digestiva Baja: Lower Gastrointestinal BleedingDocument6 pagesHemorragia Digestiva Baja: Lower Gastrointestinal BleedingwiwiNo ratings yet
- Case Write Up SURGERYDocument14 pagesCase Write Up SURGERYRahul Audenesen50% (2)
- Routine Fecalysis Stool Analysis: Is A Series of Tests Done On A Stool Sample To Help Diagnose Certain ConditionsDocument3 pagesRoutine Fecalysis Stool Analysis: Is A Series of Tests Done On A Stool Sample To Help Diagnose Certain ConditionsSheila GarciaNo ratings yet
- Digestive System: MouthDocument3 pagesDigestive System: MouthTOt's VinNo ratings yet
- Management of common breast conditionsDocument122 pagesManagement of common breast conditionsﻋﻤﻴﺪ ﺍﻟﺸﻤﻴﺮﻱNo ratings yet
- Getting Foods To Cell 1Document4 pagesGetting Foods To Cell 1ScatchJhel PascuaNo ratings yet
- Reduce Risk of Stomach Ulcers and Gastritis - Life ExtensionDocument8 pagesReduce Risk of Stomach Ulcers and Gastritis - Life ExtensionŞtefan PtrtuNo ratings yet
- Which of Following Processes Is The Function of The Smooth Muscle Layer of The Digestive SystemDocument31 pagesWhich of Following Processes Is The Function of The Smooth Muscle Layer of The Digestive SystemCatherine LoyolaNo ratings yet
- Royal Government of Bhutan Jigme Dorji Wangchuk National Referral Hospital Patient Discharge FormDocument1 pageRoyal Government of Bhutan Jigme Dorji Wangchuk National Referral Hospital Patient Discharge FormSuman Pradhan 2803No ratings yet
- Digestive System: Reported By:Era Denise A. Allego & Yleah Kyla D. SoletaDocument28 pagesDigestive System: Reported By:Era Denise A. Allego & Yleah Kyla D. SoletaEnerita AllegoNo ratings yet
- Hirschsprung Disease: A Congenital Birth Defect of the IntestinesDocument3 pagesHirschsprung Disease: A Congenital Birth Defect of the IntestinesJan Rae Barnatia AtienzaNo ratings yet
- Digestive System: Nur Rahimatul Hayati Binti Abdul Rahman Centre of Foundation Studies UitmDocument54 pagesDigestive System: Nur Rahimatul Hayati Binti Abdul Rahman Centre of Foundation Studies UitmNadiah RahmanNo ratings yet
- Lasunadi Vati Health Benefits - Bimbima PDFDocument6 pagesLasunadi Vati Health Benefits - Bimbima PDFamjadNo ratings yet
- Helicobacter Pylori Infection - Recent Developments in DiagnosisDocument16 pagesHelicobacter Pylori Infection - Recent Developments in DiagnosisRima Carolina Bahsas ZakyNo ratings yet
- LiverDocument3 pagesLiverrahniNo ratings yet