You might also like
- Photosensitizing Medication ListDocument3 pagesPhotosensitizing Medication ListDimas RfNo ratings yet
- Materi 1 Dr. Apt. Diana Laila Ramatillah, M.farmDocument32 pagesMateri 1 Dr. Apt. Diana Laila Ramatillah, M.farmDimas RfNo ratings yet
- Pedia Drugs and Dosages SlidesDocument25 pagesPedia Drugs and Dosages SlidesWipaporn ChaengsriNo ratings yet
- Antimicrobial Stewardship Program1Document29 pagesAntimicrobial Stewardship Program1esNo ratings yet
- Dr. Ronald Irwanto Natadidjaja, SPPD - Kpti, Finasim: NamaDocument28 pagesDr. Ronald Irwanto Natadidjaja, SPPD - Kpti, Finasim: Namasri handayaniNo ratings yet
- 09 Gyssens PDFDocument45 pages09 Gyssens PDFTjoe DongNo ratings yet
- Wiser Choice of Antibiotic From Bench To Bedside and Back Again - Sri Rezeki HadinegoroDocument35 pagesWiser Choice of Antibiotic From Bench To Bedside and Back Again - Sri Rezeki HadinegoroIfah Inayah D'zatrichaNo ratings yet
- Humanimmunodeficiency Virusinitialassessmentand Routinefollow-UpDocument16 pagesHumanimmunodeficiency Virusinitialassessmentand Routinefollow-UpBriando Stevano LinelejanNo ratings yet
- 02b.terapi Infeksi AnakDocument32 pages02b.terapi Infeksi AnakIrvan KhairudinNo ratings yet
- Module 1. Overview of HIV Testing TechnologyDocument37 pagesModule 1. Overview of HIV Testing TechnologyZemen AddisNo ratings yet
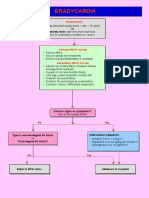
- BradycardiaDocument1 pageBradycardiaVeranika SelviyaNo ratings yet
- Nicu Neonatal Pneumonia ArticleDocument13 pagesNicu Neonatal Pneumonia ArticleJomer HeyresNo ratings yet
- Updated Covid-19 Protocols: Based On The Latest Guidelines From Doh, Psmid, CDC and WhoDocument62 pagesUpdated Covid-19 Protocols: Based On The Latest Guidelines From Doh, Psmid, CDC and WhoN CNo ratings yet
- Cervical Cancer Pandemic Impact - 05Document23 pagesCervical Cancer Pandemic Impact - 05Masrum ThamrinNo ratings yet
- Gyssen DDD MethodDocument39 pagesGyssen DDD MethodDewi RinakantiNo ratings yet
- HIV VS COVID - Dr. Christine, SP - PK (K)Document57 pagesHIV VS COVID - Dr. Christine, SP - PK (K)Rizki AdriansyahNo ratings yet
- PhysioEx Exercise 12 Activity 4Document3 pagesPhysioEx Exercise 12 Activity 4t4gjzhpfjcNo ratings yet
- Journal Reading EASL 2017 Clinical Practice Guidlines On The Management of Hepatitis B Virus InfectionDocument34 pagesJournal Reading EASL 2017 Clinical Practice Guidlines On The Management of Hepatitis B Virus InfectionSabrinaQurrotaayunNo ratings yet
- Surgical Site Infection Investigation Tool: AHRQ Safety Program For SurgeryDocument5 pagesSurgical Site Infection Investigation Tool: AHRQ Safety Program For SurgeryDewi ListyoriniNo ratings yet
- Report 2Document3 pagesReport 2kthandaveswaranNo ratings yet
- Heaptobiliary Disease by Lecturio.Document106 pagesHeaptobiliary Disease by Lecturio.louisegantierNo ratings yet
- Hepatitis B Case StudiesDocument26 pagesHepatitis B Case StudieswqmxmNo ratings yet
- Topic 6 HIV DiagnosisDocument30 pagesTopic 6 HIV DiagnosisPhilip MutuaNo ratings yet
- (MATERI 1) NEW ATIRETROVIRAL REGIMENS in HIV THERAPYDocument22 pages(MATERI 1) NEW ATIRETROVIRAL REGIMENS in HIV THERAPYJihanNo ratings yet
- Sensing Self COVID-19 Rapid Test KitDocument1 pageSensing Self COVID-19 Rapid Test KittattvanishthaNo ratings yet
- Weekly Case ReportDocument6 pagesWeekly Case ReportAyat AlshawayNo ratings yet
- Penny R. Thayer, FNP, BC Gastro/Hepatology NP James H. Quillen, VAMCDocument27 pagesPenny R. Thayer, FNP, BC Gastro/Hepatology NP James H. Quillen, VAMCPatresya LantanNo ratings yet
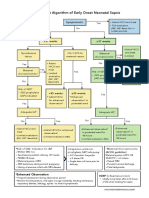
- Neonatal Sepsis Algorithm2Document1 pageNeonatal Sepsis Algorithm2CHIERBEENo ratings yet
- Hepatitis B Serologic Interpretation Policy Application 2022Document2 pagesHepatitis B Serologic Interpretation Policy Application 2022Brilliance M.No ratings yet
- F-Clinical Pre TreatmentDocument1 pageF-Clinical Pre Treatmenth gNo ratings yet
- Algoritma Tes HIVDocument31 pagesAlgoritma Tes HIVyurdiansyahNo ratings yet
- ACC/AHA Guidelines Stemi: DR Rajesh K FDocument84 pagesACC/AHA Guidelines Stemi: DR Rajesh K FFandi TriansyahNo ratings yet
- Resistance in HCV: Andrew J. Muir, MD MHSDocument33 pagesResistance in HCV: Andrew J. Muir, MD MHSEleni HagosNo ratings yet
- Stemi 4Document92 pagesStemi 4Abnet WondimuNo ratings yet
- Life CellDocument2 pagesLife CellSuman HazariNo ratings yet
- Pneumonia AdultDocument1 pagePneumonia AdultRoi LevinzonNo ratings yet
- Differences of Hap-Vap Guidelines in The Idsa 2005 and 2016Document13 pagesDifferences of Hap-Vap Guidelines in The Idsa 2005 and 2016Adeh MahardikaNo ratings yet
- Review Questions Unit 1 AnswerDocument4 pagesReview Questions Unit 1 Answerkoket negashNo ratings yet
- Asymptomatic Severe Moderate Mild: Comprehensive Guidelines For Management of COVID-19 PatientsDocument9 pagesAsymptomatic Severe Moderate Mild: Comprehensive Guidelines For Management of COVID-19 PatientsVaishnavi JayakumarNo ratings yet
- The HBV Pipeline and What The SIG Can OfferDocument29 pagesThe HBV Pipeline and What The SIG Can OfferTran Thanh NamNo ratings yet
- Pillar ComparisonDocument1 pagePillar ComparisonSatya PNo ratings yet
- Case Study CH 06Document13 pagesCase Study CH 06ashNo ratings yet
- Hepatitis B & C, Alamanda GarutDocument43 pagesHepatitis B & C, Alamanda GarutAndi Putra RegardboyNo ratings yet
- Daily Regimen Ant TB TreatmentDocument37 pagesDaily Regimen Ant TB TreatmentVidya Mohan KrithikanandNo ratings yet
- HBV Easl CPG Slide Deck 2020Document47 pagesHBV Easl CPG Slide Deck 2020Faheem Ul HasanNo ratings yet
- Acute & Chronic HepatitisDocument65 pagesAcute & Chronic HepatitisMahmoud AjinehNo ratings yet
- Ciw CellulitisDocument3 pagesCiw CellulitisEben Alameda-PalapuzNo ratings yet
- HepatitisDocument29 pagesHepatitisRose Anne AbivaNo ratings yet
- One Stop Model TB HIV IntegrationDocument1 pageOne Stop Model TB HIV IntegrationIGD PKMDobarNo ratings yet
- Tatalaksana ARV - Efek Samping - IRIS - Monitoring Terapi - PEPDocument95 pagesTatalaksana ARV - Efek Samping - IRIS - Monitoring Terapi - PEPtriiNo ratings yet
- 5.RTRI Principle and Performance 8may2019Document34 pages5.RTRI Principle and Performance 8may2019ABCDeNo ratings yet
- Chapter 5 - Mind Map PDFDocument1 pageChapter 5 - Mind Map PDFPhoenix Cassidy MotekeNo ratings yet
- 1 - PPT Dr. Agnes R. Indrati KONAS 2022Document33 pages1 - PPT Dr. Agnes R. Indrati KONAS 2022Mustakim DuharingNo ratings yet
- UK Biologics Checklist May 2014Document2 pagesUK Biologics Checklist May 2014Dr Sneha's Skin and Allergy Clinic IndiaNo ratings yet
- Nutritional Assessment TemplateDocument3 pagesNutritional Assessment TemplateScribdTranslationsNo ratings yet
- Form Evaluaso AmsDocument1 pageForm Evaluaso AmsNadial uzmahNo ratings yet
- Dr. Ikram: Dokter Internsip RSUD Teungku Rafi'an Siak Sri IndrapuraDocument31 pagesDr. Ikram: Dokter Internsip RSUD Teungku Rafi'an Siak Sri IndrapuraNovietha Lia FarizymelinNo ratings yet
- Hep ABC - Lab DiagnosisDocument15 pagesHep ABC - Lab DiagnosisjunaidiabdhalimNo ratings yet
- ZOOL 143 Topic 7 Detection of HIV Infection 1Document10 pagesZOOL 143 Topic 7 Detection of HIV Infection 1nattydreadfathelahNo ratings yet
- 7 Cases FungalDocument56 pages7 Cases Fungalkoteshwara raoNo ratings yet
- Recent Advance of Chronic Hepatitis B TreatmentDocument28 pagesRecent Advance of Chronic Hepatitis B Treatmentbudi darmantaNo ratings yet
- General Characteristics of VirusesDocument3 pagesGeneral Characteristics of VirusesS. C.No ratings yet
- Helwig 2019Document9 pagesHelwig 2019Dimas RfNo ratings yet
- 1071 FullDocument11 pages1071 FullDimas RfNo ratings yet
- CMH 612Document8 pagesCMH 612Dimas RfNo ratings yet
- Opinion of The Scientific Steering Committee ON: European CommissionDocument121 pagesOpinion of The Scientific Steering Committee ON: European CommissionDimas RfNo ratings yet
- Guidelines For Prevention and Control of Infections Due To Antibiotic-Resistant OrganismsDocument62 pagesGuidelines For Prevention and Control of Infections Due To Antibiotic-Resistant OrganismsDimas RfNo ratings yet
- Hospital Antibiotic Policy: ST Helens and Knowsley Hospitals TrustDocument72 pagesHospital Antibiotic Policy: ST Helens and Knowsley Hospitals TrustDimas RfNo ratings yet
- Dmso 7 553Document11 pagesDmso 7 553Dimas RfNo ratings yet
- 5 6059713553416323809Document351 pages5 6059713553416323809Dimas RfNo ratings yet
- Cost Effectiveness of Hmg-Coa Reductase Inhibitor (Statin) Treatment Related To The Risk of Coronary Heart Disease and Cost of Drug TreatmentDocument9 pagesCost Effectiveness of Hmg-Coa Reductase Inhibitor (Statin) Treatment Related To The Risk of Coronary Heart Disease and Cost of Drug TreatmentDimas RfNo ratings yet
- The Control and Prevention of MRSA in Hospitals and in The CommunityDocument41 pagesThe Control and Prevention of MRSA in Hospitals and in The CommunityDimas RfNo ratings yet
- Infection Control Programmes To Control Antimicrobial ResistanceDocument53 pagesInfection Control Programmes To Control Antimicrobial ResistanceDimas RfNo ratings yet
- Pharm Stroke: Care PadaDocument38 pagesPharm Stroke: Care PadaDimas RfNo ratings yet
- Sharing Experience: Oncology Pharmacy Practice in IndonesiaDocument23 pagesSharing Experience: Oncology Pharmacy Practice in IndonesiaDimas RfNo ratings yet
- Slowing Down Superbugs: Legislation and Antimicrobial Resistance (AMR)Document36 pagesSlowing Down Superbugs: Legislation and Antimicrobial Resistance (AMR)Dimas RfNo ratings yet
- Moisturizer and Corticosteroid For Atopic Dermatitis: DR. Dr. FX Wikan Indarto, Sp.ADocument22 pagesMoisturizer and Corticosteroid For Atopic Dermatitis: DR. Dr. FX Wikan Indarto, Sp.ADimas RfNo ratings yet
- Food and Health in Europe:: WHO Regional Publications European Series, No. 96Document405 pagesFood and Health in Europe:: WHO Regional Publications European Series, No. 96Dimas RfNo ratings yet
- A Milestone in Codifying The Wisdom of Traditional Oriental Medicine: TCM, Kampo, TKM, TVM-WHO International Standard Terminologies On Traditional Medicine in The Western Pacific RegionDocument3 pagesA Milestone in Codifying The Wisdom of Traditional Oriental Medicine: TCM, Kampo, TKM, TVM-WHO International Standard Terminologies On Traditional Medicine in The Western Pacific RegionDimas RfNo ratings yet
- Summary of NAP Implementation ReviewDocument29 pagesSummary of NAP Implementation ReviewDimas RfNo ratings yet
- Antibiotic Prophylaxis in Surgery: A National Clinical GuidelineDocument78 pagesAntibiotic Prophylaxis in Surgery: A National Clinical GuidelineDimas RfNo ratings yet
- Employing Pharmacokinetic and Pharmacodynamic Principles To Optimize Antimicrobial Treatment in The Face of Emerging ResistanceDocument11 pagesEmploying Pharmacokinetic and Pharmacodynamic Principles To Optimize Antimicrobial Treatment in The Face of Emerging ResistanceDimas RfNo ratings yet
- Xarelto Tablet Salut Selaput 20 MG - Rivaroksaban - DKI1251602517C1 - 2020Document26 pagesXarelto Tablet Salut Selaput 20 MG - Rivaroksaban - DKI1251602517C1 - 2020Dimas RfNo ratings yet
- Nurse Perspective of Hajj Pilgrims Health Management in Response To A New Emerging Disease.Document17 pagesNurse Perspective of Hajj Pilgrims Health Management in Response To A New Emerging Disease.Dimas RfNo ratings yet
- 10.1055@s 0031 1300449Document6 pages10.1055@s 0031 1300449Dimas RfNo ratings yet
- Ismr Update: Gram-Positive Antibiotic Selection: PK/PD ConsiderationsDocument16 pagesIsmr Update: Gram-Positive Antibiotic Selection: PK/PD ConsiderationsDimas RfNo ratings yet
- en Potensi Kejadian Interaksi Obat Pada PenDocument3 pagesen Potensi Kejadian Interaksi Obat Pada PenDimas RfNo ratings yet
- Preanaesthetic Medication Anaesthetic AgentsDocument35 pagesPreanaesthetic Medication Anaesthetic AgentsSubhash BeraNo ratings yet
- Nebulizer ProcedureDocument2 pagesNebulizer Procedureralph_gailNo ratings yet
- Syllabus Refreshing of First Aid Intermediate Level For Synthetic Rubber Indonesia Security TeamDocument5 pagesSyllabus Refreshing of First Aid Intermediate Level For Synthetic Rubber Indonesia Security TeamRobbyAjiAryaNo ratings yet
- Betahistine (DRUG LIST)Document2 pagesBetahistine (DRUG LIST)Bon- BonNo ratings yet
- Clini India SyllabusDocument7 pagesClini India SyllabusYash DevrukhkarNo ratings yet
- Ventilator Graphics PDFDocument30 pagesVentilator Graphics PDFRina AnggrainiNo ratings yet
- 1 Analgetik Ketorolac: No Golongan Obat Nama GenerikDocument44 pages1 Analgetik Ketorolac: No Golongan Obat Nama GenerikHayu Ajeng A RNo ratings yet
- Intern Drug ListDocument5 pagesIntern Drug ListKenette Diane CantubaNo ratings yet
- Pharmacist Role in ADR MDocument9 pagesPharmacist Role in ADR Mimran moopansNo ratings yet
- Lista 25 Febrero Cobefar - WismanDocument64 pagesLista 25 Febrero Cobefar - WismanLincoln López GodoyNo ratings yet
- Hypnotherapy For Happiness (For Everybody) : PrefaceDocument1 pageHypnotherapy For Happiness (For Everybody) : PrefaceLaura PNo ratings yet
- XXXXXXXXXXXXXXXXXXDocument36 pagesXXXXXXXXXXXXXXXXXXkhraieric16No ratings yet
- Form Standarisasi BMHP RSU Jampang Kulon 2020Document6 pagesForm Standarisasi BMHP RSU Jampang Kulon 2020Avrilia Fuji AstutiNo ratings yet
- Current Application of Cannabidiol (CBD) in The Management and Treatment of Neurological DisordersDocument14 pagesCurrent Application of Cannabidiol (CBD) in The Management and Treatment of Neurological Disorderssara laadamiNo ratings yet
- Drug Study: Midazolam: RecommendedDocument5 pagesDrug Study: Midazolam: RecommendedShara Lailanie A. AzisNo ratings yet
- Green Pharmacy - A Narrative ReviewDocument8 pagesGreen Pharmacy - A Narrative ReviewCHATHUMI WEERAKOONNo ratings yet
- Roxonin LeafletDocument2 pagesRoxonin LeafletmohammedfirasatNo ratings yet
- Poster Clinical Investigation of Magic Ring (Modified Plastibell Device) For CircumcisionDocument1 pagePoster Clinical Investigation of Magic Ring (Modified Plastibell Device) For CircumcisionLutfi Aulia RahmanNo ratings yet
- NNF Ready ReckonerDocument6 pagesNNF Ready ReckonerKicku100% (1)
- Sheet 2 (Local Anesthesia 2)Document14 pagesSheet 2 (Local Anesthesia 2)ardesh abdilleNo ratings yet
- Ethical Use of CannabisDocument3 pagesEthical Use of CannabisMile PrikopNo ratings yet
- Julho - 22 Us CoachDocument7 pagesJulho - 22 Us CoachPantajr - GTR250No ratings yet
- Hospital Pharmacy: Birla Institute of Technology & Science Pilani, Hyderabad CampusDocument37 pagesHospital Pharmacy: Birla Institute of Technology & Science Pilani, Hyderabad CampusAshiff Shaik100% (2)
- Presentation Regulators Perspective Session 2 Keith Pugh - enDocument15 pagesPresentation Regulators Perspective Session 2 Keith Pugh - enAshishShuklaNo ratings yet
- Pediatric Medication Calculations: UNRS 314 Jan Bazner-Chandler CPNP, CNS, MSN, RNDocument47 pagesPediatric Medication Calculations: UNRS 314 Jan Bazner-Chandler CPNP, CNS, MSN, RNHunny BearstenNo ratings yet
- Licorice Root On Burn HealingDocument19 pagesLicorice Root On Burn HealingAbang OzielNo ratings yet
- Guidelines On The Management of Postoperative PainDocument38 pagesGuidelines On The Management of Postoperative PainIeyna Key Nor Azmina100% (1)
- Perspective LawsDocument3 pagesPerspective LawsJenilyn FarnacioNo ratings yet
- Daftar Obat High Alert Royal MaternityyDocument1 pageDaftar Obat High Alert Royal Maternityydiffa rahmaNo ratings yet