You might also like
- Surgical Site InfectionDocument8 pagesSurgical Site Infection1234chocoNo ratings yet
- Monitoring The One Year Postoperative Infection Rate After Primary Total Hip ReplacementDocument7 pagesMonitoring The One Year Postoperative Infection Rate After Primary Total Hip ReplacementChebbah MahmoudNo ratings yet
- Does An Antimicrobial Incision Drape Prevent.15Document9 pagesDoes An Antimicrobial Incision Drape Prevent.15Jimenez-Espinosa JeffersonNo ratings yet
- Surgery JournalDocument7 pagesSurgery JournalJane Arian BerzabalNo ratings yet
- Predictors of Surgical Site InfectionsDocument7 pagesPredictors of Surgical Site InfectionsMageNo ratings yet
- Surgical Site Infections Latest Literature Update March 2019Document42 pagesSurgical Site Infections Latest Literature Update March 2019shah hassaanNo ratings yet
- 61140352Document6 pages61140352Febri Nick Daniel SihombingNo ratings yet
- SsiDocument8 pagesSsim8wyb2f6ngNo ratings yet
- 4147 15918 1 PBDocument7 pages4147 15918 1 PBI Made AryanaNo ratings yet
- 1 s2.0 S0039606007003480 MainDocument8 pages1 s2.0 S0039606007003480 MainAna MîndrilăNo ratings yet
- Chaptre 1 Evidence-Based Principles and Practices For Preoperative Preventing Surgical Site InfectionsDocument92 pagesChaptre 1 Evidence-Based Principles and Practices For Preoperative Preventing Surgical Site InfectionsAbdelrahman GameelNo ratings yet
- 3avijeet EtalDocument9 pages3avijeet EtaleditorijmrhsNo ratings yet
- Prognostic FactorDocument8 pagesPrognostic FactorMarno TakaNo ratings yet
- Surgical Site InfectionDocument7 pagesSurgical Site InfectionCaxton ThumbiNo ratings yet
- Postoperative Infection and Mortality Following Elective Surgery in The International Surgical Outcomes Study (ISOS)Document32 pagesPostoperative Infection and Mortality Following Elective Surgery in The International Surgical Outcomes Study (ISOS)Antonio Carlos Betanzos PlanellNo ratings yet
- Surgical Site Infection After Groin Hernia RepairDocument7 pagesSurgical Site Infection After Groin Hernia Repairيحيى الجبليNo ratings yet
- Incidence of Wound Sepsis and Related Factors in Post-Operative Patients in Kampala International University Teaching Hospital Ishaka Bushenyi-Western UganDocument12 pagesIncidence of Wound Sepsis and Related Factors in Post-Operative Patients in Kampala International University Teaching Hospital Ishaka Bushenyi-Western UganKIU PUBLICATION AND EXTENSIONNo ratings yet
- Post Caesarean Surgical Site Infections 2Document6 pagesPost Caesarean Surgical Site Infections 2saryindrianyNo ratings yet
- Prevention of Surgical Site InfectionDocument10 pagesPrevention of Surgical Site InfectionValiant Baybay100% (1)
- Predictors of SSI in Laparoscopic and Open Ventral Hernia RepairDocument6 pagesPredictors of SSI in Laparoscopic and Open Ventral Hernia RepairJose Manuel Luna VazquezNo ratings yet
- Effectiveness of A Multidisciplinary Patient Care Bundle For Reducing Surgical-Site InfectionsDocument8 pagesEffectiveness of A Multidisciplinary Patient Care Bundle For Reducing Surgical-Site InfectionsNurul AidaNo ratings yet
- Faktor Resiko Infeksi SCDocument11 pagesFaktor Resiko Infeksi SCAlberto BrahmNo ratings yet
- Antimicrobial Prophylaxis For Prevention of Surgical Site Infection in AdultsDocument59 pagesAntimicrobial Prophylaxis For Prevention of Surgical Site Infection in Adultsbolohan biatriceNo ratings yet
- Journal Surg Ward BorjaDocument4 pagesJournal Surg Ward BorjaYana PotNo ratings yet
- Antibiotic Prophylaxis in Elective Soft Tissue Hand SurgeryDocument5 pagesAntibiotic Prophylaxis in Elective Soft Tissue Hand SurgeryAnshar_nitroNo ratings yet
- DE LA CRUZ Prevención de Infección Del Sitio Quirúrgico - ArtDocument6 pagesDE LA CRUZ Prevención de Infección Del Sitio Quirúrgico - ArtJOSE FERNANDO DE LA CRUZ SILVANNo ratings yet
- Articulo 2019Document8 pagesArticulo 2019Felicia FernandezNo ratings yet
- Isid Guide Preparing The Patient For Surgery-1Document16 pagesIsid Guide Preparing The Patient For Surgery-1Prunaru BogdanNo ratings yet
- Surgical Site Infection in General Surgery: September 2015Document8 pagesSurgical Site Infection in General Surgery: September 2015Olifvia IntariNo ratings yet
- rgj9w7Document8 pagesrgj9w7Stella SulartoNo ratings yet
- Incidence of Surgical Site Infection in Abdominal Surgery in A Tertiaty Care Center in AssamDocument6 pagesIncidence of Surgical Site Infection in Abdominal Surgery in A Tertiaty Care Center in AssamIJAR JOURNALNo ratings yet
- Hospital Acquired Infection Incidence and Risk FactorsDocument7 pagesHospital Acquired Infection Incidence and Risk FactorsKshitiz112No ratings yet
- Screenshot 2022-09-26 at 20.14.44Document8 pagesScreenshot 2022-09-26 at 20.14.44Sutama ArtaNo ratings yet
- Saar 2016Document7 pagesSaar 2016iinmsNo ratings yet
- 10.1038@s41598 020 65019 8Document5 pages10.1038@s41598 020 65019 8bouchra8blsNo ratings yet
- Urquhart 2019Document9 pagesUrquhart 2019Vanessa DuzNo ratings yet
- Prevalence of Surgical Site Infections Among Surgical Operated Patients in Zewditu Memorial Hospital Addis Ababa EthiopiDocument10 pagesPrevalence of Surgical Site Infections Among Surgical Operated Patients in Zewditu Memorial Hospital Addis Ababa EthiopiAngelo Michilena100% (1)
- Study of Incidence and Risk Factors For Surgical Site Infection After Cesarean Section at First Referral UnitDocument3 pagesStudy of Incidence and Risk Factors For Surgical Site Infection After Cesarean Section at First Referral UnitFaozan FikriNo ratings yet
- Antibiotic Prophylaxis For Transurethral Urological Surgeries: Systematic ReviewDocument14 pagesAntibiotic Prophylaxis For Transurethral Urological Surgeries: Systematic ReviewFajrul Jawa'iNo ratings yet
- Post-Operative Wound Infection: A Surgeon'S Dilemma: Original ArticleDocument7 pagesPost-Operative Wound Infection: A Surgeon'S Dilemma: Original ArticlePetit-Paul WedlyNo ratings yet
- Case Study in Surgical First Assistant For NursesDocument13 pagesCase Study in Surgical First Assistant For NursesQuality ResearchNo ratings yet
- Les Infections Sur Protheses de Hanche: Quelle Strategie Therapeutique ?Document9 pagesLes Infections Sur Protheses de Hanche: Quelle Strategie Therapeutique ?IJAR JOURNALNo ratings yet
- Post-Operative Wound Complications Following Emergency and Elective Abdominal SurgeriesDocument6 pagesPost-Operative Wound Complications Following Emergency and Elective Abdominal SurgeriesNurul Aini DamayantiNo ratings yet
- Watanabe 2014Document6 pagesWatanabe 2014krittapas.9000No ratings yet
- IPAC Spring2018 Maciel de Castro Franco PDFDocument6 pagesIPAC Spring2018 Maciel de Castro Franco PDFKoKo TinNo ratings yet
- A Study of Prevalence and Root Causes of Surgical Site Infections in An Acute Care Facility in Sharjah, United Arab EmiratesDocument23 pagesA Study of Prevalence and Root Causes of Surgical Site Infections in An Acute Care Facility in Sharjah, United Arab EmiratesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 1 s2.0 S1078588413007946 Main 2Document7 pages1 s2.0 S1078588413007946 Main 2Saffa AzharaaniNo ratings yet
- Jkms 31 1963Document6 pagesJkms 31 1963Aura RivasNo ratings yet
- 001 Hipoglucemia NeonatalDocument6 pages001 Hipoglucemia NeonatalErick Lozada OlivaNo ratings yet
- Infection prevention imperative for perioperative safetyDocument3 pagesInfection prevention imperative for perioperative safetyKryza Dale Bunado BaticanNo ratings yet
- 1 s2.0 S0039606018302721 MainDocument7 pages1 s2.0 S0039606018302721 MainMelo Pérez Pamela J.No ratings yet
- Prophylactic Antibiotics before Gynecologic Surgery_ A Comprehensive Review of GuidelinesDocument18 pagesProphylactic Antibiotics before Gynecologic Surgery_ A Comprehensive Review of GuidelinesLuisa MorenoNo ratings yet
- Surgical Site Infection (Ssi 3)Document21 pagesSurgical Site Infection (Ssi 3)Shireen Qaiser100% (1)
- Surgical Site Infection Prevention Among Nursing Staff at Kampala International University Teaching Hospital Bushenyi, UgandaDocument33 pagesSurgical Site Infection Prevention Among Nursing Staff at Kampala International University Teaching Hospital Bushenyi, UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Y. AL HashmiDocument11 pagesY. AL HashmiAzam alausyNo ratings yet
- International Journal of Health Sciences and ResearchDocument8 pagesInternational Journal of Health Sciences and ResearchHàri HàránNo ratings yet
- 2019 Article 525Document8 pages2019 Article 525Diane MxNo ratings yet
- Predictors of Mesh Infection and Explantation After Abdominal Wall Hernia RepairDocument8 pagesPredictors of Mesh Infection and Explantation After Abdominal Wall Hernia RepairOtto NaftariNo ratings yet
- How Safe Are IV CannulaDocument4 pagesHow Safe Are IV CannulaDr Kadiyali M Srivatsa100% (2)
- Case Studies of Postoperative Complications after Digestive SurgeryFrom EverandCase Studies of Postoperative Complications after Digestive SurgeryNo ratings yet
- Classification of Compression Bandages PDocument10 pagesClassification of Compression Bandages Pbouchra8blsNo ratings yet
- Classification of Compression Bandages PDocument10 pagesClassification of Compression Bandages Pbouchra8blsNo ratings yet
- Compression Under Dynamic StateDocument15 pagesCompression Under Dynamic Statebouchra8blsNo ratings yet
- Characterization of Compression BandageDocument21 pagesCharacterization of Compression Bandagebouchra8blsNo ratings yet
- Dr. Lojpur - Dressing and BandageDocument9 pagesDr. Lojpur - Dressing and BandageJayvie Gacutan100% (1)
- Prevention of Hospital-Acquired Infections A Practical Guide 2nd EditionDocument72 pagesPrevention of Hospital-Acquired Infections A Practical Guide 2nd EditionAndreah YoungNo ratings yet
- Compression Under Dynamic StateDocument15 pagesCompression Under Dynamic Statebouchra8blsNo ratings yet
- Characterization of Compression BandageDocument21 pagesCharacterization of Compression Bandagebouchra8blsNo ratings yet
- Dr. Lojpur - Dressing and BandageDocument9 pagesDr. Lojpur - Dressing and BandageJayvie Gacutan100% (1)
- Mechanical Properties of Orthopedic Plaster Bandages : U.S.A. Robert E. Porter?Document14 pagesMechanical Properties of Orthopedic Plaster Bandages : U.S.A. Robert E. Porter?bouchra8blsNo ratings yet
- Nosocomial Infections Epidemiology Prevention Control and SurveillanceDocument21 pagesNosocomial Infections Epidemiology Prevention Control and SurveillanceFelicia BulaiNo ratings yet
- The Impact of Gown-Use Requirement On Hand Hygiene ComplianceDocument7 pagesThe Impact of Gown-Use Requirement On Hand Hygiene Compliancebouchra8blsNo ratings yet
- Haley 1991Document7 pagesHaley 1991bouchra8blsNo ratings yet
- The Impact of Gown-Use Requirement On Hand Hygiene ComplianceDocument7 pagesThe Impact of Gown-Use Requirement On Hand Hygiene Compliancebouchra8blsNo ratings yet
- To Lera 2020Document7 pagesTo Lera 2020bouchra8blsNo ratings yet
- Prevention of Hospital-Acquired Infections: Review of Non-Pharmacological InterventionsDocument16 pagesPrevention of Hospital-Acquired Infections: Review of Non-Pharmacological Interventionsbouchra8blsNo ratings yet
- Vieira 2011Document6 pagesVieira 2011bouchra8blsNo ratings yet
- Nosocomial Infections and Infection Control: What's New?Document5 pagesNosocomial Infections and Infection Control: What's New?bouchra8blsNo ratings yet
- Prevention of Hospital-Acquired Infections A Practical Guide 2nd EditionDocument72 pagesPrevention of Hospital-Acquired Infections A Practical Guide 2nd EditionAndreah YoungNo ratings yet
- Nosocomial Infections and Infection Control: What's New?Document5 pagesNosocomial Infections and Infection Control: What's New?bouchra8blsNo ratings yet
- Pediatric Protrusion Mentioned,: Robert M.D. CityDocument2 pagesPediatric Protrusion Mentioned,: Robert M.D. Citybouchra8blsNo ratings yet
- Chauveau X 2015Document7 pagesChauveau X 2015bouchra8blsNo ratings yet
- Chauveau X 2015Document7 pagesChauveau X 2015bouchra8blsNo ratings yet
- Face Masks and Respirators in The Fight Against The COVID-19 Pandemic: An Overview of The Standards and Testing MethodsDocument12 pagesFace Masks and Respirators in The Fight Against The COVID-19 Pandemic: An Overview of The Standards and Testing Methodsbouchra8blsNo ratings yet
- Prevention of Hospital-Acquired Infections: Review of Non-Pharmacological InterventionsDocument16 pagesPrevention of Hospital-Acquired Infections: Review of Non-Pharmacological Interventionsbouchra8blsNo ratings yet
- Chauveau X 2015Document7 pagesChauveau X 2015bouchra8blsNo ratings yet
- Pediatric Protrusion Mentioned,: Robert M.D. CityDocument2 pagesPediatric Protrusion Mentioned,: Robert M.D. Citybouchra8blsNo ratings yet
- Pediatric Protrusion Mentioned,: Robert M.D. CityDocument2 pagesPediatric Protrusion Mentioned,: Robert M.D. Citybouchra8blsNo ratings yet
- Nosocomial Infections and Infection Control: What's New?Document5 pagesNosocomial Infections and Infection Control: What's New?bouchra8blsNo ratings yet
- Prevention of Hospital-Acquired Infections: Review of Non-Pharmacological InterventionsDocument16 pagesPrevention of Hospital-Acquired Infections: Review of Non-Pharmacological Interventionsbouchra8blsNo ratings yet
- Sina Cheffer PDFDocument7 pagesSina Cheffer PDFCaroline RobisonNo ratings yet
- Specialized Group Homes For Persons With Severe or Profound Mental Retardation and Serious Problem Behaviour in EnglandDocument18 pagesSpecialized Group Homes For Persons With Severe or Profound Mental Retardation and Serious Problem Behaviour in EnglandDeborah RiskinNo ratings yet
- Catálogo de Dispositivos PQS 2014 PDFDocument318 pagesCatálogo de Dispositivos PQS 2014 PDFGestion Biomedica Prosalco IPSNo ratings yet
- Cardiac Marker Sem 5Document42 pagesCardiac Marker Sem 5novi pujiNo ratings yet
- SAS 6 - Abapo, Aquea B.Document5 pagesSAS 6 - Abapo, Aquea B.Aquea Bernardo AbapoNo ratings yet
- Msds Sodium HypochloriteDocument9 pagesMsds Sodium Hypochloritehinur awaNo ratings yet
- Emergency First Initial Assesment: Monday, October 05, 2020Document50 pagesEmergency First Initial Assesment: Monday, October 05, 2020Agoes TreeyantNo ratings yet
- First Responders: The Heroes Who Answer Emergency CallsDocument11 pagesFirst Responders: The Heroes Who Answer Emergency CallsDIANA MARIE MOTA ABREUNo ratings yet
- Baby Thesis RevisedDocument20 pagesBaby Thesis RevisedSanjoe Angelo ManaloNo ratings yet
- The Psychology of Ageing - An Introduction, 3rd EdDocument320 pagesThe Psychology of Ageing - An Introduction, 3rd Edfauziahfasya123No ratings yet
- Pharma Laboratory ExperimentsDocument34 pagesPharma Laboratory Experimentsapi-3748748100% (4)
- 2017 (Laporan Pelayanan Rawat Jalan Dr. Ida Ayu Anom Margareni)Document11 pages2017 (Laporan Pelayanan Rawat Jalan Dr. Ida Ayu Anom Margareni)Anggi RiyaniNo ratings yet
- Neet Ug Absolute Biology Vol 2Document22 pagesNeet Ug Absolute Biology Vol 2Rakesh Agarwal0% (1)
- PBL Modul 2 TropisDocument31 pagesPBL Modul 2 TropiskasmaNo ratings yet
- Does Masturbation Cause Acne in Men?Document3 pagesDoes Masturbation Cause Acne in Men?AndyJenkinsNo ratings yet
- The Psychodynamic Diagnostic Manual An Effort To Compensate For The Limitations of Descriptive Psychiatric Diagnosis (Mcwilliams2011)Document12 pagesThe Psychodynamic Diagnostic Manual An Effort To Compensate For The Limitations of Descriptive Psychiatric Diagnosis (Mcwilliams2011)Anastasiya PlohihNo ratings yet
- NCP Activity NavidasDocument2 pagesNCP Activity NavidasFran LanNo ratings yet
- Lessons For Financial Success CH 5 Productivity Capacity StaffingDocument41 pagesLessons For Financial Success CH 5 Productivity Capacity StaffingoggokNo ratings yet
- Identification and Typing of Pasteurella Multocida A ReviewDocument18 pagesIdentification and Typing of Pasteurella Multocida A Reviewsebasrd07No ratings yet
- Cardiopulmonary Resuscitation Update: Continuing Education ColumnDocument9 pagesCardiopulmonary Resuscitation Update: Continuing Education Columnkang soon cheolNo ratings yet
- Limited Uretheral Mobilization Procedure (Lump) For Distal Penile Hypospadias Repair, A Single Centre Retrospective AnalysisDocument9 pagesLimited Uretheral Mobilization Procedure (Lump) For Distal Penile Hypospadias Repair, A Single Centre Retrospective AnalysisIJAR JOURNALNo ratings yet
- Vaccine Excipient & Media Summary: Excipients Included in U.S. Vaccines, by VaccineDocument4 pagesVaccine Excipient & Media Summary: Excipients Included in U.S. Vaccines, by VaccineZeljko RasoNo ratings yet
- 07 - Towards Elimination DR Gottfried HirnschallDocument24 pages07 - Towards Elimination DR Gottfried HirnschallAjeet LohanaNo ratings yet
- Genetic Disorders: Chromosomal Abnormalities and Down SyndromeDocument27 pagesGenetic Disorders: Chromosomal Abnormalities and Down SyndromeMerwan KemalNo ratings yet
- Provisional Admit Card Cum Call LetterDocument3 pagesProvisional Admit Card Cum Call Lettersravikumar sNo ratings yet
- Guidelines for diagnosing and treating hypothyroidismDocument43 pagesGuidelines for diagnosing and treating hypothyroidismJoseAbdalaNo ratings yet
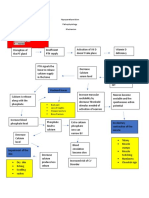
- Hypoparathyroidism PathophysiologyDocument1 pageHypoparathyroidism PathophysiologymaricarNo ratings yet
- Sexual Health Awareness ScaleDocument17 pagesSexual Health Awareness ScaleezazpsychologistNo ratings yet
- Heavenly Spa MenuDocument2 pagesHeavenly Spa MenuDeTaaliNo ratings yet
- Professional Foundation Level Acupressure Training CourseDocument94 pagesProfessional Foundation Level Acupressure Training CourseLuis Del Valle TorregrosaNo ratings yet