You might also like
- Abnormal Bleeding Anxiety/Depression High Blood Pressure Diabetes Autoimmune Disease Mood Swings Migraines SeizuresDocument2 pagesAbnormal Bleeding Anxiety/Depression High Blood Pressure Diabetes Autoimmune Disease Mood Swings Migraines SeizuresAnna Croox ReschNo ratings yet
- Marcias Esthetics Client Intake FormDocument4 pagesMarcias Esthetics Client Intake Formapi-194244218No ratings yet
- MediSpa Intake FormsDocument9 pagesMediSpa Intake FormsUtopiaawaitsNo ratings yet
- Facial Consultation CardDocument1 pageFacial Consultation CardHakan Ares Lazodobi100% (1)
- Client ConsultationForm Beauty V6 2021Document2 pagesClient ConsultationForm Beauty V6 2021Jeff SeaboardsNo ratings yet
- Lash Brow Tinting ConsentDocument1 pageLash Brow Tinting ConsentGGenZ ConsultingNo ratings yet
- Esthetician/paramedical AestheticianDocument2 pagesEsthetician/paramedical Aestheticianapi-121459287No ratings yet
- PCA Patient Checklist PDFDocument14 pagesPCA Patient Checklist PDFSuper SummonerNo ratings yet
- Disclosure and Consent For Intradermal Cosmetic ProceduresDocument2 pagesDisclosure and Consent For Intradermal Cosmetic Proceduresapi-3473912470% (1)
- Pre and After Care SPMDocument8 pagesPre and After Care SPMTana PeñaNo ratings yet
- What Are The Benefits of Dermaplaning and How Much Does It Cost?Document2 pagesWhat Are The Benefits of Dermaplaning and How Much Does It Cost?Daniel CalderonNo ratings yet
- Fabulous FacialsDocument3 pagesFabulous Facialssonyinn9058No ratings yet
- IPL Client History v1 - 7Document8 pagesIPL Client History v1 - 7Karen Dodd100% (1)
- Microneedling Consent Aftercare FormDocument5 pagesMicroneedling Consent Aftercare FormMalgorzata wojtowiczNo ratings yet
- Facial Intake Form: Personal InformationDocument6 pagesFacial Intake Form: Personal InformationCrystal-Jae0% (1)
- Skin Cleansing-Wps OfficeDocument4 pagesSkin Cleansing-Wps OfficeAngela AlejandroNo ratings yet
- Facial Aftercare AdviceDocument2 pagesFacial Aftercare AdvicerobertNo ratings yet
- Monu Manual Section 1Document20 pagesMonu Manual Section 1amymonuskinNo ratings yet
- Dermalogica Consult Card PDFDocument1 pageDermalogica Consult Card PDFTony AbottNo ratings yet
- Beauty Book 2010Document16 pagesBeauty Book 2010Linda Nakashima0% (1)
- SKIN DISORDERS AND DISEASES HandoutsDocument9 pagesSKIN DISORDERS AND DISEASES HandoutsMARIALUPE ESTOQUENo ratings yet
- Dermaplaning Information SheetDocument2 pagesDermaplaning Information SheetEvelyn MurilloNo ratings yet
- Customer Service ProtocolDocument8 pagesCustomer Service ProtocolLaura Beltrán CéspedesNo ratings yet
- Chapter 23 OutlineDocument55 pagesChapter 23 OutlinerobertNo ratings yet
- Main - Microblading Consent FormDocument2 pagesMain - Microblading Consent FormAnnee bellaNo ratings yet
- The Spa Book: The Official Guide To Spa Therapy - Fashion & Beauty IndustriesDocument4 pagesThe Spa Book: The Official Guide To Spa Therapy - Fashion & Beauty IndustrieskyxesegaNo ratings yet
- DermaRoller Consent Form 2011Document3 pagesDermaRoller Consent Form 2011BrianZackNo ratings yet
- Master EstheticianDocument2 pagesMaster Estheticianapi-791991640% (2)
- Skinside Out: Beauty Ethnicity & Cosmetic SurgeryFrom EverandSkinside Out: Beauty Ethnicity & Cosmetic SurgeryNo ratings yet
- Essay 20 Tips To Improve Service SkillsDocument8 pagesEssay 20 Tips To Improve Service Skillsdobe.h15No ratings yet
- CIDESCO CertificationDocument1 pageCIDESCO CertificationSandip PatilNo ratings yet
- Spa Treatment MenuDocument32 pagesSpa Treatment MenuEmelia Jugdav100% (1)
- Beauty Checklist PrintableDocument1 pageBeauty Checklist PrintableSandyDavidNo ratings yet
- The Basics of Skincare: A Framework For Study ReflectionDocument28 pagesThe Basics of Skincare: A Framework For Study Reflectiondgina8800No ratings yet
- Guide: Facial RejuvenationDocument12 pagesGuide: Facial Rejuvenationcesar augusto palacio echeverriNo ratings yet
- Training Book MederDocument35 pagesTraining Book MederToàn Nguyễn ĐứcNo ratings yet
- 1620215237wpdm - MMM Training ManualDocument10 pages1620215237wpdm - MMM Training Manualndg_49No ratings yet
- The Spa V BioessenceDocument18 pagesThe Spa V BioessencePatrick HariramaniNo ratings yet
- Micro Blading Training BibleDocument98 pagesMicro Blading Training Biblezaina28No ratings yet
- NVQ SVQ Diploma in Beauty Therapy Level 3 Sample Unit G8 Draft Sample MaterialDocument6 pagesNVQ SVQ Diploma in Beauty Therapy Level 3 Sample Unit G8 Draft Sample MaterialJowie SooNo ratings yet
- DermalogicaDocument28 pagesDermalogicaSundas ShahidNo ratings yet
- Eventsec Customer Care TrainingDocument12 pagesEventsec Customer Care Traininginfo856No ratings yet
- MONU Manual Section 4Document45 pagesMONU Manual Section 4amymonuskinNo ratings yet
- Confidential Consultation Form: Personal InformationDocument3 pagesConfidential Consultation Form: Personal InformationPurwandoko SutopoNo ratings yet
- Client Intake Form - NailsDocument2 pagesClient Intake Form - NailsGGenZ ConsultingNo ratings yet
- Beauty Therapy PracticalDocument60 pagesBeauty Therapy Practicalangela100% (1)
- Consent WaxingDocument1 pageConsent Waxingapi-252185122No ratings yet
- Skin Training 2Document81 pagesSkin Training 2TheQueensafa90100% (2)
- Basic Model User'S ManualDocument4 pagesBasic Model User'S ManualDokterYolanda100% (1)
- Presentation 2 Final 1Document20 pagesPresentation 2 Final 1api-463666283No ratings yet
- Microdermabrasion Manual SFMCDocument13 pagesMicrodermabrasion Manual SFMCji76100% (1)
- New Client Intake FormDocument1 pageNew Client Intake FormTori BaileyNo ratings yet
- Sect 8 - Ref GalvadermDocument19 pagesSect 8 - Ref GalvadermamymonuskinNo ratings yet
- Daily Skin Care PDFDocument2 pagesDaily Skin Care PDFiqra zafarNo ratings yet
- Basic Skin Care ProtocolsDocument16 pagesBasic Skin Care ProtocolsCarmi Bolivar CodotcoNo ratings yet
- Beauty Has Its Own Rules: Everything There Is to Know on the New World of Beauty TreatmentsFrom EverandBeauty Has Its Own Rules: Everything There Is to Know on the New World of Beauty TreatmentsNo ratings yet
- Make Acne Stop: The Easiest Guide to Treatments for Acne & Acne ScarsFrom EverandMake Acne Stop: The Easiest Guide to Treatments for Acne & Acne ScarsNo ratings yet
- Doha Form 842Document34 pagesDoha Form 842Gaia Wellness CompanyNo ratings yet
- St. Faustina's Litany To The Blessed Host: (Diary of Saint Maria Faustina Kowalska, Paragraph 356)Document2 pagesSt. Faustina's Litany To The Blessed Host: (Diary of Saint Maria Faustina Kowalska, Paragraph 356)Gaia Wellness CompanyNo ratings yet
- 50 Ways To Get Online Tutoring Students 2021 1Document16 pages50 Ways To Get Online Tutoring Students 2021 1Gaia Wellness CompanyNo ratings yet
- Rose Petal LemonadeDocument1 pageRose Petal LemonadeGaia Wellness CompanyNo ratings yet
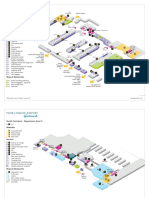
- Gatwick South v282 PDFDocument6 pagesGatwick South v282 PDFAuxiliadora Poyato RamirezNo ratings yet
- Way of The Cross For LegionariesDocument4 pagesWay of The Cross For LegionariesclosoriosaldoNo ratings yet
- CSP General Information Booklet - ECWA Sponsored Global Humanitarian Visa - 18 AUGUST 2022Document17 pagesCSP General Information Booklet - ECWA Sponsored Global Humanitarian Visa - 18 AUGUST 2022Gaia Wellness CompanyNo ratings yet
- 30 - Second After Elevator Speech PuciataDocument3 pages30 - Second After Elevator Speech PuciataGaia Wellness CompanyNo ratings yet
- 10 Clients In30 Days CTDActionGuideDocument3 pages10 Clients In30 Days CTDActionGuideGaia Wellness CompanyNo ratings yet
- 6 Steps To Attracting Your Ideal ClientDocument12 pages6 Steps To Attracting Your Ideal ClientGaia Wellness CompanyNo ratings yet
- Questions For Business Strategy SessionDocument3 pagesQuestions For Business Strategy SessionGaia Wellness CompanyNo ratings yet
- Impact Slave TradeDocument1 pageImpact Slave TradeGaia Wellness CompanyNo ratings yet
- 071114blog ChecklistDocument1 page071114blog ChecklistGaia Wellness CompanyNo ratings yet
- Your Rock Solid Business Plan Template 2016Document24 pagesYour Rock Solid Business Plan Template 2016Gaia Wellness CompanyNo ratings yet
- TA Cheat SheetDocument1 pageTA Cheat SheetGaia Wellness CompanyNo ratings yet
- Annual Return Form28Document5 pagesAnnual Return Form28Gaia Wellness CompanyNo ratings yet
- RGD Receipt 115823592203Document1 pageRGD Receipt 115823592203Gaia Wellness CompanyNo ratings yet
- Ab Rehab Guide 2019Document19 pagesAb Rehab Guide 2019Gaia Wellness CompanyNo ratings yet
- AlphabetDocument2 pagesAlphabetGaia Wellness CompanyNo ratings yet
- GrammarDocument2 pagesGrammarGaia Wellness CompanyNo ratings yet
- Muscular SystemDocument3 pagesMuscular SystemGaia Wellness CompanyNo ratings yet
- Human Skeletal SystemDocument1 pageHuman Skeletal SystemGaia Wellness CompanyNo ratings yet
- OSHA Employment Application Form (2) 2 - Copy - CompletedDocument3 pagesOSHA Employment Application Form (2) 2 - Copy - CompletedGaia Wellness CompanyNo ratings yet
- Blocks Centre LTD C20150428066: Form 28Document5 pagesBlocks Centre LTD C20150428066: Form 28Gaia Wellness CompanyNo ratings yet
- The Ultimate DR Recovery Guide 2Document12 pagesThe Ultimate DR Recovery Guide 2Gaia Wellness Company0% (1)
- Math Video Lessons For Remote Teaching EdpuzzleDocument4 pagesMath Video Lessons For Remote Teaching EdpuzzleGaia Wellness CompanyNo ratings yet
- Letter of Complaint ELADocument1 pageLetter of Complaint ELAGaia Wellness CompanyNo ratings yet
- Detox Acne Facial: Step 1: Step 2: Step 3: Step 4: Step 5Document1 pageDetox Acne Facial: Step 1: Step 2: Step 3: Step 4: Step 5Gaia Wellness CompanyNo ratings yet
- Chocolate Chip Banana Bread in A JarDocument1 pageChocolate Chip Banana Bread in A JarGaia Wellness CompanyNo ratings yet
- FNMGiftTag WEBDocument1 pageFNMGiftTag WEBGaia Wellness CompanyNo ratings yet
- Total Abdominal Hysterectomy With Bilateral SalpingoDocument3 pagesTotal Abdominal Hysterectomy With Bilateral SalpingoReyniel Pablo ElumbaNo ratings yet
- Powerful Communication Tools For Successful Acupuncture PracticeDocument4 pagesPowerful Communication Tools For Successful Acupuncture Practicebinglei chenNo ratings yet
- Chronic Rhinosinusitis With Nasal Polyps: Clinical PracticeDocument9 pagesChronic Rhinosinusitis With Nasal Polyps: Clinical PracticeAnabel SagasteguiNo ratings yet
- Anti Allergy: NO Produk Komposisi Kemasan HNA Hna + PPN KETDocument6 pagesAnti Allergy: NO Produk Komposisi Kemasan HNA Hna + PPN KETMuhammad Asri,S.Kep,NsNo ratings yet
- Aceclofenac 100 MG Film-Coated Tablets - Summary of Product Characteristics (SMPC) - Print Friendly - (eMC) PDFDocument9 pagesAceclofenac 100 MG Film-Coated Tablets - Summary of Product Characteristics (SMPC) - Print Friendly - (eMC) PDFHabibNo ratings yet
- Giant Malignant Phyllodes Tumor of The Breast: A Case Report Etuk EB', Amanari OC', Nwafor CC 2Document5 pagesGiant Malignant Phyllodes Tumor of The Breast: A Case Report Etuk EB', Amanari OC', Nwafor CC 2siti qomaria usuNo ratings yet
- AACN-Essentials of Critical Care Nursing - 1st EditionDocument602 pagesAACN-Essentials of Critical Care Nursing - 1st Editiondevils27100% (1)
- Nursing Diagnosis in Acne VulgarisDocument1 pageNursing Diagnosis in Acne VulgarisEvangelyn EgusquizaNo ratings yet
- Arbeitsheft 2018Document147 pagesArbeitsheft 2018Pamela MusabelliuNo ratings yet
- Infopia Clover A1cDocument31 pagesInfopia Clover A1cAde NasutionNo ratings yet
- Industrial Pharmacy Practice Notes-1Document4 pagesIndustrial Pharmacy Practice Notes-1Gerald Limo Arap ChebiiNo ratings yet
- CHO Special MCQs #1Document7 pagesCHO Special MCQs #1Praveen LaxkarNo ratings yet
- Alternative Certificate - Foundation Competences ProtectedDocument12 pagesAlternative Certificate - Foundation Competences ProtectedFlavian Costin NacladNo ratings yet
- Lplpo Agustus 2017Document66 pagesLplpo Agustus 2017Selly Wijaya BermawiNo ratings yet
- Interventions For Clients Requiring Oxygen Therapy or TracheostomyDocument25 pagesInterventions For Clients Requiring Oxygen Therapy or TracheostomyFabricio Serna MarinNo ratings yet
- SCRIPTDocument5 pagesSCRIPTMia Grace GarciaNo ratings yet
- 2019-Cpc Study Guide Sample PagesDocument15 pages2019-Cpc Study Guide Sample PagesAneez Malik63% (8)
- Nauclea Latifolia: A Medicinal, Economic and Pharmacological ReviewDocument19 pagesNauclea Latifolia: A Medicinal, Economic and Pharmacological ReviewMichael Kwesi BaahNo ratings yet
- ARTG Summary For Health NavigatorDocument2 pagesARTG Summary For Health NavigatorinergetixNo ratings yet
- Rule 15Document2 pagesRule 15begenyolNo ratings yet
- Universiti Teknologi Mara Cawangan Pahang Faculty of Sports Science & RecreationDocument26 pagesUniversiti Teknologi Mara Cawangan Pahang Faculty of Sports Science & RecreationJalal NasirNo ratings yet
- Hyperemesis GravidarumDocument32 pagesHyperemesis GravidarumBharat ThapaNo ratings yet
- Noureen Zawar Family Medicine FMH Oct 21, 2017Document32 pagesNoureen Zawar Family Medicine FMH Oct 21, 2017Noureen ZawarNo ratings yet
- Validación EPDS en Chile - 1995Document6 pagesValidación EPDS en Chile - 1995pennylane_girlNo ratings yet
- Mya Harkness-Annotated Bibliography 1-12Document10 pagesMya Harkness-Annotated Bibliography 1-12api-403918901No ratings yet
- Computed Tomography Radiation Safety Issues in OntarioDocument71 pagesComputed Tomography Radiation Safety Issues in Ontariopebbles18950% (2)
- What Is DysarthriaDocument3 pagesWhat Is DysarthriaAsnan Azis Fatoni100% (1)
- ETS & CapillaryDocument6 pagesETS & CapillaryRoela Marie AlbaniaNo ratings yet
- Family Systems: Genograms and Ecomaps: Dr. Mergan Naidoo Principal Family PhysicianDocument42 pagesFamily Systems: Genograms and Ecomaps: Dr. Mergan Naidoo Principal Family PhysicianWendy LucasNo ratings yet
- SMP 3510 Heller Chapter34Document48 pagesSMP 3510 Heller Chapter34Ari DewiyantiNo ratings yet