You might also like
- Basic Arrhythmia RulesDocument3 pagesBasic Arrhythmia Rulesgreenflames0997% (30)
- STEMI Mimics A Mnemonic.Document13 pagesSTEMI Mimics A Mnemonic.Simon Mark Daley100% (1)
- ECG Interpretation UnismaDocument178 pagesECG Interpretation UnismadefinaNo ratings yet
- Coronary Artery DiseaseDocument30 pagesCoronary Artery Diseasesarguss14100% (1)
- Advanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineDocument88 pagesAdvanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineRoroNo ratings yet
- EGurukul Cardiology 2.0Document287 pagesEGurukul Cardiology 2.0Merin Emanuel KNo ratings yet
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- Ekg FastlaneDocument10 pagesEkg FastlaneAida UzunovicNo ratings yet
- The P WaveDocument13 pagesThe P Wave成失No ratings yet
- Electrical Axis: Fast & Easy Ecgs - A Self-Paced Learning ProgramDocument29 pagesElectrical Axis: Fast & Easy Ecgs - A Self-Paced Learning ProgramMihaela PrisacaruNo ratings yet
- Basics & Timing-PmDocument120 pagesBasics & Timing-PmWiwik Puji Lestari100% (1)
- Cardiac Stress TestingDocument24 pagesCardiac Stress TestingRhoda Dela Torre ContrerasNo ratings yet
- EKG/ECG Study GuideDocument13 pagesEKG/ECG Study GuideSherree HayesNo ratings yet
- Dysrhythmias: Sinus Node Dysrhythmias Tachycardia, and Sinus ArrhythmiaDocument5 pagesDysrhythmias: Sinus Node Dysrhythmias Tachycardia, and Sinus ArrhythmiaKayelyn-Rose Combate100% (1)
- Basic Arrythmias: Prof. Maximin A. Pomperada, RN, MNDocument70 pagesBasic Arrythmias: Prof. Maximin A. Pomperada, RN, MNRellie CastroNo ratings yet
- ECG Master Class-3Document97 pagesECG Master Class-3Shohag ID CenterNo ratings yet
- Approach To A Patient With Congenital Heart DiseaseDocument164 pagesApproach To A Patient With Congenital Heart DiseaseCloudySkyNo ratings yet
- Avnrt AvrtDocument21 pagesAvnrt AvrtRima Rovanne Wenas100% (1)
- Advanced 12-Lead InterpretationDocument30 pagesAdvanced 12-Lead InterpretationRohini SelvarajahNo ratings yet
- Hepatic Vein FlowDocument14 pagesHepatic Vein FlowJORGENo ratings yet
- Top Ten (Or 11) EKG KillersDocument84 pagesTop Ten (Or 11) EKG KillersphausknechtNo ratings yet
- Heart MuscleDocument10 pagesHeart Muscle22194No ratings yet
- Basic Chest X-Ray Interpretation: Eliana MuisDocument58 pagesBasic Chest X-Ray Interpretation: Eliana MuiselianaNo ratings yet
- Valvular Heart DiseaseDocument54 pagesValvular Heart DiseaseKiki RizkyNo ratings yet
- Normal Ecg, Infarction & Arrhythmia SDocument98 pagesNormal Ecg, Infarction & Arrhythmia SAdinda GupitaNo ratings yet
- ECG at A GlanceDocument53 pagesECG at A GlancePetrus TjiangNo ratings yet
- EDAN Holter System V1.2Document27 pagesEDAN Holter System V1.2Suciu FlorinNo ratings yet
- Ecg Treadmill and Holter TestDocument77 pagesEcg Treadmill and Holter TestRiteka Singh100% (1)
- Mitral Valve Prolapse, Flailed Mitral Valve Mitral Annular CalcificationDocument33 pagesMitral Valve Prolapse, Flailed Mitral Valve Mitral Annular CalcificationcafemedNo ratings yet
- Bundle Branch BlockDocument37 pagesBundle Branch BlocksyukronchalimNo ratings yet
- Echo Facts IndexDocument3 pagesEcho Facts Indexs336336anl100% (1)
- Chronic Congestive Heart Failure: Dr. Irwan, SPJPDocument115 pagesChronic Congestive Heart Failure: Dr. Irwan, SPJPMuhammad Arief Budiman YSNo ratings yet
- Biatrial Enlargement DefinitionDocument3 pagesBiatrial Enlargement DefinitionFathimah afifah zahrah100% (1)
- Dr. Firman Leksmono SP - JP Basic ECG Interpretation For StudentDocument54 pagesDr. Firman Leksmono SP - JP Basic ECG Interpretation For Studentadela_97line100% (2)
- 123 Sonography Prosthetic Valves AssesmentDocument9 pages123 Sonography Prosthetic Valves AssesmentNavojit Chowdhury100% (1)
- Pacing Week PresentationsDocument54 pagesPacing Week PresentationsjoejenningsNo ratings yet
- Essential Cardiac Electrophysiology: The Self-Assessment ApproachFrom EverandEssential Cardiac Electrophysiology: The Self-Assessment ApproachNo ratings yet
- Learning Ecg ModulesDocument150 pagesLearning Ecg ModulesdodiNo ratings yet
- Mitral RegurgitationDocument6 pagesMitral RegurgitationMelfi Triani SiskaNo ratings yet
- Focal Atrial Tachycardia I: Clinical Features, DiagnosisDocument10 pagesFocal Atrial Tachycardia I: Clinical Features, Diagnosisapi-26166949No ratings yet
- Mitral RegurgitationDocument11 pagesMitral RegurgitationAbdur RaqibNo ratings yet
- Advanced ECG BBB PGDocument47 pagesAdvanced ECG BBB PGdragon66No ratings yet
- Ecg Pathology 02Document95 pagesEcg Pathology 02Andi MP Manurung100% (1)
- Pulmonary HypertensionDocument58 pagesPulmonary HypertensionnadiasalimaNo ratings yet
- Chest X-RayDocument101 pagesChest X-RayYuke04No ratings yet
- 08 - Abnormalities of R Wave ProgressionDocument3 pages08 - Abnormalities of R Wave ProgressionSharan Murugaboopathy100% (1)
- Basics of Pacing CombinedDocument54 pagesBasics of Pacing CombinedMichael Susanto100% (1)
- Basic Ecg: A Report By: Clinical Clerk Mary Hazel TeDocument74 pagesBasic Ecg: A Report By: Clinical Clerk Mary Hazel TeHazel Arcosa100% (1)
- ElectrocardiogramDocument52 pagesElectrocardiogramTuong HoangManhNo ratings yet
- DORVDocument33 pagesDORVjayasiinputNo ratings yet
- Atrial Septal DefekDocument29 pagesAtrial Septal DefekChe Ainil ZainodinNo ratings yet
- L-R ShuntDocument88 pagesL-R ShuntnanohaniwiekoNo ratings yet
- Basic EP IntervalsDocument13 pagesBasic EP IntervalsdrharoonmohdNo ratings yet
- Left Ventricular Non-CompactionDocument20 pagesLeft Ventricular Non-CompactionlawlietNo ratings yet
- Cardiac SarcoidosisDocument13 pagesCardiac SarcoidosisEmeric Jorge Macedo VendezuNo ratings yet
- Mechanisms of Cardiac Arrhythmias From Automatici+Document24 pagesMechanisms of Cardiac Arrhythmias From Automatici+Malar MannanNo ratings yet
- Valvular Heart Disease 2Document46 pagesValvular Heart Disease 2Topea BogdanNo ratings yet
- AP WindowDocument13 pagesAP WindowHugo GonzálezNo ratings yet
- Pericardial EffusionDocument3 pagesPericardial EffusionNita Hurek100% (1)
- Cardiac Cycle: Mechanical Event and Their Electrical and Clinical CorrelationDocument28 pagesCardiac Cycle: Mechanical Event and Their Electrical and Clinical Correlationhawas muhammed100% (1)
- FinalDocument56 pagesFinalvamshidhNo ratings yet
- Cardio-Vascular Disease: Mitral Stenosis & Mitral RegurgitationDocument25 pagesCardio-Vascular Disease: Mitral Stenosis & Mitral Regurgitationyulia silviNo ratings yet
- Dr. Dheeraj Sharma M.CH ResidentDocument94 pagesDr. Dheeraj Sharma M.CH ResidentVik SharNo ratings yet
- Eisenmenger SyndromeDocument6 pagesEisenmenger SyndromeWarkah SanjayaNo ratings yet
- Design and Analysis of A Dual Chamber Cardiac Pacemaker Using VHDL in Biomedical ApplicationDocument3 pagesDesign and Analysis of A Dual Chamber Cardiac Pacemaker Using VHDL in Biomedical ApplicationEditor IJRITCCNo ratings yet
- Mitral StenosisDocument50 pagesMitral Stenosissruthimeena6891No ratings yet
- STEMI RBBB TypeDocument6 pagesSTEMI RBBB TypeAlfa AlfinNo ratings yet
- CARDIAC ELECTROPHYSIOLOGY AND THE ELECTROCARDIOGRAM - ClinicalKey PDFDocument40 pagesCARDIAC ELECTROPHYSIOLOGY AND THE ELECTROCARDIOGRAM - ClinicalKey PDFMelanie DascăluNo ratings yet
- ECG Case 084: ECG 1 On Arrival Pain 3/10Document2 pagesECG Case 084: ECG 1 On Arrival Pain 3/10Fathimah afifah zahrahNo ratings yet
- ECG Case 094Document3 pagesECG Case 094Fathimah afifah zahrahNo ratings yet
- Left Posterior Fascicular BlockDocument4 pagesLeft Posterior Fascicular BlockFathimah afifah zahrahNo ratings yet
- Left Anterior Fascicular BlockDocument4 pagesLeft Anterior Fascicular BlockFathimah afifah zahrahNo ratings yet
- Definition of Trifascicular BlockDocument4 pagesDefinition of Trifascicular BlockFathimah afifah zahrahNo ratings yet
- Sgarbossa Criteria OverviewDocument4 pagesSgarbossa Criteria OverviewFathimah afifah zahrahNo ratings yet
- Onlinemeded Notes CardioDocument1 pageOnlinemeded Notes CardioCourtney HolbrookNo ratings yet
- Ischemic Heart DiseaseDocument13 pagesIschemic Heart Diseasegyspsunshine girlNo ratings yet
- Diastolic DysfunctionDocument5 pagesDiastolic DysfunctionNeeraja AjayanNo ratings yet
- Acls Notes 7-2012Document13 pagesAcls Notes 7-2012sarahbearcoupsNo ratings yet
- Cal EcgDocument7 pagesCal EcgNur Amirah FarhanahNo ratings yet
- IGH (Indian Guidelines On Hypertension) - 2019 GUIDELINESDocument15 pagesIGH (Indian Guidelines On Hypertension) - 2019 GUIDELINESVasishta NadellaNo ratings yet
- AP Biology Lab Ten: Physiology of The Circulatory SystemDocument8 pagesAP Biology Lab Ten: Physiology of The Circulatory SystemCoolAsianDude75% (4)
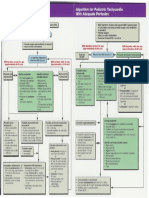
- Pediatric Tachycardia AlgorithmsDocument1 pagePediatric Tachycardia AlgorithmsGalih FatoniNo ratings yet
- Mitral Regurgitation Congestive: CardiomyopathyDocument4 pagesMitral Regurgitation Congestive: CardiomyopathyHamna NaeemNo ratings yet
- 1.HT MechanismDocument40 pages1.HT MechanismChayagon MongkonsawatNo ratings yet
- Nur 111 Session 10 Sas 1Document9 pagesNur 111 Session 10 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- AcQtrac BrochureDocument8 pagesAcQtrac Brochurex409No ratings yet
- NCM 112 Pre Test On EcgDocument2 pagesNCM 112 Pre Test On EcgTrixia AlmendralNo ratings yet
- Sphygmomanometers For Clinical UseDocument19 pagesSphygmomanometers For Clinical Usever_at_workNo ratings yet
- How Animals Survive (Circulation and GasDocument24 pagesHow Animals Survive (Circulation and GasJohn Ted BañezNo ratings yet
- Bprints MEDICINE Best Copy SearchableDocument90 pagesBprints MEDICINE Best Copy SearchablePhilippe Ceasar BascoNo ratings yet
- Pathophysiology: Cardiovascular System Dr. Maen DweikDocument38 pagesPathophysiology: Cardiovascular System Dr. Maen DweikshoibyNo ratings yet
- Advanced Cardiac Life SupportDocument13 pagesAdvanced Cardiac Life SupportEldonVinceIsidroNo ratings yet
- Daftar Pustaka: Medical Students and Faculty - Edisi Keempat - Baltimore-PhiladelpiaDocument2 pagesDaftar Pustaka: Medical Students and Faculty - Edisi Keempat - Baltimore-PhiladelpiaSylvia PertiwiNo ratings yet
- LIT177 Impulse6000 D - 7000DP Demo Instructions - RevbDocument11 pagesLIT177 Impulse6000 D - 7000DP Demo Instructions - RevbAlejandra EchavarriaNo ratings yet
- ID Efektivitas Senam Jantung Sehat TerhadapDocument7 pagesID Efektivitas Senam Jantung Sehat TerhadapAisyah SyahidahNo ratings yet
- Data Set 1: Health Exam Results: Male Age HT WT Waist Pulse SYS Dias Chol BMI Leg Elbow Wrist ArmDocument2 pagesData Set 1: Health Exam Results: Male Age HT WT Waist Pulse SYS Dias Chol BMI Leg Elbow Wrist ArmBishop PantaNo ratings yet