You might also like
- Bank DepositsDocument15 pagesBank DepositsSamuel BaulaNo ratings yet
- VDA Volume 2 6.edition (2020 04) enDocument92 pagesVDA Volume 2 6.edition (2020 04) enGreenheart Oussama100% (6)
- Geometric Shape GeneratorDocument23 pagesGeometric Shape GeneratorAhmedYahiaEnabNo ratings yet
- BVG Integrated Services BroucherDocument8 pagesBVG Integrated Services Broucherankit sharmaNo ratings yet
- Republic Vs Li YaoDocument2 pagesRepublic Vs Li YaoKariz Escaño100% (1)
- Test - Palo Alto Networks Accredited Systems Engineer (PSE) : Cortex Associate Accreditation ExamDocument8 pagesTest - Palo Alto Networks Accredited Systems Engineer (PSE) : Cortex Associate Accreditation Examandresp_telecom0% (1)
- Rekapan Rujukan PKM Soreang 2022Document97 pagesRekapan Rujukan PKM Soreang 2022Fitri KarsariNo ratings yet
- Diare 11Document1 pageDiare 11Nirmala SariNo ratings yet
- Laporan Posyandu 2017 LamaDocument18 pagesLaporan Posyandu 2017 LamaGugus MatahariNo ratings yet
- Sop Air WayDocument9 pagesSop Air WayAyhu HadriNo ratings yet
- SheetDocument1 pageSheetPankati SutharNo ratings yet
- Ground. (On Site) ModelDocument1 pageGround. (On Site) ModelFathima NazrinNo ratings yet
- Room Attendant Control SheetDocument3 pagesRoom Attendant Control SheetStev WualaNo ratings yet
- Full Trail Map - WebDocument1 pageFull Trail Map - WebEdan AmoyalNo ratings yet
- 6J Puteri NorzilaDocument2 pages6J Puteri NorzilakerenggaNo ratings yet
- Leiger 2021 Pas Kelas 9 ADocument4 pagesLeiger 2021 Pas Kelas 9 AIlham AkbarNo ratings yet
- TPP Juni PKM BlanakanDocument1 pageTPP Juni PKM BlanakanRifan HaykalNo ratings yet
- 2018-2019 SEASONAL PLAN Below 11 Years Old Football Team SK Kampung Baharu, JerantutDocument5 pages2018-2019 SEASONAL PLAN Below 11 Years Old Football Team SK Kampung Baharu, JerantutCik MeijayumiNo ratings yet
- Evidence Perfundimtare, KL.3 B Lirika ToskaDocument1 pageEvidence Perfundimtare, KL.3 B Lirika Toskajoana kiciNo ratings yet
- Luces Exteriores 1 de 2Document2 pagesLuces Exteriores 1 de 2Felix VelasquezNo ratings yet
- Layout Lampu Dan All Fix 2023Document13 pagesLayout Lampu Dan All Fix 2023All In OneNo ratings yet
- Movimiento de Almacen Enero 2024Document2 pagesMovimiento de Almacen Enero 2024Heberth quispe roaNo ratings yet
- Laporan Harian Obat Pustu LibukangDocument12 pagesLaporan Harian Obat Pustu Libukangwulan sriwardaniNo ratings yet
- Hegesztéstechnikai Utasítások Welding Instructions: 2DEA149 - Rev - 02Document1 pageHegesztéstechnikai Utasítások Welding Instructions: 2DEA149 - Rev - 02BanditAkosNo ratings yet
- 4u Asnida BT AbdullahDocument3 pages4u Asnida BT AbdullahkerenggaNo ratings yet
- City Engineer: City of Santa RosaDocument1 pageCity Engineer: City of Santa RosaDhenil ManubatNo ratings yet
- Diagram Alir Proses Pengolahan Gula Pabrik Gula Cinta Manis: Cane LifterDocument1 pageDiagram Alir Proses Pengolahan Gula Pabrik Gula Cinta Manis: Cane LifterTika Septia100% (1)
- HSHS DWG 001Document1 pageHSHS DWG 001Raymundo GirayNo ratings yet
- HNHS Entrance - Exit Gate - PlanDocument4 pagesHNHS Entrance - Exit Gate - PlanRaymundo GirayNo ratings yet
- UK First News 14 20 Jan 2022Document28 pagesUK First News 14 20 Jan 2022JIAJIE WUNo ratings yet
- WSNLBGKKUDCH7500080000V10APPROVEP47Document1 pageWSNLBGKKUDCH7500080000V10APPROVEP47rushi123No ratings yet
- 2u Pn. Maleesa Bt. Abdul WahidDocument3 pages2u Pn. Maleesa Bt. Abdul WahidkerenggaNo ratings yet
- 1-Exc Programme 2022 HOTELS Issued 08 MARCH 22Document1 page1-Exc Programme 2022 HOTELS Issued 08 MARCH 22apostomichNo ratings yet
- Girls Education MindmapDocument1 pageGirls Education MindmapYogesh ChaudhariNo ratings yet
- DNS - AYU ZULHAIDA, S.PD (XII IPS - Smstr-2 - 2016-2017)Document8 pagesDNS - AYU ZULHAIDA, S.PD (XII IPS - Smstr-2 - 2016-2017)sunarNo ratings yet
- Proposed Land Use-2032Document1 pageProposed Land Use-2032puneetNo ratings yet
- Downtown Des Moines Skywalk MapDocument1 pageDowntown Des Moines Skywalk MapannaNo ratings yet
- Pemerintah Kabupaten Gowa Dinas Kesehatan: Jumlah Desa: 14 Jumlah Lapor: MingguDocument2 pagesPemerintah Kabupaten Gowa Dinas Kesehatan: Jumlah Desa: 14 Jumlah Lapor: MingguRiezka AndrianaNo ratings yet
- Senarai Barang TKR Siri 181Document24 pagesSenarai Barang TKR Siri 181Azwar AshrafNo ratings yet
- Exhibition Slide A0Document1 pageExhibition Slide A0Gibran PradoNo ratings yet
- Vicinity Map: Mangaldan Public MarketDocument1 pageVicinity Map: Mangaldan Public Marketcristian gonzalesNo ratings yet
- The Sun Daily Final Edition 22-11-2019 CompleteDocument24 pagesThe Sun Daily Final Edition 22-11-2019 CompleteSitiNo ratings yet
- SD Percobaan 3 - 1Document6 pagesSD Percobaan 3 - 1Reza BaharsyahNo ratings yet
- Interim Master Plan PanchkulaDocument1 pageInterim Master Plan PanchkulaSUNIDHI VERMA100% (1)
- Bus TerminalDocument1 pageBus TerminalClarisse DoriaNo ratings yet
- This Site: Table of ContentDocument1 pageThis Site: Table of ContentReden H. ArgawanonNo ratings yet
- Proposed Installation of Dust Collector and Bending Machine 2019Document20 pagesProposed Installation of Dust Collector and Bending Machine 2019Mark Redira ManayonNo ratings yet
- Arnav - IDFC - TW Recovery Print FileDocument7 pagesArnav - IDFC - TW Recovery Print FileJitendra KumarNo ratings yet
- Indian Weekender 5 May 2017Document32 pagesIndian Weekender 5 May 2017Indian WeekenderNo ratings yet
- Wwett2019-8 Page FlyerDocument8 pagesWwett2019-8 Page Flyermarcus harnessNo ratings yet
- N Site Development Plan: 8M Road Right-Of-WayDocument1 pageN Site Development Plan: 8M Road Right-Of-WayParengpaching ggNo ratings yet
- Luces Exteriores 2 de 2Document2 pagesLuces Exteriores 2 de 2Felix VelasquezNo ratings yet
- Sale Is On Not For Long: Shop NOWDocument8 pagesSale Is On Not For Long: Shop NOWDEEPAK KUMAR SINGHNo ratings yet
- V03-B-MD-4 UnitsDocument23 pagesV03-B-MD-4 UnitsAmjad Wael Yahia FayedNo ratings yet
- MeerutDocument1 pageMeerutAbhishek ChetriNo ratings yet
- India Today 2016 05 02Document90 pagesIndia Today 2016 05 02Ayaz Ahmed KhanNo ratings yet
- Sekolah Tinggi Pariwisata Nusa Dua - Bali Room Boy/Maid Controll SheetsDocument3 pagesSekolah Tinggi Pariwisata Nusa Dua - Bali Room Boy/Maid Controll SheetsIputu PandeNo ratings yet
- Marca, Model / Judete: Alfa RomeoDocument38 pagesMarca, Model / Judete: Alfa Romeoalbinutza79No ratings yet
- Ea 3Document1 pageEa 3cloydNo ratings yet
- 4 Urban Renewal (PHYSICAL) Land Use ZoningDocument1 page4 Urban Renewal (PHYSICAL) Land Use ZoningstrictlythiccNo ratings yet
- Executive Floor - p4Document1 pageExecutive Floor - p4Zeeshan Ul HassanNo ratings yet
- Layout Grounding Pt. Wilmar Nabati Indonesia - Padang: Tank FarmDocument1 pageLayout Grounding Pt. Wilmar Nabati Indonesia - Padang: Tank FarmYosafat VidoNo ratings yet
- Plan and L SectionDocument2 pagesPlan and L SectiondilipNo ratings yet
- Victorias City Plaza Update3Document1 pageVictorias City Plaza Update3Calvin Chavez IIINo ratings yet
- 3 Location Map: One-Storey Residential BuildingDocument1 page3 Location Map: One-Storey Residential BuildingRichie Juls BacalsoNo ratings yet
- 4B CervixDocument87 pages4B CervixrubenNo ratings yet
- 4D OvaryDocument108 pages4D OvaryrubenNo ratings yet
- 4C UterusDocument86 pages4C UterusrubenNo ratings yet
- 4F Borderline Ovarian TumourDocument92 pages4F Borderline Ovarian TumourrubenNo ratings yet
- JD - Membership Ambassador (1) - 4Document2 pagesJD - Membership Ambassador (1) - 4NAMRATA GUPTANo ratings yet
- CtpsDocument88 pagesCtpsSyafiqah NajibNo ratings yet
- Thông báo nộp thuế TNCNDocument3 pagesThông báo nộp thuế TNCNTrieu Thi RanhNo ratings yet
- What Are The Similarities and Differences of The Raspberry Pi Pico VariantsDocument8 pagesWhat Are The Similarities and Differences of The Raspberry Pi Pico VariantsjackNo ratings yet
- School Watching Checklist and Hazard MappingDocument2 pagesSchool Watching Checklist and Hazard MappingMark CatiponNo ratings yet
- Sintesis Elektrokimia Kompleks Cuii Basa A403e316Document5 pagesSintesis Elektrokimia Kompleks Cuii Basa A403e316YuanNo ratings yet
- Lost StarsDocument3 pagesLost StarsRodrigo Massayuki SadakaneNo ratings yet
- Ingeniador v. Vital Images Et. Al.Document11 pagesIngeniador v. Vital Images Et. Al.PriorSmartNo ratings yet
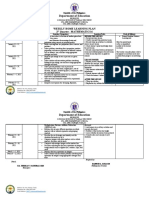
- Department of Education: Weekly Home Learning Plan 2 Quarter - MATHEMATICS 6Document2 pagesDepartment of Education: Weekly Home Learning Plan 2 Quarter - MATHEMATICS 6Maestro Varix100% (1)
- RedoxDocument29 pagesRedoxViníciusNo ratings yet
- ACI Anywhere Extending The ACI Fabric - Max ArdicaDocument53 pagesACI Anywhere Extending The ACI Fabric - Max ArdicavijiNo ratings yet
- Edith Wharton Roman Fever ThesisDocument5 pagesEdith Wharton Roman Fever Thesish0nuvad1sif2100% (1)
- Philtranco Services Enterprises Vs BLRDocument3 pagesPhiltranco Services Enterprises Vs BLRPatricia VillamilNo ratings yet
- Program MUTDocument3 pagesProgram MUTSrdjan VasilijevićNo ratings yet
- Renewable Energy Basics OneDocument46 pagesRenewable Energy Basics OneqiTNo ratings yet
- NET Core ServiceCollectionExtensionDocument2 pagesNET Core ServiceCollectionExtensioncarlosNo ratings yet
- 0004000000175E00Document9 pages0004000000175E00akun YugiNo ratings yet
- Agency Contract (Draft)Document15 pagesAgency Contract (Draft)rogov.alumparkNo ratings yet
- Internet Banking Adoption in India: Structural Equation Modeling ApproachDocument2 pagesInternet Banking Adoption in India: Structural Equation Modeling ApproachNursamsiWahyuApriantoNo ratings yet
- Disciples of Christ - How Much Do We Desire To Know Him?Document123 pagesDisciples of Christ - How Much Do We Desire To Know Him?Irene McGoughNo ratings yet
- Beverage Recipe: Non CoffeeDocument4 pagesBeverage Recipe: Non CoffeeAldi RinaldiNo ratings yet
- Does Loving A Group Mean Hating Its Rivals? Exploring The Relationship Between Ingroup Cohesion and Outgroup Hostility Among Soccer FansDocument20 pagesDoes Loving A Group Mean Hating Its Rivals? Exploring The Relationship Between Ingroup Cohesion and Outgroup Hostility Among Soccer FansRaihan Nurul HadiNo ratings yet
- Journal of Statistical Software: Reviewer: Tim Downie Beuth University of Applied Sciences BerlinDocument4 pagesJournal of Statistical Software: Reviewer: Tim Downie Beuth University of Applied Sciences BerlinInfinitum Gym StoreNo ratings yet