You might also like
- The Educational Foundation of Guidance in The PhilippinesDocument5 pagesThe Educational Foundation of Guidance in The PhilippinesSir Vince Vinas100% (1)
- ACTIVITY 1 The Stages of Development and Developmental TasksDocument3 pagesACTIVITY 1 The Stages of Development and Developmental TasksJaymar Magtibay100% (2)
- My Unique Picture AlbumDocument1 pageMy Unique Picture AlbumJaymar Magtibay0% (1)
- NSTP 1 CWTS 1 Module For Health Care and Drug Education First Semester AY 2021-2022Document40 pagesNSTP 1 CWTS 1 Module For Health Care and Drug Education First Semester AY 2021-2022Marialyn AnonuevoNo ratings yet
- Using Technology To Study Cellular and Molecular BiologyDocument138 pagesUsing Technology To Study Cellular and Molecular BiologybheeshmatNo ratings yet
- Sip ReflectionDocument3 pagesSip Reflectionapi-310301423No ratings yet
- Implementing the MISOSA FrameworkDocument58 pagesImplementing the MISOSA FrameworkSienna Comanda HumamoyNo ratings yet
- (DM-PHROD-2020-00324) Dissemination of The School Effectiveness ToolkitDocument1 page(DM-PHROD-2020-00324) Dissemination of The School Effectiveness ToolkitRemelyn CortesNo ratings yet
- Using Walkie Talkies to Encourage Shy Students' English SpeakingDocument21 pagesUsing Walkie Talkies to Encourage Shy Students' English SpeakingCorollaGTNo ratings yet
- Edifying The Numeracy Skills of The Grade Five Pupils ThroughDocument1 pageEdifying The Numeracy Skills of The Grade Five Pupils ThroughJeffrey Yumang100% (1)
- Homeroom Guidance Module 5Document15 pagesHomeroom Guidance Module 5Jervin GuevarraNo ratings yet
- SIP Reflection: School Improvement ProcessDocument3 pagesSIP Reflection: School Improvement Processmary graceNo ratings yet
- Department of Education: Region Iii Schools Division Office of BulacanDocument6 pagesDepartment of Education: Region Iii Schools Division Office of BulacanKim Patrick VictoriaNo ratings yet
- MATATAG Directions 2028Document14 pagesMATATAG Directions 2028Carl CorreosNo ratings yet
- CS Form No 212 Work Experience SheetDocument2 pagesCS Form No 212 Work Experience Sheetraff estrada100% (1)
- Karaoke Cum Reading As Intervention To The Effects of CovidDocument19 pagesKaraoke Cum Reading As Intervention To The Effects of Covidruben oagdanNo ratings yet
- The Instructional Competencies of The Aralin Panlipunan Teaching Force The FinalDocument26 pagesThe Instructional Competencies of The Aralin Panlipunan Teaching Force The FinalAquino Mangilala Udtog100% (1)
- Instructional Supervisory Practices of School Heads During The New Normal at Buenavista Districts I and II, Division of QuezonDocument17 pagesInstructional Supervisory Practices of School Heads During The New Normal at Buenavista Districts I and II, Division of QuezonPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Decs Order Deped MemoDocument5 pagesDecs Order Deped MemoLowell Jay PacureNo ratings yet
- Processes of Educational Planning.Document18 pagesProcesses of Educational Planning.MK Barrientos100% (1)
- Chapter 3 Basic Principles of Educational PlanningDocument1 pageChapter 3 Basic Principles of Educational PlanningChristopher Dela cruzNo ratings yet
- Parent Teacher Partnership and Academic Performance Maria Andrea B. Monakil Maed em As of August 13, 2022Document61 pagesParent Teacher Partnership and Academic Performance Maria Andrea B. Monakil Maed em As of August 13, 2022Maria Andrea MonakilNo ratings yet
- Republic of The Philippines D E Division of Camarines Sur Bula, Camarines SurDocument1 pageRepublic of The Philippines D E Division of Camarines Sur Bula, Camarines SurShielaR.NavalNo ratings yet
- Natinalism& Patritoism IntegrityDocument33 pagesNatinalism& Patritoism IntegrityJehan ChawlaNo ratings yet
- Delm 311 Online OutputDocument4 pagesDelm 311 Online OutputMark Francis Munar100% (1)
- PPST Modules LAC Activity ReportDocument2 pagesPPST Modules LAC Activity ReportDima JhamboyNo ratings yet
- Biolinks: A Localized and Contextualized Instructional MaterialDocument12 pagesBiolinks: A Localized and Contextualized Instructional MaterialHeizelMeaVenturaLapuz-SuguitanNo ratings yet
- RM 576 Call For Applications To Pilot ALS SHS Program WORD AutoRecoveredDocument8 pagesRM 576 Call For Applications To Pilot ALS SHS Program WORD AutoRecoveredMark Anthony GarciaNo ratings yet
- Sdo Bulacan Cse Action Plan 2023 2024Document4 pagesSdo Bulacan Cse Action Plan 2023 2024heraldantoni.resurreccion100% (2)
- Department of Education: Republic of The PhilippinesDocument5 pagesDepartment of Education: Republic of The PhilippinesCarmehlyn BalogbogNo ratings yet
- Ra 10157 & Ra 9155: InsightsDocument2 pagesRa 10157 & Ra 9155: Insightsroa yusonNo ratings yet
- Filipino Action Plan 2016 - 2017Document8 pagesFilipino Action Plan 2016 - 2017Mhaye CendanaNo ratings yet
- Gad Integrated Lesson Plan 5Document19 pagesGad Integrated Lesson Plan 5Laarni BrionesNo ratings yet
- Home Visit Form TemplateDocument1 pageHome Visit Form TemplateMonica Morales Maaño100% (1)
- School-Based Management Key Performance IndicatorsDocument8 pagesSchool-Based Management Key Performance IndicatorsJohn Dale EvangelioNo ratings yet
- Department of Education: Republic of The PhilippinesDocument2 pagesDepartment of Education: Republic of The PhilippinesSARAH FABIANNo ratings yet
- Lesson 1: Background, Rationale, and Development of Melcs: Module 2: Most Essential Learning Competencies (Melcs)Document5 pagesLesson 1: Background, Rationale, and Development of Melcs: Module 2: Most Essential Learning Competencies (Melcs)LenielynBisoNo ratings yet
- Action Plan for Teacher DevelopmentDocument2 pagesAction Plan for Teacher DevelopmentAngela RuleteNo ratings yet
- The Third MillenniumDocument8 pagesThe Third MillenniumVanderNo ratings yet
- PPST - RP - Module 6Document38 pagesPPST - RP - Module 6Leodejoy Ruiz TulangNo ratings yet
- Continuous Improvement RoleDocument2 pagesContinuous Improvement RoleYeshua Yesha100% (1)
- Child FriendlySchoolSystemontheSchoolPerformanceDocument20 pagesChild FriendlySchoolSystemontheSchoolPerformanceCristy Lyn Bialen TianchonNo ratings yet
- Modular Teaching PDFDocument3 pagesModular Teaching PDFKazumi GraceAnnNo ratings yet
- Sjdmes 2Document2 pagesSjdmes 2Fairy-Lou Mejia100% (2)
- GIYA Teachers Guides For Instructions Yielding Archetype Teachers Grades 11 12Document8 pagesGIYA Teachers Guides For Instructions Yielding Archetype Teachers Grades 11 12Josine Calijan100% (1)
- Applied Knowledge and PedagogyDocument31 pagesApplied Knowledge and PedagogyEvan Siano BautistaNo ratings yet
- Level of Awareness in Values Restoration Program Among Senior High School StudentsDocument2 pagesLevel of Awareness in Values Restoration Program Among Senior High School StudentsAquiline ReedNo ratings yet
- Promoting Time Consciousness and HonestyDocument2 pagesPromoting Time Consciousness and HonestyMarah CedilloNo ratings yet
- Kra 1 Kra 2 Kra 3 Kra 4 Kra 5Document9 pagesKra 1 Kra 2 Kra 3 Kra 4 Kra 5Genesis Anne GarcianoNo ratings yet
- SARDO Tracking Template-UnprotectedDocument27 pagesSARDO Tracking Template-UnprotectedJonas Reduta Cabacungan33% (3)
- Matrix of Activities (Teachers' Day)Document2 pagesMatrix of Activities (Teachers' Day)Christine ApoloNo ratings yet
- Evaluating Nonformal Education ProgramsDocument21 pagesEvaluating Nonformal Education ProgramsLee Jae An100% (1)
- Certification of No Pending Staffing Modification (Long Size)Document1 pageCertification of No Pending Staffing Modification (Long Size)Mers ZiiNo ratings yet
- "Multi-Year Guidelines On The Results-Based Performance Management System-Philippine Professional Standards For Teachers".Document12 pages"Multi-Year Guidelines On The Results-Based Performance Management System-Philippine Professional Standards For Teachers".Mary Grace RamosNo ratings yet
- Education System in Philippines and HongkongDocument24 pagesEducation System in Philippines and HongkongTeofian Amparo LuibNo ratings yet
- District Learning Delivery Modalities Course 2 (LDM2) For TeachersDocument21 pagesDistrict Learning Delivery Modalities Course 2 (LDM2) For TeachersAni Vie Macero80% (10)
- Elln Second Lac SessionDocument3 pagesElln Second Lac SessionMarites Espino MaonNo ratings yet
- KRA Objectives and Performance SummaryDocument4 pagesKRA Objectives and Performance Summaryjennelyn malaynoNo ratings yet
- DO No. 105 S. 2010Document2 pagesDO No. 105 S. 2010Darwin Abes50% (2)
- L1A2 - Development and Design of MELCsDocument5 pagesL1A2 - Development and Design of MELCsCharlyne Mari Flores100% (1)
- Philippines Education Reform Agenda 2006-2010Document14 pagesPhilippines Education Reform Agenda 2006-2010Sheila Divinagracia - EscobedoNo ratings yet
- Safe and Secure: Strategies for Improving School Security in the PhilippinesFrom EverandSafe and Secure: Strategies for Improving School Security in the PhilippinesNo ratings yet
- Resolution 2021 1363Document2 pagesResolution 2021 1363TheSummitExpress75% (8)
- DM090 Administration of Philippine Informal Reading Inventory (Phil-IRI) PretestDocument2 pagesDM090 Administration of Philippine Informal Reading Inventory (Phil-IRI) PretestJaymar MagtibayNo ratings yet
- Conduct of The Clustered Orientation of Teacher-Advisers On The Recommended Programs, Projects and Activities (PPAS) of The Student Government Under The New NormalDocument3 pagesConduct of The Clustered Orientation of Teacher-Advisers On The Recommended Programs, Projects and Activities (PPAS) of The Student Government Under The New NormalJaymar MagtibayNo ratings yet
- Addendum to Division Memorandum No. 60, s. 2022 Titled Seminar-Workshop on the Preparation of Reports on Guidance & Counseling, Homeroom Guidance, Career Guidance Program, Child Protection cum Mental Health & Psycho-SoDocument1 pageAddendum to Division Memorandum No. 60, s. 2022 Titled Seminar-Workshop on the Preparation of Reports on Guidance & Counseling, Homeroom Guidance, Career Guidance Program, Child Protection cum Mental Health & Psycho-SoJaymar MagtibayNo ratings yet
- SY 2020-2021 Office Performance Commitment and Review Form (OPCRF)Document11 pagesSY 2020-2021 Office Performance Commitment and Review Form (OPCRF)Jaymar MagtibayNo ratings yet
- List of Self-Learning Module Reviewers/Editors in English For Quarters 1 & 3 NO. Name PositionDocument4 pagesList of Self-Learning Module Reviewers/Editors in English For Quarters 1 & 3 NO. Name PositionJaymar MagtibayNo ratings yet
- Grade 11 - Cinnamon (ABM) MaleDocument1 pageGrade 11 - Cinnamon (ABM) MaleJaymar MagtibayNo ratings yet
- Eastern Mindoro College Child Development CourseDocument2 pagesEastern Mindoro College Child Development CourseJaymar MagtibayNo ratings yet
- Civil Service Form No. 48 Daily Time RecordDocument2 pagesCivil Service Form No. 48 Daily Time RecordJaymar MagtibayNo ratings yet
- Certificate of Recognition English OrMinDocument80 pagesCertificate of Recognition English OrMinJaymar MagtibayNo ratings yet
- School Level - Form 1.0 - Secondary - Formon National High SchoolDocument242 pagesSchool Level - Form 1.0 - Secondary - Formon National High SchoolJaymar MagtibayNo ratings yet
- Certification of CompletionDocument1 pageCertification of CompletionJaymar MagtibayNo ratings yet
- List of Self-Learning Module Reviewers/Editors in English For Quarters 1 & 3 NO. Name PositionDocument4 pagesList of Self-Learning Module Reviewers/Editors in English For Quarters 1 & 3 NO. Name PositionJaymar MagtibayNo ratings yet
- Ljbepartmtnt of Qfbucation: Deped Ord Er No., S. 2021Document12 pagesLjbepartmtnt of Qfbucation: Deped Ord Er No., S. 2021Mike ReyesNo ratings yet
- DepEd Revised Guidelines on Work Arrangements During COVID-19Document16 pagesDepEd Revised Guidelines on Work Arrangements During COVID-19Godofredo CualterosNo ratings yet
- Eastern Mindoro CollegeDocument8 pagesEastern Mindoro CollegeJaymar MagtibayNo ratings yet
- O C C (V) : Pening and Losing Eremonies IrtualDocument8 pagesO C C (V) : Pening and Losing Eremonies IrtualJaymar MagtibayNo ratings yet
- Grade 11 - Gmelina (HUMSS) MaleDocument2 pagesGrade 11 - Gmelina (HUMSS) MaleJaymar MagtibayNo ratings yet
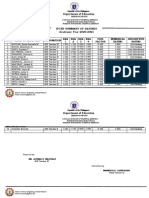
- Department of Education: Ipcrf Summary of Ratings Academic Year 2020-2021Document2 pagesDepartment of Education: Ipcrf Summary of Ratings Academic Year 2020-2021Jaymar MagtibayNo ratings yet
- Daily Time Record Daily Time Record Daily Time Record Daily Time RecordDocument2 pagesDaily Time Record Daily Time Record Daily Time Record Daily Time RecordJaymar MagtibayNo ratings yet
- Deped Smart Sim Card Activation TutorialDocument4 pagesDeped Smart Sim Card Activation TutorialJaymar MagtibayNo ratings yet
- Magtibay, ClaudiDocument1 pageMagtibay, ClaudiJaymar MagtibayNo ratings yet
- SY 2020-2021 Office Performance Commitment and Review Form (OPCRF)Document11 pagesSY 2020-2021 Office Performance Commitment and Review Form (OPCRF)Jaymar MagtibayNo ratings yet
- Grade 9-KAMAGONGDocument1 pageGrade 9-KAMAGONGJaymar MagtibayNo ratings yet
- Parents' Orientation - AttendanceDocument7 pagesParents' Orientation - AttendanceJaymar MagtibayNo ratings yet
- Magtibay, ClaudiDocument1 pageMagtibay, ClaudiJaymar MagtibayNo ratings yet
- SDO/School 2021 OBE Ticketing SystemDocument1 pageSDO/School 2021 OBE Ticketing SystemJaymar MagtibayNo ratings yet
- Assessing Pulse Oximetry (Performance Checklist) : Iloilo Doctors' College College of NursingDocument1 pageAssessing Pulse Oximetry (Performance Checklist) : Iloilo Doctors' College College of NursingJemy Tamaño MorongNo ratings yet
- Dissociative Disorder: Assistant Professor DR .Akeel Al Sabbagh Consultant PsychiatristDocument11 pagesDissociative Disorder: Assistant Professor DR .Akeel Al Sabbagh Consultant Psychiatristhani S. ALTaheryNo ratings yet
- Guidelines For COVID-19Document13 pagesGuidelines For COVID-19Pherdaus Islam AlaminNo ratings yet
- Šta je rezilijentnost definicijaDocument2 pagesŠta je rezilijentnost definicijaAlex Maric DragasNo ratings yet
- Tricho Till Omani ADocument25 pagesTricho Till Omani AYzel SeniningNo ratings yet
- Making The BussinessDocument4 pagesMaking The BussinessSonya RosaNo ratings yet
- Different Approaches in Pharmacological ResearchDocument3 pagesDifferent Approaches in Pharmacological ResearcharcherselevatorsNo ratings yet
- Learn The Basics Behind Basal Body TemperatureDocument6 pagesLearn The Basics Behind Basal Body TemperatureAaloka vermaNo ratings yet
- The Advantages and Disadvantages of Smart CitiesDocument3 pagesThe Advantages and Disadvantages of Smart CitiesthuantethiNo ratings yet
- Adhd InfographicDocument1 pageAdhd Infographicapi-666361680No ratings yet
- ErythroplakiaDocument20 pagesErythroplakiaEshan VermaNo ratings yet
- The Durex Story Stretching The MarketDocument4 pagesThe Durex Story Stretching The MarketShwetaGoudNo ratings yet
- MBBS-BDS Stray - Round - SelectionList R4Document462 pagesMBBS-BDS Stray - Round - SelectionList R4Lakshmi ManasaNo ratings yet
- AlzheimersDocument9 pagesAlzheimersNader Smadi100% (1)
- Health 7: Topic: Nutrition (Food Group and Elements of Nutrition) Grade 7Document42 pagesHealth 7: Topic: Nutrition (Food Group and Elements of Nutrition) Grade 7Zchecsh Blace AceNo ratings yet
- Workshop Report On International Brest Feeding Week Celebrations August 1 TO7 2021Document24 pagesWorkshop Report On International Brest Feeding Week Celebrations August 1 TO7 2021Apex College of NursingNo ratings yet
- By: Dr. Ayman Bukhari House Officer Obstetrics & GynaecologyDocument54 pagesBy: Dr. Ayman Bukhari House Officer Obstetrics & GynaecologyBharat ThapaNo ratings yet
- Article+0202 368 379Document12 pagesArticle+0202 368 379Muhammad Alif Nur FaizinNo ratings yet
- Giving Advice 2Document11 pagesGiving Advice 2Devi CintyaNo ratings yet
- Barret's Syndrome Case ReportDocument3 pagesBarret's Syndrome Case ReportResearch ParkNo ratings yet
- ASALEXU Volume 21 Issue 2 Pages 69-82Document14 pagesASALEXU Volume 21 Issue 2 Pages 69-82احمد العايديNo ratings yet
- Assignment-I Business Statistics: TOPIC: Abbott India LTDDocument14 pagesAssignment-I Business Statistics: TOPIC: Abbott India LTDAbhishek MohanpuriaNo ratings yet
- Forensic Aspects of Consultation-Liaison PsychiatryDocument88 pagesForensic Aspects of Consultation-Liaison PsychiatryRaul GrapilonNo ratings yet
- Vertigo DavidsonDocument13 pagesVertigo DavidsonifahInayahNo ratings yet
- Dakota Horizons BrochureDocument2 pagesDakota Horizons Brochurekatie_krebsbach_1No ratings yet
- MSOSH Academy Training Calendar 2020Document23 pagesMSOSH Academy Training Calendar 2020Muhammad FizreeNo ratings yet
- Respiratory System Upper Respiratory DiseasesDocument32 pagesRespiratory System Upper Respiratory DiseasesPrince Rener Velasco Pera100% (1)
- SPED-213-UNIT 1-Nature-of-Learning-Disability-CISDocument46 pagesSPED-213-UNIT 1-Nature-of-Learning-Disability-CISElaine Rae PugradNo ratings yet