You might also like
- NUR 204.administering A Tube FeedingDocument74 pagesNUR 204.administering A Tube FeedingKouta SanNo ratings yet
- Final Clinical Handout - Urinary Catheterization - 08.0602020Document4 pagesFinal Clinical Handout - Urinary Catheterization - 08.0602020Drmirfat AlkashifNo ratings yet
- - م 3 الانبوب الانفيDocument6 pages- م 3 الانبوب الانفيأسرار وغرائب owedahNo ratings yet
- التيوب الأنفي المعديDocument19 pagesالتيوب الأنفي المعديرافت العواضيNo ratings yet
- الأنبوب الأنفي المعدي We NursingDocument4 pagesالأنبوب الأنفي المعدي We Nursingرافت العواضيNo ratings yet
- 8تحضير المريض قبل وبعد العمليةDocument24 pages8تحضير المريض قبل وبعد العمليةnadakareem497No ratings yet
- Clinical Handout - Cast ApplicationDocument2 pagesClinical Handout - Cast ApplicationDrmirfat AlkashifNo ratings yet
- Pr.الإنعاش القلبي الرئوي .33Document2 pagesPr.الإنعاش القلبي الرئوي .33Ahmad Abu JmeiNo ratings yet
- Pre and Post Surgery Instruction A-3Document23 pagesPre and Post Surgery Instruction A-3Ola AfifyNo ratings yet
- العناية التمريضية قبل و بعد العمليةDocument12 pagesالعناية التمريضية قبل و بعد العمليةsafasayed100% (4)
- Contact Droplet Isolation Precautions ArabicDocument2 pagesContact Droplet Isolation Precautions ArabicShawqi AlmughniNo ratings yet
- Egd Preparations ArabicDocument2 pagesEgd Preparations Arabickurt94764No ratings yet
- 4 الاساليب المانعة للتلوثDocument6 pages4 الاساليب المانعة للتلوثnoha darwishNo ratings yet
- رقم 12 إزالة القسطرة البوليةDocument3 pagesرقم 12 إزالة القسطرة البوليةraad_alghamdi_1No ratings yet
- سحب الدم للمجموعاتDocument13 pagesسحب الدم للمجموعاتSanaa Sbdelghany100% (4)
- إن التمريض الجراحي قبل وبعد العمليات الجراحية يعتبر من أهم عوامل سرعة شفاء المريض فالسسترDocument5 pagesإن التمريض الجراحي قبل وبعد العمليات الجراحية يعتبر من أهم عوامل سرعة شفاء المريض فالسسترsafasayedNo ratings yet
- إعطاء الأدوية عن طريق الحقن-1Document2 pagesإعطاء الأدوية عن طريق الحقن-1mopeen٠٩٦٢١٠حخعقث١جملسمظزب . easaNo ratings yet
- الالتهاب الرئويDocument3 pagesالالتهاب الرئويlaoy aolNo ratings yet
- التنبيب الرغامي Intubation.pdf - 1Document31 pagesالتنبيب الرغامي Intubation.pdf - 1sultan mansoub100% (1)
- National Training Institute Ministry Of Health And Population بــيردــتـلل يــموـقـلا دـهـعمـلا ناـكسلاو ةــحصلا ةرازوDocument60 pagesNational Training Institute Ministry Of Health And Population بــيردــتـلل يــموـقـلا دـهـعمـلا ناـكسلاو ةــحصلا ةرازوMeme SooneNo ratings yet
- Pdfالعناية التمريضية للعمليات الجراحيةDocument6 pagesPdfالعناية التمريضية للعمليات الجراحيةRabab HassanNo ratings yet
- UntitledDocument233 pagesUntitledشَآدَي آلمِلگNo ratings yet
- رقم 60 كيفية استحمام المرضىDocument5 pagesرقم 60 كيفية استحمام المرضىraad_alghamdi_1No ratings yet
- نولوقلا ريظنتل ريضحتلا Colonoscopy PreparationsDocument2 pagesنولوقلا ريظنتل ريضحتلا Colonoscopy Preparationskurt94764No ratings yet
- 2 انعاش القلبي الرئويDocument45 pages2 انعاش القلبي الرئويaqel605859No ratings yet
- مصاب فاقد للوعي و لا يتنفسDocument16 pagesمصاب فاقد للوعي و لا يتنفسAbdellah ASKOURNo ratings yet
- Dr. Jamal Abdel Kareem Dabbas - Drdabbas - Com - Medical Publication Archive - Part1Document96 pagesDr. Jamal Abdel Kareem Dabbas - Drdabbas - Com - Medical Publication Archive - Part1Medicsindex Telepin SlidecaseNo ratings yet
- Clinical Handout - Ostomy Care (Option 1)Document2 pagesClinical Handout - Ostomy Care (Option 1)Drmirfat AlkashifNo ratings yet
- .. .. Bone marrow مترجمDocument4 pages.. .. Bone marrow مترجمreadsa722No ratings yet
- تحضير عينة البرازDocument37 pagesتحضير عينة البرازDjdjjd SiisusNo ratings yet
- الانعاش القلبي الرئويDocument16 pagesالانعاش القلبي الرئويMirna jamal100% (1)
- Pdfالعناية التمريضية للعمليات الجراحيةDocument6 pagesPdfالعناية التمريضية للعمليات الجراحيةDr NotesNo ratings yet
- ICUDocument47 pagesICUamna mahmood100% (1)
- Eemdcone4 Protocol IDocument3 pagesEemdcone4 Protocol ISal7 kra M7mdNo ratings yet
- Medical Assistant - FundamentalDocument74 pagesMedical Assistant - FundamentalAb90 S100% (1)
- العناية الذاتية بالفستولا والقسطرةDocument3 pagesالعناية الذاتية بالفستولا والقسطرةumibrahimNo ratings yet
- العناية بالتمريض لمرضى الجهاز البوليDocument13 pagesالعناية بالتمريض لمرضى الجهاز البوليlaoy aol100% (1)
- Omfs, Lecture 3 .Document5 pagesOmfs, Lecture 3 .0 0No ratings yet
- شرح المستلزماتDocument1 pageشرح المستلزماتSojod AliNo ratings yet
- مصاب فاقد للوعي و لا يتنفسDocument16 pagesمصاب فاقد للوعي و لا يتنفسAbdellah ASKOURNo ratings yet
- لوج نسا 2022Document40 pagesلوج نسا 2022Es LamNo ratings yet
- خزع الرغامى والتنبيبDocument38 pagesخزع الرغامى والتنبيبKlizli1996100% (1)
- Ctscan AraDocument4 pagesCtscan AraAhmed MardNo ratings yet
- كتاب اسس تمريض عملي 2016 - 1Document77 pagesكتاب اسس تمريض عملي 2016 - 1Abdullah Adel100% (2)
- Injections المحاقن الطبية PDFDocument12 pagesInjections المحاقن الطبية PDFDr NotesNo ratings yet
- سياسات عملية التسليم والتسلم بين طواقم التمريض في المستشفيDocument8 pagesسياسات عملية التسليم والتسلم بين طواقم التمريض في المستشفيmahmoud alghaberi92% (24)
- بحث انقاذ 1Document8 pagesبحث انقاذ 1dr.mohamed fathyNo ratings yet
- SCHS Nursing Specialist Exam Model 6Document9 pagesSCHS Nursing Specialist Exam Model 6Ahmad Khalil Al Sadi100% (1)
- UrineSampleFemale ARDocument3 pagesUrineSampleFemale ARFady FocasNo ratings yet
- 16 الإسعافات الأوليةDocument14 pages16 الإسعافات الأوليةAbdelrahman N. AliNo ratings yet
- تمريض مرضى الجهاز الهضميDocument9 pagesتمريض مرضى الجهاز الهضميlaoy aolNo ratings yet
- سلس البرازDocument10 pagesسلس البرازzsx4s9fts8No ratings yet
- رقم 28 الرعاية التمريضية لمريض الفصامDocument2 pagesرقم 28 الرعاية التمريضية لمريض الفصامraad_alghamdi_1No ratings yet
- GIS Data InterpretationDocument29 pagesGIS Data InterpretationZain MajaliNo ratings yet
- Natural Birth ArabicDocument11 pagesNatural Birth ArabicradbirdNo ratings yet
- Eaneanaev2 Protocol IDocument1 pageEaneanaev2 Protocol ISal7 kra M7mdNo ratings yet
- اعتني بمنطقة العجانDocument12 pagesاعتني بمنطقة العجانdauphinecenterkobNo ratings yet
- النظافة الشخصيةDocument18 pagesالنظافة الشخصيةRafic AbdallahNo ratings yet
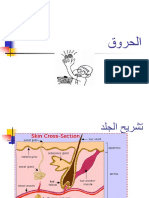
- Burn - ArabicDocument15 pagesBurn - ArabicmmmmmmNo ratings yet
- واجب المكبرDocument5 pagesواجب المكبرKouta SanNo ratings yet
- بحث عن خالد بن الوليد رضي الله عنهDocument16 pagesبحث عن خالد بن الوليد رضي الله عنهKouta SanNo ratings yet
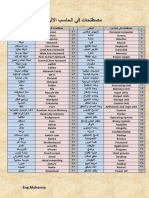
- مصطلحات في الحاسبDocument1 pageمصطلحات في الحاسبKouta SanNo ratings yet
- اسئلة مقدمة 6 شهور اجابهDocument3 pagesاسئلة مقدمة 6 شهور اجابهKouta SanNo ratings yet
- أساليب التطوير الذاتيDocument12 pagesأساليب التطوير الذاتيKouta San0% (1)
- بحث عن محمد صلى الله عليه وسلمDocument10 pagesبحث عن محمد صلى الله عليه وسلمKouta SanNo ratings yet