You might also like
- Black S Medical Dictionary PDFDocument2,413 pagesBlack S Medical Dictionary PDFAlexandr Trotsky100% (1)
- Why We Get SickDocument2 pagesWhy We Get SickJonathan RossNo ratings yet
- Utero-Placental Doppler Ultrasound For Improving Pregnancy Outcome (Review)Document50 pagesUtero-Placental Doppler Ultrasound For Improving Pregnancy Outcome (Review)Diapositivas08No ratings yet
- Placenta DevelopmentDocument74 pagesPlacenta DevelopmentEllagEsz33% (3)
- Figure 5-6: Virus Infected Body CellDocument10 pagesFigure 5-6: Virus Infected Body CellKaren Flores BartoloNo ratings yet
- Normal PregnancyDocument65 pagesNormal PregnancyRhesie Joyce AguilarNo ratings yet
- Garbhsanskar Mental and Intellectual Development of Unborn ChildDocument4 pagesGarbhsanskar Mental and Intellectual Development of Unborn ChildSabrina FagundesNo ratings yet
- Langman Medical Embryology Made Easy PDFDocument19 pagesLangman Medical Embryology Made Easy PDFAsma SaleemNo ratings yet
- 10 - Genetics and Evolution (Worksheet)Document8 pages10 - Genetics and Evolution (Worksheet)Lim YH100% (1)
- O&G CompendiumDocument676 pagesO&G Compendiumwalefamous100% (1)
- Case Presentation On IUD, Preeclampsia & Bells PalsyDocument14 pagesCase Presentation On IUD, Preeclampsia & Bells Palsypriyanjali sainiNo ratings yet
- Conduction of DeliveryDocument31 pagesConduction of Deliverysagi mu100% (2)
- HemtDocument42 pagesHemtSaily JaquezNo ratings yet
- FA 2022 Small SizeDocument42 pagesFA 2022 Small SizeAnNo ratings yet
- FA - Hematology and OncologyDocument40 pagesFA - Hematology and OncologyMargaret GraceNo ratings yet
- The Developing HumanDocument15 pagesThe Developing HumanJasmine Olinda DjuwonoNo ratings yet
- Sample Paper: Time: 90 Minutes Max. Marks: 50Document11 pagesSample Paper: Time: 90 Minutes Max. Marks: 50Swapnarani SubudhiNo ratings yet
- Coagulation Tests in Children PDFDocument47 pagesCoagulation Tests in Children PDFanggaririnNo ratings yet
- Paper - Biology10 - Semester 2 Exam - 2020Document14 pagesPaper - Biology10 - Semester 2 Exam - 2020Putri Dwi AnggrainiNo ratings yet
- BORJA Genetics Lab Exercise 6 Multiple Alleles and ABO Blood Groups in HumansDocument5 pagesBORJA Genetics Lab Exercise 6 Multiple Alleles and ABO Blood Groups in Humansbry uyNo ratings yet
- SMK Chung Cheng SPM Biology Trials (Paper 1)Document13 pagesSMK Chung Cheng SPM Biology Trials (Paper 1)mith777No ratings yet
- +2 Zoology WorksheetsDocument33 pages+2 Zoology WorksheetsLena AlbertNo ratings yet
- SQ03/N5/01 Biology Section 1-Questions: National Quali Cations Specimen OnlyDocument48 pagesSQ03/N5/01 Biology Section 1-Questions: National Quali Cations Specimen OnlyDoraNo ratings yet
- Olimpiade Bio Semifinal 2014Document22 pagesOlimpiade Bio Semifinal 2014iip casmiriNo ratings yet
- University of Cambridge International Examinations International General Certificate of Secondary EducationDocument16 pagesUniversity of Cambridge International Examinations International General Certificate of Secondary EducationYuli Prapita SariNo ratings yet
- Posteljica I Pupkovina SlikeDocument11 pagesPosteljica I Pupkovina SlikeJulia PutnikNo ratings yet
- Class Xii Biology Time: 90 Minutes General Instructions:: Sample Question Paper (Term I) 2021-22Document20 pagesClass Xii Biology Time: 90 Minutes General Instructions:: Sample Question Paper (Term I) 2021-22Aman KumarNo ratings yet
- Class Xii Biology Time: 90 Minutes General Instructions:: Sample Question Paper (Term I) 2021-22Document20 pagesClass Xii Biology Time: 90 Minutes General Instructions:: Sample Question Paper (Term I) 2021-22Xyz XyzNo ratings yet
- Class Xii Biology Time: 90 Minutes General Instructions:: Sample Question Paper (Term I) 2021-22Document20 pagesClass Xii Biology Time: 90 Minutes General Instructions:: Sample Question Paper (Term I) 2021-22Sriram .RNo ratings yet
- Class Xii Biology Time: 90 Minutes General Instructions:: Sample Question Paper (Term I) 2021-22Document20 pagesClass Xii Biology Time: 90 Minutes General Instructions:: Sample Question Paper (Term I) 2021-22Debangsu GhoshNo ratings yet
- Pathophysiology (Diagram) : Hydatidiform MoleDocument1 pagePathophysiology (Diagram) : Hydatidiform MoleQuintin MangaoangNo ratings yet
- International Indian School, Riyadh: General InstructionsDocument22 pagesInternational Indian School, Riyadh: General InstructionsAltaf Hussain KhanNo ratings yet
- Science 6 Q3 Quiz 1Document2 pagesScience 6 Q3 Quiz 1Joniele Angelo AninNo ratings yet
- Abo Gcuc 2015Document49 pagesAbo Gcuc 2015Laud ArthurNo ratings yet
- Sankalp Proton NEET: Human ReproductionDocument4 pagesSankalp Proton NEET: Human ReproductionComics WorldNo ratings yet
- CirculationDocument134 pagesCirculationDr. Prakash SahNo ratings yet
- (Answer Key) Written Competency ReticulocytesDocument25 pages(Answer Key) Written Competency ReticulocytessaharNo ratings yet
- Class Xii Biology Time: 90 Minutes General Instructions:: Sample Question Paper-1Document23 pagesClass Xii Biology Time: 90 Minutes General Instructions:: Sample Question Paper-1RitishnaNo ratings yet
- Fetal DevelopmentDocument3 pagesFetal DevelopmentBela MillenaNo ratings yet
- Genetics Laboratory ManualDocument69 pagesGenetics Laboratory ManualAyu JumainNo ratings yet
- 0653 s06 QP 1Document16 pages0653 s06 QP 1minamaged628No ratings yet
- Exercise On Transport PDF Vein BloodDocument1 pageExercise On Transport PDF Vein Bloodaliensumsum1010No ratings yet
- Form 5: Chapter 13 Reproduction and GrowthDocument11 pagesForm 5: Chapter 13 Reproduction and Growthapi-3841154No ratings yet
- Developing Human Clinically Oriented Embryology 10th Edition Moore Test BankDocument8 pagesDeveloping Human Clinically Oriented Embryology 10th Edition Moore Test Bankdrerindavisddsybrqsdmajp100% (16)
- Cambridge International General Certificate of Secondary EducationDocument16 pagesCambridge International General Certificate of Secondary EducationAhmed Sherif HelmyNo ratings yet
- Bio Neet Revision Series Human ReproductionDocument133 pagesBio Neet Revision Series Human ReproductionPummy ThakurNo ratings yet
- SMK Serian Term 3 2017 Trial STPM QPDocument9 pagesSMK Serian Term 3 2017 Trial STPM QPViola Voon Li WeiNo ratings yet
- B12 Cell Division MSDocument9 pagesB12 Cell Division MSZenron27No ratings yet
- CS Q.P 1 2019Document16 pagesCS Q.P 1 2019rekicheruNo ratings yet
- Alport SD Ald Thin MembraneDocument48 pagesAlport SD Ald Thin MembraneHignacio AlarcónNo ratings yet
- Hema Summary NotesDocument42 pagesHema Summary NotesJustine Joy Remotigue MantosNo ratings yet
- 12 Preboard-2021Document14 pages12 Preboard-2021Sandeep KNo ratings yet
- Body Fluids and CirculationDocument14 pagesBody Fluids and Circulationictmi45No ratings yet
- Class 12 Bio SP6Document9 pagesClass 12 Bio SP6KiranNo ratings yet
- Biology Sample Paper-6Document10 pagesBiology Sample Paper-6Prasanth MNo ratings yet
- Heridity and EvolutionDocument8 pagesHeridity and EvolutionAmitabh BiswasNo ratings yet
- Development of Extra-Embryonic MembranesDocument7 pagesDevelopment of Extra-Embryonic MembranesAfridi ShaikhNo ratings yet
- P2 2019 SMK Methodist PDFDocument11 pagesP2 2019 SMK Methodist PDFBryanLeeChienYungNo ratings yet
- Class XII Biology 23-24 Pre-Board AnsDocument16 pagesClass XII Biology 23-24 Pre-Board AnsAyushman DharNo ratings yet
- Exercise 1 Bio Sem 2 2020Document4 pagesExercise 1 Bio Sem 2 2020Thurgahini KikaNo ratings yet
- OB BULLETS by Mycobacterium - MDDocument2 pagesOB BULLETS by Mycobacterium - MDCris YumulNo ratings yet
- 06.end of Unit Test Solution U1Document1 page06.end of Unit Test Solution U1OCHANDO MARTINEZ MONICANo ratings yet
- Maternity Nursing An Introductory Text 11th Edition Leifer Test BankDocument25 pagesMaternity Nursing An Introductory Text 11th Edition Leifer Test BankJenniferNicholsonqknj100% (63)
- Blood BookletDocument10 pagesBlood BookletTezdjan HassanNo ratings yet
- Life ScienceDocument15 pagesLife ScienceJedae' JamesNo ratings yet
- (#2) Multiple PregnancyDocument55 pages(#2) Multiple Pregnancymarina_shawkyNo ratings yet
- Nust Applied Biosciences Sample Paper 02Document13 pagesNust Applied Biosciences Sample Paper 02Noor AfshanNo ratings yet
- ArtiDocument13 pagesArtiValeria Dalay Avila LopezNo ratings yet
- Winter 2002 Paper 2 IGCSE Biology CompletedDocument20 pagesWinter 2002 Paper 2 IGCSE Biology CompletedSaif UllahNo ratings yet
- Plants and Organelles: A Compilation from the GenBank® and EMBL data librariesFrom EverandPlants and Organelles: A Compilation from the GenBank® and EMBL data librariesNo ratings yet
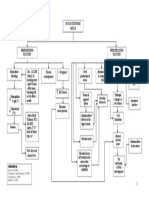
- Supplier Qualification: Constructing A Cause-and-Effect DiagramDocument10 pagesSupplier Qualification: Constructing A Cause-and-Effect DiagramKaren Flores BartoloNo ratings yet
- Project Management Methodology: Processes From The PMBOK Should Be Selected ForDocument10 pagesProject Management Methodology: Processes From The PMBOK Should Be Selected ForKaren Flores BartoloNo ratings yet
- Arachis Hypogaea, 133Document10 pagesArachis Hypogaea, 133Karen Flores BartoloNo ratings yet
- Salvia Sclarea, 134Document3 pagesSalvia Sclarea, 134Karen Flores BartoloNo ratings yet
- The Abo Blood Group System: Unit 4 - Red Blood Cell Groups and HlaDocument10 pagesThe Abo Blood Group System: Unit 4 - Red Blood Cell Groups and HlaKaren Flores BartoloNo ratings yet
- Subgroups of B: Figure 9-7Document10 pagesSubgroups of B: Figure 9-7Karen Flores BartoloNo ratings yet
- Automated Blood Products: Figure 2-1Document10 pagesAutomated Blood Products: Figure 2-1Karen Flores BartoloNo ratings yet
- Selection of Incubation Phase: TABLE 6-2Document10 pagesSelection of Incubation Phase: TABLE 6-2Karen Flores BartoloNo ratings yet
- Shipping Containers: Review QuestionsDocument10 pagesShipping Containers: Review QuestionsKaren Flores BartoloNo ratings yet
- Complement: Tertiary ReactionsDocument10 pagesComplement: Tertiary ReactionsKaren Flores BartoloNo ratings yet
- Phlebotomy and Collection of SamplesDocument10 pagesPhlebotomy and Collection of SamplesKaren Flores BartoloNo ratings yet
- Positional or Modifier Effects of Genes: TABLE 4-2Document10 pagesPositional or Modifier Effects of Genes: TABLE 4-2Karen Flores BartoloNo ratings yet
- TABLE 3-3: Examples of Bag Types and Components That Can Be Made in A Closed SystemDocument10 pagesTABLE 3-3: Examples of Bag Types and Components That Can Be Made in A Closed SystemKaren Flores BartoloNo ratings yet
- 20 Questions On ObDocument5 pages20 Questions On ObCes Espino TorreNo ratings yet
- Placenta PreviaDocument2 pagesPlacenta PreviaIrish Joy S. DecrepitoNo ratings yet
- Obs Gynae DiamsDocument6 pagesObs Gynae DiamsFarrukh Ali KhanNo ratings yet
- Recurrent Pregnancy LossDocument19 pagesRecurrent Pregnancy LossSean NamNo ratings yet
- Background: Abruptio PlacentaeDocument6 pagesBackground: Abruptio PlacentaeEj ZGNo ratings yet
- PlasentaDocument15 pagesPlasentaIpan MahendriyansaNo ratings yet
- 16 Learning ObjectivesDocument5 pages16 Learning Objectivesapi-309893409No ratings yet
- OBS 1stDocument18 pagesOBS 1staqsa ashrafNo ratings yet
- Matrudevobhavaby DR RAnjaneyulu MDDGODocument225 pagesMatrudevobhavaby DR RAnjaneyulu MDDGOAnonymous ZuSPWY2vF100% (2)
- Post Partum Case 1Document47 pagesPost Partum Case 1clarNo ratings yet
- Lecture Notes AnatomyDocument18 pagesLecture Notes AnatomyFau Fau DheoboNo ratings yet
- Adventures in Human BeingDocument11 pagesAdventures in Human BeingShubham DoshiNo ratings yet
- Why Methotrexate Is An Immoral Response To Ectopic PregnancyDocument21 pagesWhy Methotrexate Is An Immoral Response To Ectopic PregnancyelainemenezNo ratings yet
- 3rd and 4th Stage of LabourDocument53 pages3rd and 4th Stage of LabourlisafelixNo ratings yet
- Lecture Guide: Introduction To EmbryologyDocument23 pagesLecture Guide: Introduction To EmbryologyAldrin Hardy PabloNo ratings yet
- Gaumard Catálogo 2014Document232 pagesGaumard Catálogo 2014renucha2010No ratings yet
- Basic Nursing Concepts Skills and Reasoning 1st Edition Treas Test BankDocument16 pagesBasic Nursing Concepts Skills and Reasoning 1st Edition Treas Test Bankclaraninht5sqdj100% (25)
- REFERAT - Ppt.solusio Plasenta ItaDocument18 pagesREFERAT - Ppt.solusio Plasenta ItaMochammad Adam EldiNo ratings yet
- ASSE Project Final ExamDocument7 pagesASSE Project Final ExamMycz DoñaNo ratings yet
- Embryology FlashcardsDocument3 pagesEmbryology FlashcardsAisha YolaNo ratings yet