You might also like
- Factors Associated With Early Smoking Initiation Among Korean AdolescentsDocument5 pagesFactors Associated With Early Smoking Initiation Among Korean AdolescentsTiwi AgustinaNo ratings yet
- Method of Research (Final Na Ito)Document86 pagesMethod of Research (Final Na Ito)Jean Madariaga BalanceNo ratings yet
- Impacts of Smoking on Student HealthDocument47 pagesImpacts of Smoking on Student Healthcafe customercareNo ratings yet
- Family Process and Peer Influences On Substance Use by AdolescentsDocument18 pagesFamily Process and Peer Influences On Substance Use by AdolescentsRanveer Raj BhatnagarNo ratings yet
- 071-005 Factor AssociatedDocument5 pages071-005 Factor AssociatedAzlisonGuilaboBawangNo ratings yet
- Shsconf Erpa2018 01006Document10 pagesShsconf Erpa2018 01006Jodie Junio BaladadNo ratings yet
- Group 2 ResearchDocument16 pagesGroup 2 ResearchlorieferpaloganNo ratings yet
- Chapter i and Chapter II ResearchDocument20 pagesChapter i and Chapter II ResearchMon HaleNo ratings yet
- CHAPTER I With Reference - 2Document10 pagesCHAPTER I With Reference - 2Anjo FernandezNo ratings yet
- A-Research-Study-on-SmokingDocument8 pagesA-Research-Study-on-SmokingMr.anonymous unknownNo ratings yet
- g1 Practical Research 2Document16 pagesg1 Practical Research 2jaymegeramie8No ratings yet
- Attitude of West Negros UniversityDocument27 pagesAttitude of West Negros UniversityjhilyNo ratings yet
- Prevalence and Associated Factors of Smoking in Middle and High School Students: A School-Based Cross-Sectional Study in Zhejiang Province, ChinaDocument6 pagesPrevalence and Associated Factors of Smoking in Middle and High School Students: A School-Based Cross-Sectional Study in Zhejiang Province, ChinafloridaNo ratings yet
- FSS 1150 Final PaperDocument6 pagesFSS 1150 Final Papersaranajem310No ratings yet
- 7-Article Text-12-1-10-20200304 - 2Document5 pages7-Article Text-12-1-10-20200304 - 2Christopher RyalinoNo ratings yet
- Parental Smoking Exposure and Adolescent Smoking TrajectoriesDocument11 pagesParental Smoking Exposure and Adolescent Smoking TrajectoriesMutiara Dumalangga SawitriNo ratings yet
- Keywords: Risk Behaviour, Violence, Health, Well-Being, Peer Relation, Parent RelationDocument10 pagesKeywords: Risk Behaviour, Violence, Health, Well-Being, Peer Relation, Parent RelationmandaNo ratings yet
- Research ProposalDocument13 pagesResearch ProposalMohaiminul IslamNo ratings yet
- Manuscrib Rivan PDFDocument11 pagesManuscrib Rivan PDFFirman SyahNo ratings yet
- Attitude Among Male Students in 2 Public High School in Zamboanguita 1Document11 pagesAttitude Among Male Students in 2 Public High School in Zamboanguita 1Jeanie TabalNo ratings yet
- Review of Related LiteratureDocument9 pagesReview of Related LiteratureJean Calubag CatalanNo ratings yet
- Heliyon: Nurulhuda Mat Hassan, Aniza Abdul Aziz, Rohayah Husain, Norwati Daud, Siti Norazlina JuhariDocument6 pagesHeliyon: Nurulhuda Mat Hassan, Aniza Abdul Aziz, Rohayah Husain, Norwati Daud, Siti Norazlina JuhariIntan NurfadillahNo ratings yet
- Senior High Students' Perceptions of SmokingDocument37 pagesSenior High Students' Perceptions of SmokingLancer MonillaNo ratings yet
- PEER INFLUENCE ON SMOKING DESIRE OF ELEMENTARY STUDENTSDocument8 pagesPEER INFLUENCE ON SMOKING DESIRE OF ELEMENTARY STUDENTSdevintanauraNo ratings yet
- Profil Kesehatan 2 TugasDocument6 pagesProfil Kesehatan 2 TugasIngNo ratings yet
- ASchool-BasedStudyoftheInfluenceofStudentsRelationshipAPJCP Volume19 IssueS1 Pages7-121Document7 pagesASchool-BasedStudyoftheInfluenceofStudentsRelationshipAPJCP Volume19 IssueS1 Pages7-121king12No ratings yet
- Try and Try Again: Qualitative Insights Into Adolescent Smoking Experimentation and Notions of AddictionDocument8 pagesTry and Try Again: Qualitative Insights Into Adolescent Smoking Experimentation and Notions of AddictionChanelle Honey VicedoNo ratings yet
- Chapter 1 (Finally)Document19 pagesChapter 1 (Finally)izayoiNo ratings yet
- Baby Thesis The Effects of Vices On Academic Peformance of StudentsDocument21 pagesBaby Thesis The Effects of Vices On Academic Peformance of StudentsDianne Monique Sibayan92% (13)
- Devinta Naura JournalDocument8 pagesDevinta Naura JournaldevintanauraNo ratings yet
- Smoking Cessation in OANARIDocument29 pagesSmoking Cessation in OANARINickoleQuijalvoPeraltaNo ratings yet
- Literature Review ON Peer Influence On Adolescent'S Substance UseDocument20 pagesLiterature Review ON Peer Influence On Adolescent'S Substance UseLara AkinpeluNo ratings yet
- LIVED EXPERIENCES OF ALCOHOLIC DRINKING IN COLLEGEDocument14 pagesLIVED EXPERIENCES OF ALCOHOLIC DRINKING IN COLLEGETrinity .vlogsNo ratings yet
- Biblo Annat DraftDocument6 pagesBiblo Annat Draftmcheung04No ratings yet
- Harvey ResearchDocument22 pagesHarvey ResearchEgi Mark GallardeNo ratings yet
- Beige Pastel Minimalist Thesis Defense PresentationDocument21 pagesBeige Pastel Minimalist Thesis Defense Presentationw6szgb8wxqNo ratings yet
- Drug and Alcohol DependenceDocument7 pagesDrug and Alcohol DependenceNur Melizza, S.Kep., NsNo ratings yet
- Predictors of Cigarette Smoking Among AdolescentsDocument10 pagesPredictors of Cigarette Smoking Among AdolescentsPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Quiz AbstrackDocument4 pagesQuiz AbstracknielresimanukNo ratings yet
- Effects of Health Education On Cigarette Smoking Habits of Young Adults in Tertiary Institutions in A Northern Nigerian StateDocument13 pagesEffects of Health Education On Cigarette Smoking Habits of Young Adults in Tertiary Institutions in A Northern Nigerian StateGaoudam NatarajanNo ratings yet
- Relationship Between Knowledge, Attitudes and Smoking Behavior in Teenage BoysDocument8 pagesRelationship Between Knowledge, Attitudes and Smoking Behavior in Teenage BoysMukhsin ANo ratings yet
- EpidemiologyyDocument7 pagesEpidemiologyyw6szgb8wxqNo ratings yet
- Ash 648Document7 pagesAsh 648Aryani PujiyantiNo ratings yet
- Hanging Out Trends in Substance Use Among Youth in A Private Tertiary Institution in Nigeria A Qualitative StudyDocument21 pagesHanging Out Trends in Substance Use Among Youth in A Private Tertiary Institution in Nigeria A Qualitative StudyGlobal Research and Development ServicesNo ratings yet
- Peer pressure and smoking: the complex role of research methodsDocument5 pagesPeer pressure and smoking: the complex role of research methodsJessica BaldemorNo ratings yet
- The Effect of Tobacco Smoking Among Third Year Student Nurse in The University of LuzonDocument6 pagesThe Effect of Tobacco Smoking Among Third Year Student Nurse in The University of LuzonNeil Christian TadzNo ratings yet
- Knowledge, Attitude and Practices of Alcohol and Smoking Among Undergraduate Oral Health Students at A South African UniversityDocument4 pagesKnowledge, Attitude and Practices of Alcohol and Smoking Among Undergraduate Oral Health Students at A South African UniversityAamirNo ratings yet
- Parental Role in Adoles Subst AbuseDocument4 pagesParental Role in Adoles Subst AbuseAdina CipariuNo ratings yet
- Reasons behind alcohol and cigarette use among Laak National High School studentsDocument8 pagesReasons behind alcohol and cigarette use among Laak National High School studentspaWpaO HDNo ratings yet
- 27Document11 pages27Amit TamboliNo ratings yet
- Fss 1150 Rough DraftDocument7 pagesFss 1150 Rough Draftsaranajem310No ratings yet
- Final ResearchsdsDocument24 pagesFinal ResearchsdsVicente AngelesNo ratings yet
- Practical Research Group 5Document17 pagesPractical Research Group 5jryl ortgaNo ratings yet
- Level of Involvement in Smoking, Drinking and Drugs AbuseDocument35 pagesLevel of Involvement in Smoking, Drinking and Drugs Abusehyacinth_sobebe100% (2)
- 1-Weight-Related Teasing, Coping Strategies and Self-Esteem in Obese University StudentsDocument14 pages1-Weight-Related Teasing, Coping Strategies and Self-Esteem in Obese University StudentsClinical and Counselling Psychology ReviewNo ratings yet
- Examining The Relationshings Between Parent Experiences and Youth Self-Reports of Slapping-SpankingDocument8 pagesExamining The Relationshings Between Parent Experiences and Youth Self-Reports of Slapping-SpankingCarla Isabel Ramírez SantosNo ratings yet
- GROUP 2 ResearchDocument27 pagesGROUP 2 ResearchKatherine AliceNo ratings yet
- Youth Smoking Research PaperDocument8 pagesYouth Smoking Research Paperafedtkjdz100% (1)
- Ok 4Document10 pagesOk 4floridaNo ratings yet
- Prevalence and Associated Factors of Smoking in Middle and High School Students: A School-Based Cross-Sectional Study in Zhejiang Province, ChinaDocument6 pagesPrevalence and Associated Factors of Smoking in Middle and High School Students: A School-Based Cross-Sectional Study in Zhejiang Province, ChinafloridaNo ratings yet
- Ok 1Document5 pagesOk 1floridaNo ratings yet
- Ok 4Document10 pagesOk 4floridaNo ratings yet
- Capaian Pis PK Tahun 2017 Upt Puskesmas Ngoresan Dinas Kesehatan Kota Surakarta NO. RW RT 001 RT 002 RT 003 RT 004 RT 005 RT 006 JumlahDocument1 pageCapaian Pis PK Tahun 2017 Upt Puskesmas Ngoresan Dinas Kesehatan Kota Surakarta NO. RW RT 001 RT 002 RT 003 RT 004 RT 005 RT 006 JumlahfloridaNo ratings yet
- By Feri Boedi Artomo, Muh. SulchanDocument1 pageBy Feri Boedi Artomo, Muh. SulchanFloerida Frida ApriliaNo ratings yet
- Solid State Physics by Kettel Chapter 4Document17 pagesSolid State Physics by Kettel Chapter 4Taseer BalochNo ratings yet
- Introduction To HAPDocument6 pagesIntroduction To HAPMaheshSukhadiyaNo ratings yet
- Test Paper Trigonometric Functions and Equations PDFDocument9 pagesTest Paper Trigonometric Functions and Equations PDFkaushalshah28598No ratings yet
- CorrectDocument45 pagesCorrectaskerman 3No ratings yet
- DLP November 7 11 2022Document11 pagesDLP November 7 11 2022Harvey RabinoNo ratings yet
- Class Test Dec 10Document6 pagesClass Test Dec 10trudes100No ratings yet
- Communication TasksDocument19 pagesCommunication Taskswaqas08100% (4)
- Object Oriented Programming (OOPS) : Java Means Durga SirDocument2 pagesObject Oriented Programming (OOPS) : Java Means Durga SirROHIT JAINNo ratings yet
- Handbook Valve Technology 03.04.2020Document132 pagesHandbook Valve Technology 03.04.2020Ramazan YaşarNo ratings yet
- Pate, M. B., Evaporators and Condensers For Refrigeration and Air-Conditioning Systems, in Boilers, Evaporators andDocument1 pagePate, M. B., Evaporators and Condensers For Refrigeration and Air-Conditioning Systems, in Boilers, Evaporators andpete pansNo ratings yet
- El 5036 V2 PDFDocument86 pagesEl 5036 V2 PDFCriss TNo ratings yet
- Management Quality ManagementDocument7 pagesManagement Quality ManagementJasmine LimNo ratings yet
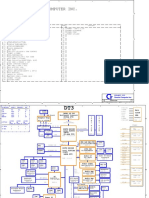
- Acer Aspire 1710 (Quanta DT3) PDFDocument35 pagesAcer Aspire 1710 (Quanta DT3) PDFMustafa AkanNo ratings yet
- Operation and Safety Manual: Ansi As/NzsDocument116 pagesOperation and Safety Manual: Ansi As/NzsMuhammad AwaisNo ratings yet
- TH - TB Series (Helical GearBox Catalog)Document94 pagesTH - TB Series (Helical GearBox Catalog)poorianaNo ratings yet
- Defibrelator ch1Document31 pagesDefibrelator ch1د.محمد عبد المنعم الشحاتNo ratings yet
- Hill, Tomlinson (2003) - Coursebook Listening ActivitiesDocument11 pagesHill, Tomlinson (2003) - Coursebook Listening ActivitiesMelina San Miguel GarciaNo ratings yet
- Advances in Littorinid BiologyDocument193 pagesAdvances in Littorinid Biologyasaad lahmarNo ratings yet
- SPE 63041 Design and Installation of Sand Separation and Handling SystemDocument10 pagesSPE 63041 Design and Installation of Sand Separation and Handling Systemalexalek2000No ratings yet
- ASTM C1019 GroutingDocument4 pagesASTM C1019 GroutingTrung Hieu NguyenNo ratings yet
- Lecture Notes Natural LawDocument52 pagesLecture Notes Natural LawVina EstherNo ratings yet
- 16656561931665656193FinancialModellingProfessional 1 (1) CompressedDocument17 pages16656561931665656193FinancialModellingProfessional 1 (1) CompressedDharmik UndaviyaNo ratings yet
- ESDIS05161 DMP For DPs Template PDFDocument15 pagesESDIS05161 DMP For DPs Template PDFneerajshukla246829No ratings yet
- Geotechnical Scope of Work For ERL Unit-2Document75 pagesGeotechnical Scope of Work For ERL Unit-2smjohirNo ratings yet
- UKPSC JE Civil 2024 Exam (Technical) - ScheduleDocument4 pagesUKPSC JE Civil 2024 Exam (Technical) - ScheduleIES-GATEWizNo ratings yet
- TUDelft Clay Suction PDFDocument8 pagesTUDelft Clay Suction PDFDing LiuNo ratings yet
- HXPM8XBBYY19065T2CDocument1 pageHXPM8XBBYY19065T2CЕвгений ГрязевNo ratings yet
- SummaryDocument3 pagesSummaryОля ВласійчукNo ratings yet
- Troubleshooting Edge Quality: Mild SteelDocument14 pagesTroubleshooting Edge Quality: Mild SteelAnonymous U6yVe8YYCNo ratings yet
- Prof. Hanumant Pawar: GeomorphologyDocument15 pagesProf. Hanumant Pawar: GeomorphologySHAIK CHAND PASHANo ratings yet