You might also like
- Pulmonary Function Tests in Clinical PracticeFrom EverandPulmonary Function Tests in Clinical PracticeAli AltalagRating: 5 out of 5 stars5/5 (1)
- Bronchial AsthmaDocument2 pagesBronchial AsthmaRubz JeanNo ratings yet
- Understanding COPD: A Case Study on Diagnosis and Nutrition TherapyDocument11 pagesUnderstanding COPD: A Case Study on Diagnosis and Nutrition TherapyFajer AleitanNo ratings yet
- Respiratory Air Flow and VolumeDocument7 pagesRespiratory Air Flow and Volumeshwuyng91100% (3)
- Presentation 4 3Document25 pagesPresentation 4 3api-276974907No ratings yet
- Respiration 6 PDFDocument27 pagesRespiration 6 PDFSardar jiNo ratings yet
- LAB ActivityDocument2 pagesLAB ActivityNicole AquinoNo ratings yet
- COPD Case Study Reveals Mechanisms of DyspneaDocument27 pagesCOPD Case Study Reveals Mechanisms of DyspneaMelissa MakhoulNo ratings yet
- Resp Yamashita PulmonaryFunctionTests NotesDocument13 pagesResp Yamashita PulmonaryFunctionTests Notes1233211qwerasdNo ratings yet
- Dr. Rowshne Jahan Spirometry Presentation-1Document40 pagesDr. Rowshne Jahan Spirometry Presentation-1Shahadat Hossain BabuNo ratings yet
- Spirometry InterpretationDocument4 pagesSpirometry InterpretationSSNo ratings yet
- DR Ambreen Shams NephrologistDocument58 pagesDR Ambreen Shams NephrologistAamer NaeemNo ratings yet
- Jps R 07011508Document3 pagesJps R 07011508AbhiramNo ratings yet
- UntitledDocument4 pagesUntitledRafsan HossainNo ratings yet
- BBB 1 - Pulmonary Function Tests InterpretationDocument14 pagesBBB 1 - Pulmonary Function Tests InterpretationArhanNo ratings yet
- Topic 2 COPD and AsthmaDocument18 pagesTopic 2 COPD and AsthmaCaitlynNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument8 pagesChronic Obstructive Pulmonary DiseaseYessamin Paith RoderosNo ratings yet
- 0 - CSBC-321 Assignment 2 CHCS-2017-045Document13 pages0 - CSBC-321 Assignment 2 CHCS-2017-045JessieNo ratings yet
- CopdDocument29 pagesCopdRidha SyahputraNo ratings yet
- Emphysema BrochureDocument2 pagesEmphysema Brochureapi-242394302No ratings yet
- Spirometry (PPT & Words) 1Document5 pagesSpirometry (PPT & Words) 1Fluffyyy BabyyyNo ratings yet
- Using The Pathophysiology of Obstructive Sleep Apnea To Teach Cardiopulmonary IntegrationDocument7 pagesUsing The Pathophysiology of Obstructive Sleep Apnea To Teach Cardiopulmonary IntegrationAdiel OjedaNo ratings yet
- Nurs 2200 Asthma Case StudyDocument6 pagesNurs 2200 Asthma Case StudyBrandee StantonNo ratings yet
- Bronchitis: Edited by Ignacio Martín-LoechesDocument200 pagesBronchitis: Edited by Ignacio Martín-LoechesskilmagNo ratings yet
- Onbrez June 2014Document32 pagesOnbrez June 2014NateStephBarnardNo ratings yet
- Pulmonary Function Test Part 1 PPTDR Mona AllangawiDocument84 pagesPulmonary Function Test Part 1 PPTDR Mona Allangawisachin10dulkarNo ratings yet
- COPD Guide Covers Causes, Symptoms, DiagnosisDocument5 pagesCOPD Guide Covers Causes, Symptoms, DiagnosisElvando SimatupangNo ratings yet
- HSNS264 Assessment 1Document6 pagesHSNS264 Assessment 1Sophie AndersonNo ratings yet
- Mechanics of Respiration: Functions of The Respiratory SystemDocument7 pagesMechanics of Respiration: Functions of The Respiratory SystemNorrifhan Akmal IsmailNo ratings yet
- Interpreting Pulmonary Function TestsDocument6 pagesInterpreting Pulmonary Function TestsVittorio Di PaoloNo ratings yet
- Biology QuizDocument8 pagesBiology Quizkathy abreuNo ratings yet
- COPD Vs RLDDocument64 pagesCOPD Vs RLDXine DeeNo ratings yet
- Respiratory Impairment and The Aging Lung - A Novel Paradigm For Assessing Pulmonary FunctionDocument12 pagesRespiratory Impairment and The Aging Lung - A Novel Paradigm For Assessing Pulmonary FunctionSrilatha GirishNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) Is A Condition ofDocument12 pagesChronic Obstructive Pulmonary Disease (COPD) Is A Condition ofDiana Jalaynie S. SambolawanNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) Is A Condition ofDocument12 pagesChronic Obstructive Pulmonary Disease (COPD) Is A Condition ofDiana Jalaynie S. SambolawanNo ratings yet
- Case Studies: Restrictive and Obstructive Respiratory Conditions Case Study # 1Document5 pagesCase Studies: Restrictive and Obstructive Respiratory Conditions Case Study # 1psyarjavierNo ratings yet
- Case Studies: Restrictive and Obstructive Respiratory Conditions Case Study # 1Document5 pagesCase Studies: Restrictive and Obstructive Respiratory Conditions Case Study # 1psyarjavierNo ratings yet
- Pulmonary Function TestsDocument16 pagesPulmonary Function TestsRashed ShatnawiNo ratings yet
- Practice EamDocument35 pagesPractice EamMYKRISTIE JHO MENDEZNo ratings yet
- Respiratory Physiology: Lung Volumes and CapacitiesDocument35 pagesRespiratory Physiology: Lung Volumes and CapacitiesNur Faizah Ahmad AriffNo ratings yet
- FT Kardiorespirasi - CompressedDocument101 pagesFT Kardiorespirasi - CompressedWahdina PratamaNo ratings yet
- PN21 Health and Healing - Pre-Class Activities - Test 2 PDFDocument33 pagesPN21 Health and Healing - Pre-Class Activities - Test 2 PDFRachel HomesNo ratings yet
- Hypoxemia Interpretation of SpirometryDocument55 pagesHypoxemia Interpretation of SpirometryRLI23nyNo ratings yet
- Batuk EfektifDocument11 pagesBatuk EfektifDadi ArdiansyahNo ratings yet
- COPD Risk Factors, Pathogenesis, PathophysiologyDocument5 pagesCOPD Risk Factors, Pathogenesis, PathophysiologyMarshel BudiarsaNo ratings yet
- ER Treatment for Asthmatic PatientDocument4 pagesER Treatment for Asthmatic PatientEver Green100% (2)
- Respiratory PhysiologyDocument9 pagesRespiratory PhysiologyBrent TorresNo ratings yet
- Study Case FinalDocument6 pagesStudy Case FinalthouonesandNo ratings yet
- Case PresentationDocument12 pagesCase PresentationMary Mae BuellaNo ratings yet
- Ageing Lungs2Document3 pagesAgeing Lungs2David John BalanagNo ratings yet
- Jurnal Dari UnairDocument8 pagesJurnal Dari Unairfauzan mashudiNo ratings yet
- Pulmonary Function TestsDocument29 pagesPulmonary Function TestsOrion JohnNo ratings yet
- PT Case: Copd Exacerbation: DedicationDocument10 pagesPT Case: Copd Exacerbation: DedicationDianaLopezBorjaNo ratings yet
- COPD Case StudyDocument6 pagesCOPD Case Studyvanessa100% (1)
- Chronic Obsrtructive Pulmonary DiseaseDocument11 pagesChronic Obsrtructive Pulmonary Diseasepreeti sharmaNo ratings yet
- COPD Risk Factors & Spirometry StagingDocument38 pagesCOPD Risk Factors & Spirometry StagingKudingLimMingYaoNo ratings yet
- Anesth in Advanced Vent SupportDocument14 pagesAnesth in Advanced Vent SupportFrancisco DuqueNo ratings yet
- Westjmed00276 0040Document9 pagesWestjmed00276 0040Marc AbellaNo ratings yet
- COPD Nursing Care GuideDocument16 pagesCOPD Nursing Care GuideJay-ar Zars0% (1)
- NEET PG 2013 Question Paper With SolutionsDocument2,164 pagesNEET PG 2013 Question Paper With SolutionsSK RaulNo ratings yet
- Examination of The ThroatDocument10 pagesExamination of The Throatsejal3vijNo ratings yet
- Bac Culture Idn Prac RecDocument7 pagesBac Culture Idn Prac Recsejal3vijNo ratings yet
- Ear ExaminationDocument13 pagesEar Examinationsejal3vijNo ratings yet
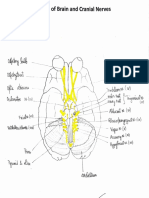
- Base of Brain and Cranial NervesDocument9 pagesBase of Brain and Cranial Nervessejal3vijNo ratings yet
- Asclepius - A Unit of Rotaract Apollo: Creating An Impact-One Cause at A TimeDocument7 pagesAsclepius - A Unit of Rotaract Apollo: Creating An Impact-One Cause at A Timesejal3vijNo ratings yet
- Reflex Functions of BrainstemDocument17 pagesReflex Functions of Brainstemsejal3vijNo ratings yet
- CamScanner App Scans Documents EasilyDocument2 pagesCamScanner App Scans Documents Easilysejal3vij50% (6)
- Lec 23 - Spinal Reflexes & Their AdaptabilityDocument2 pagesLec 23 - Spinal Reflexes & Their Adaptabilitysejal3vijNo ratings yet
- NEET PG 2013 Question Paper With SolutionsDocument2,164 pagesNEET PG 2013 Question Paper With SolutionsSK RaulNo ratings yet
- Sia PhysiologyDocument34 pagesSia Physiologysejal3vijNo ratings yet
- Sia AnatomyDocument15 pagesSia Anatomysejal3vij100% (3)
- Sia BiochemistryDocument8 pagesSia Biochemistrysejal3vijNo ratings yet
- NEET PG 2014 Question Paper With SolutionsDocument2,472 pagesNEET PG 2014 Question Paper With SolutionsSK RaulNo ratings yet
- Muscle Inserted into Floor of Intertubercular SulcusDocument1,588 pagesMuscle Inserted into Floor of Intertubercular Sulcussejal3vijNo ratings yet
- Protein Metabolism - Urea CycleDocument2 pagesProtein Metabolism - Urea Cyclesejal3vijNo ratings yet
- Materials RequiredDocument14 pagesMaterials Requiredsejal3vijNo ratings yet
- Book of The Dead Becoming God in AncientDocument12 pagesBook of The Dead Becoming God in Ancientsejal3vij100% (2)
- Surgical SutureDocument10 pagesSurgical Suturesejal3vijNo ratings yet
- Oncology and Infectious Diseases in Anci PDFDocument119 pagesOncology and Infectious Diseases in Anci PDFsejal3vijNo ratings yet
- Band 2 eDocument58 pagesBand 2 eIonaş Claudia Ramona100% (1)
- The Transition to Computer-Based FE Exams for Chemical EngineersDocument21 pagesThe Transition to Computer-Based FE Exams for Chemical EngineersNNo ratings yet
- WEG Guia de Instalacao pws5610 Quick Guide English PDFDocument1 pageWEG Guia de Instalacao pws5610 Quick Guide English PDFÁgó AttilaNo ratings yet
- Postdoctoral Research Associate in Functional Organic MaterialsDocument6 pagesPostdoctoral Research Associate in Functional Organic MaterialsTheo GazisNo ratings yet
- WAVES FORM 5the diagram, identify the followingDocument52 pagesWAVES FORM 5the diagram, identify the followingHuda IdrisNo ratings yet
- New Correlations For Predicting Two Phase Electrical SubmersibleDocument11 pagesNew Correlations For Predicting Two Phase Electrical SubmersibleNicolás Ruiz FuentesNo ratings yet
- Morteza MirzaeiDocument3 pagesMorteza MirzaeiUmitNo ratings yet
- Plant Toxicology, Fourth Edition (Books in Soils, Plants, and The Environment) PDFDocument664 pagesPlant Toxicology, Fourth Edition (Books in Soils, Plants, and The Environment) PDFFahad JavedNo ratings yet
- ConMed v. Cosmescu Et. Al.Document28 pagesConMed v. Cosmescu Et. Al.PriorSmartNo ratings yet
- Epidemiology and Etiology of Peptic Ulcer DiseaseDocument5 pagesEpidemiology and Etiology of Peptic Ulcer DiseaseDeepali Mahajan ChaudhariNo ratings yet
- Microflow Air Sampler User ManualDocument31 pagesMicroflow Air Sampler User Manualira rahmaNo ratings yet
- Spring 2009 Midterm Opkst Mth601Document10 pagesSpring 2009 Midterm Opkst Mth601Khurram NadeemNo ratings yet
- Poem PDFDocument6 pagesPoem PDFTaylor JohnsNo ratings yet
- Capacitive Touch Sensing, MSP430™ Slider and Wheel Tuning GuideDocument18 pagesCapacitive Touch Sensing, MSP430™ Slider and Wheel Tuning GuideFábio Carvalho FurtadoNo ratings yet
- Major Project ReportDocument49 pagesMajor Project ReportMohini BhartiNo ratings yet
- Downol PmaDocument2 pagesDownol Pmavanhung68100% (1)
- Roof Truss Installation GuideDocument12 pagesRoof Truss Installation GuideAwang Mahardy67% (3)
- Equity ValuationDocument18 pagesEquity ValuationAbhishek NagpalNo ratings yet
- Tubo Optiflux 2000 - Manual PDFDocument48 pagesTubo Optiflux 2000 - Manual PDFRonaldo Damasceno EmerichNo ratings yet
- Gmat Clinic Course Notes PDFDocument213 pagesGmat Clinic Course Notes PDFDavid ThompsonNo ratings yet
- G650 Unimog UL1750 RAAF Data Summary 0Document4 pagesG650 Unimog UL1750 RAAF Data Summary 0Jimmy50% (2)
- Roland RD-800 Manuale Stage PianoDocument64 pagesRoland RD-800 Manuale Stage PianoAlberto FicheraNo ratings yet
- Probability As A General Concept Can Be Defined As The Chance of An Event OccurDocument14 pagesProbability As A General Concept Can Be Defined As The Chance of An Event OccurMuhammad Adnan KhalidNo ratings yet
- Lecture Drugs in Sport - NotesDocument14 pagesLecture Drugs in Sport - NotesDavid FornitoNo ratings yet
- FM 4 Fluid Kinematics CompleteDocument48 pagesFM 4 Fluid Kinematics Completeالياس يونس مرغلانيNo ratings yet
- IBPhysics Particle Practice KeyDocument2 pagesIBPhysics Particle Practice KeyOnur YavuzcetinNo ratings yet
- STARZ Schedule 2016 12Document118 pagesSTARZ Schedule 2016 12Oscar V100% (1)
- Range Safety Regulations and DocumentsDocument11 pagesRange Safety Regulations and Documentsjakehunter24No ratings yet
- Yutra 3Document31 pagesYutra 3ကိုနေဝင်းNo ratings yet
- Week 3 Ipe Review ModuleDocument2 pagesWeek 3 Ipe Review ModuleDarren Ian MaalihanNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (41)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)