You might also like
- Experiments Handbook: An overview of how and when to validate hypotheses. And whith whom.From EverandExperiments Handbook: An overview of how and when to validate hypotheses. And whith whom.No ratings yet
- Nir Eyal's Hooked: Proven Strategies for Getting Up to Speed Faster and Smarter SummaryFrom EverandNir Eyal's Hooked: Proven Strategies for Getting Up to Speed Faster and Smarter SummaryRating: 4 out of 5 stars4/5 (5)
- Client Initial Evaluation Soap NoteDocument8 pagesClient Initial Evaluation Soap Noteapi-582889983No ratings yet
- Discontinuation Discharge NoteDocument5 pagesDiscontinuation Discharge Noteapi-582004078No ratings yet
- Osce Evaluation RevisedDocument5 pagesOsce Evaluation Revisedapi-582889983No ratings yet
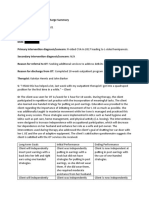
- Discharge SummaryDocument3 pagesDischarge Summaryapi-582889983No ratings yet
- Occupational Profile and Intervention Plan Final Edits 630Document18 pagesOccupational Profile and Intervention Plan Final Edits 630api-275328597No ratings yet
- CC StrokeDocument13 pagesCC Strokeapi-436090845100% (1)
- FW Client Evaluation 2021 1 1Document3 pagesFW Client Evaluation 2021 1 1api-644828371No ratings yet
- Contact Note For Fourth VisitDocument2 pagesContact Note For Fourth Visitapi-253994356No ratings yet
- Discharge NoteDocument4 pagesDischarge Noteapi-583550699No ratings yet
- Edited Adm Smaw m4Document22 pagesEdited Adm Smaw m4Wilfred LlapitanNo ratings yet
- Case Study CHNDocument5 pagesCase Study CHNIsaiah RabangNo ratings yet
- DawnsoapDocument3 pagesDawnsoapapi-338566712No ratings yet
- Rietz Discontinuation NoteDocument4 pagesRietz Discontinuation Noteapi-435782808No ratings yet
- Treatment Plan Name RemovedDocument2 pagesTreatment Plan Name Removedapi-582004078No ratings yet
- Discharge NoteDocument4 pagesDischarge Noteapi-4863293120% (1)
- Soap Note 2 Community ClientDocument12 pagesSoap Note 2 Community Clientapi-271984934No ratings yet
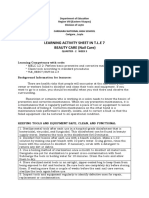
- Learner'S Packet No. 2 Quarter 1Document4 pagesLearner'S Packet No. 2 Quarter 1LETECIA BAJONo ratings yet
- Performance Task Quarter 1 Nail Care ServicesDocument8 pagesPerformance Task Quarter 1 Nail Care Servicesfaye cuevas100% (1)
- Checklst 202Document23 pagesChecklst 202Aron NovesterosNo ratings yet
- Technology and Livelihood Education: Quarter 2 - Module 3: Front Office ServicesDocument28 pagesTechnology and Livelihood Education: Quarter 2 - Module 3: Front Office ServicesREYNOLD MILLONDAGANo ratings yet
- Discharge Summary Adult Community ClientDocument3 pagesDischarge Summary Adult Community ClientcvNo ratings yet
- Discharge Summary 3 5Document3 pagesDischarge Summary 3 5api-517567016No ratings yet
- Dwnload Full Pedrettis Occupational Therapy Practice Skills For Physical Dysfunction 7th Edition Pendleton Test Bank PDFDocument36 pagesDwnload Full Pedrettis Occupational Therapy Practice Skills For Physical Dysfunction 7th Edition Pendleton Test Bank PDFsportfulscenefulzb3nh100% (11)
- Lpe2301 SCL Worksheet 8 Sem2.20.21 - 20210602093115Document3 pagesLpe2301 SCL Worksheet 8 Sem2.20.21 - 20210602093115KU BONo ratings yet
- CHCAGE005 Student Assessment Booklet AGE ID 97114 Non Workplace 3Document64 pagesCHCAGE005 Student Assessment Booklet AGE ID 97114 Non Workplace 3Francis Dave Peralta Bitong0% (1)
- Occupational Therapy Discharge SummaryDocument4 pagesOccupational Therapy Discharge Summaryapi-518285126No ratings yet
- Illustration 7 8 Module 3Document24 pagesIllustration 7 8 Module 3Drei Nathan Valdizno100% (1)
- TLE 7 8 Q2 Mod2 Care Giving V4Document24 pagesTLE 7 8 Q2 Mod2 Care Giving V4Claudine Simeon PiñeraNo ratings yet
- WEEK-4 - LectureDocument2 pagesWEEK-4 - LectureBritney TamuraNo ratings yet
- Farah Comel - c6 BurstDocument60 pagesFarah Comel - c6 BurstFarah SyazwaniNo ratings yet
- Appendix 2 - Template - Final Task 2 - Write Your Obligations and Needs in Your Daily RoleDocument6 pagesAppendix 2 - Template - Final Task 2 - Write Your Obligations and Needs in Your Daily RoleCamilo JimenezNo ratings yet
- ReportDocument22 pagesReportapi-375073856No ratings yet
- Week 6 Treatment Plan 1Document2 pagesWeek 6 Treatment Plan 1api-517780146No ratings yet
- Discharge Note 1Document2 pagesDischarge Note 1api-253994356No ratings yet
- Grade 8 AFA Crop Production 1 PDFDocument23 pagesGrade 8 AFA Crop Production 1 PDFKent Timothy Salazar71% (17)
- 4jendiscontinuation NoteDocument3 pages4jendiscontinuation Noteapi-487924214No ratings yet
- TLE7 Q2 Episode-6 SLMDocument4 pagesTLE7 Q2 Episode-6 SLMCaryll BaylonNo ratings yet
- Activity Sheet in Technology and Livelihood EducationDocument4 pagesActivity Sheet in Technology and Livelihood EducationJOVANE BARRIOSNo ratings yet
- TLE-Carpentry 7 - 8 - Module 4 - Performing Basic Preventive Maintenance - V2Document22 pagesTLE-Carpentry 7 - 8 - Module 4 - Performing Basic Preventive Maintenance - V2ron8deleon8No ratings yet
- Artfact 3 Occupational Therapy Discharge SummaryDocument4 pagesArtfact 3 Occupational Therapy Discharge Summaryapi-517998988No ratings yet
- MKT412 FinaalDocument3 pagesMKT412 FinaalNayeem Rumman Julhash 1911185642No ratings yet
- Tle 2Document18 pagesTle 2Bryant Howell AyuyaoNo ratings yet
- TLE8 Q2 W 2 HousekeepingDocument18 pagesTLE8 Q2 W 2 HousekeepingSalve PetilunaNo ratings yet
- Tle10 Eim10 Q1 M7Document13 pagesTle10 Eim10 Q1 M7Ramil ObraNo ratings yet
- At Device PaperDocument12 pagesAt Device Paperapi-275328597No ratings yet
- LAS 34 in TLE 7 BEATY CARESY.2021 2022Document12 pagesLAS 34 in TLE 7 BEATY CARESY.2021 2022Rigor GopoNo ratings yet
- NEBOSH IDIP - ID1 QN Paper Part-1Document7 pagesNEBOSH IDIP - ID1 QN Paper Part-1mehroof aliNo ratings yet
- Tle Caregiving 7 Third Quarter Set A BDocument25 pagesTle Caregiving 7 Third Quarter Set A BJohn Renzel FabroNo ratings yet
- Creativity Innovation Critical Thinking WorkbookDocument25 pagesCreativity Innovation Critical Thinking WorkbookGJT R345No ratings yet
- K To 12 Dressmaking and Tailoring Learning ModulesDocument132 pagesK To 12 Dressmaking and Tailoring Learning ModulesHari Ng Sablay94% (142)
- CMA Skill Practice! Practice Test Questions for the Certified Medical Assistant TestFrom EverandCMA Skill Practice! Practice Test Questions for the Certified Medical Assistant TestNo ratings yet
- The Manager’s Guide to Business Continuity Exercises: Testing Your PlanFrom EverandThe Manager’s Guide to Business Continuity Exercises: Testing Your PlanNo ratings yet
- Summary of Hooked: by Nir Eyal with Ryan Hoover | Includes AnalysisFrom EverandSummary of Hooked: by Nir Eyal with Ryan Hoover | Includes AnalysisNo ratings yet
- Life Cycle of a Process PlantFrom EverandLife Cycle of a Process PlantMahdi NouriNo ratings yet
- Treatment CompetencyDocument2 pagesTreatment Competencyapi-575381607No ratings yet
- Cqi Project Presentation 2Document7 pagesCqi Project Presentation 2api-575381607No ratings yet
- Discontinuation DC NoteDocument5 pagesDiscontinuation DC Noteapi-575381607No ratings yet
- Reflective Theories Writing AssignmentDocument7 pagesReflective Theories Writing Assignmentapi-575381607No ratings yet
- Cognitive Activity - Alternate SolutionsDocument3 pagesCognitive Activity - Alternate Solutionsapi-575381607No ratings yet
- FW ProjectDocument2 pagesFW Projectapi-575381607No ratings yet
- Epb - NDT ResearchDocument20 pagesEpb - NDT Researchapi-575381607No ratings yet
- PDT FwiiDocument3 pagesPDT Fwiiapi-575381607No ratings yet
- Interview With Lynne MurrayDocument3 pagesInterview With Lynne MurrayPaola CastellanosNo ratings yet
- Mutations Genetic DisordersDocument25 pagesMutations Genetic DisordersKimberly Lopez100% (1)
- VertigoandDizziness 2Document50 pagesVertigoandDizziness 2Au Ah Gelap100% (1)
- Fosinopril SodiumDocument3 pagesFosinopril Sodiumapi-3797941100% (1)
- Rule: Medicare: Physician Fee Schedule (CY 2006) Payment Policies and Realtive Value UnitsDocument362 pagesRule: Medicare: Physician Fee Schedule (CY 2006) Payment Policies and Realtive Value UnitsJustia.comNo ratings yet
- Psych Case StudyDocument94 pagesPsych Case Studyrhia casinillo100% (4)
- GuaifenesinDocument2 pagesGuaifenesincoooleNo ratings yet
- Cervical Inflammation Client Handout FinalDocument2 pagesCervical Inflammation Client Handout Finalapi-290098737No ratings yet
- FARTER PCNE Classification V9-0Document10 pagesFARTER PCNE Classification V9-0milatul amaliaNo ratings yet
- Sleep Pattern DisturbanceDocument4 pagesSleep Pattern DisturbanceVirusNo ratings yet
- 50 Item Psychiatric Nursing ExamDocument8 pages50 Item Psychiatric Nursing Examalexis_borjNo ratings yet
- Oxygen InhalationDocument44 pagesOxygen InhalationDr. Jayesh Patidar67% (3)
- MU Prospectus 2016 RevisedDocument184 pagesMU Prospectus 2016 RevisedRico BuffetNo ratings yet
- Auricular Acupuncture Points in Weight LossDocument9 pagesAuricular Acupuncture Points in Weight LossMustafa AliNo ratings yet
- Rhabdomyolysis In-Service WuDocument24 pagesRhabdomyolysis In-Service Wuapi-323356666No ratings yet
- Assessment of Somatization and MedicallyDocument20 pagesAssessment of Somatization and MedicallyMayor AnakNo ratings yet
- Mood Disorders: Major DepressionDocument12 pagesMood Disorders: Major DepressionyammyouNo ratings yet
- A Reflection About Meaning of LifeDocument4 pagesA Reflection About Meaning of Lifeenrii orense100% (1)
- Biography DissertationDocument8 pagesBiography DissertationInstantPaperWriterSpringfield100% (1)
- Neglected Galeazzi M.Sada BaskaraDocument28 pagesNeglected Galeazzi M.Sada BaskaraDavid-ortho Novi-rehabNo ratings yet
- Doze AntibioticeDocument6 pagesDoze AntibioticeMocanu Cristina-Viorica100% (1)
- Eight BrocadesDocument8 pagesEight BrocadesMaria Aurora FoxNo ratings yet
- Nutritional MedicineDocument2 pagesNutritional MedicineVinod Kumar HonnavarNo ratings yet
- Headache MacleanDocument6 pagesHeadache MacleanJohnson100% (1)
- TB Case Finding (Slide)Document15 pagesTB Case Finding (Slide)Emman Acosta DomingcilNo ratings yet
- Effectiveness and Pharmacoeconomic Analysis of The Treatment of Severe Asthma With Omalizumab in Clinical PracticeDocument9 pagesEffectiveness and Pharmacoeconomic Analysis of The Treatment of Severe Asthma With Omalizumab in Clinical PracticePetrus Kabul TogarmaNo ratings yet
- Herbal Treatment ChildrenDocument333 pagesHerbal Treatment ChildrenMrudu Ranjan Tripathy100% (4)
- Who His HWF Amr 2018.1 EngDocument28 pagesWho His HWF Amr 2018.1 EngMaulina ManurungNo ratings yet
- Hypoglycemia UMYDocument60 pagesHypoglycemia UMYTommy AkromaNo ratings yet
- Smith Peedell (2014) Private Sector and The NHS DebateDocument3 pagesSmith Peedell (2014) Private Sector and The NHS DebateMarinaPapaNo ratings yet