You might also like
- Nursing Care Plan For CellulitisDocument6 pagesNursing Care Plan For CellulitisVilma Delos Reyes63% (16)
- Answer of Exercises-Measures of Disease FrequencyDocument7 pagesAnswer of Exercises-Measures of Disease Frequencysanjivdas100% (4)
- CDC EPR - Social Media - Preparedness 101 - Zombie Apocalypse - BlogDocument2 pagesCDC EPR - Social Media - Preparedness 101 - Zombie Apocalypse - BlogZombie Splatter Survival BlogNo ratings yet
- F BuskiDocument15 pagesF BuskiArisia No AliceNo ratings yet
- CRYPTOSPORIDIUMDocument65 pagesCRYPTOSPORIDIUMRajkishor YadavNo ratings yet
- Project IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Document38 pagesProject IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Catherine MetraNo ratings yet
- FInal Laboratory Activity Microbiology LABESORESDocument10 pagesFInal Laboratory Activity Microbiology LABESORESJAN ELMER L. LABESORESNo ratings yet
- Jordan University Study on Schistosomiasis Species and Life CycleDocument20 pagesJordan University Study on Schistosomiasis Species and Life CycleDaniel AtiehNo ratings yet
- Project IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Document36 pagesProject IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Catherine MetraNo ratings yet
- INTESTINAL NEMATODES Hand Out 10 - 11Document6 pagesINTESTINAL NEMATODES Hand Out 10 - 11microperadeniyaNo ratings yet
- Rebecca Hebner Humbio 153 Parasites and Pestilence Parasite: Schistosoma MekongiDocument32 pagesRebecca Hebner Humbio 153 Parasites and Pestilence Parasite: Schistosoma MekongiJan DielNo ratings yet
- SchistosomiasisDocument12 pagesSchistosomiasisHarold Jake ArguellesNo ratings yet
- Schistopresentation 150629172317 Lva1 App6891Document43 pagesSchistopresentation 150629172317 Lva1 App6891Briana NdayisabaNo ratings yet
- Human SchistosomiasisDocument18 pagesHuman SchistosomiasisbassbngNo ratings yet
- Cryptosporidium ParvumDocument7 pagesCryptosporidium ParvumKalebNo ratings yet
- Ascaris Lumbricoides: I. MorphologyDocument6 pagesAscaris Lumbricoides: I. MorphologyJoseline SorianoNo ratings yet
- COMMON WORM INFESTATION DrASBDocument54 pagesCOMMON WORM INFESTATION DrASBDr AMAL S BABUNo ratings yet
- Module 33 Ascariasis EditedDocument10 pagesModule 33 Ascariasis EditedPrincess Mae Sierra PacificoNo ratings yet
- MLS 702: Prevent Helminthic Infections Through Control StrategiesDocument60 pagesMLS 702: Prevent Helminthic Infections Through Control StrategiesNjeodoNo ratings yet
- Toksoplasmosis 2005 - 07Document1 pageToksoplasmosis 2005 - 07syauqyNo ratings yet
- Hookworm: Ancylostoma Duodenale and Necator AmericanusDocument18 pagesHookworm: Ancylostoma Duodenale and Necator AmericanusPutri AmandaNo ratings yet
- Zoology AscriseDocument12 pagesZoology AscrisepappunaagraajNo ratings yet
- Cryptosporidium SPDocument9 pagesCryptosporidium SPNur SafitriNo ratings yet
- ROLL NO 30 (Assignment On Zoonotic Importance of Nematodes)Document3 pagesROLL NO 30 (Assignment On Zoonotic Importance of Nematodes)barsha subediNo ratings yet
- Hymenolepis DiminutDocument10 pagesHymenolepis DiminutLois RazonNo ratings yet
- "Helminths and SanitationDocument12 pages"Helminths and SanitationSyed Ali Akbar BokhariNo ratings yet
- 417 PHL - 1st Lecture - 2021-StDocument32 pages417 PHL - 1st Lecture - 2021-StLama LNo ratings yet
- (Ancylostoma Braziliense) (Ancylostoma Caninum) (Ancylostoma Duodenale) (Necator Americanus)Document8 pages(Ancylostoma Braziliense) (Ancylostoma Caninum) (Ancylostoma Duodenale) (Necator Americanus)ŘŷØoo TЯyNo ratings yet
- ParaDocument2 pagesParabonbon_cydNo ratings yet
- Ascaris Lumbricoides: Ascariasis. Infections Most Often Seen in Young Children byDocument7 pagesAscaris Lumbricoides: Ascariasis. Infections Most Often Seen in Young Children byThea GonzalesNo ratings yet
- Parasite MCQDocument10 pagesParasite MCQbayati196459357950% (2)
- Pathophysiology Schistosomiasis: Table in New WindowDocument7 pagesPathophysiology Schistosomiasis: Table in New WindowKaren Leigh MagsinoNo ratings yet
- ASCARIASISDocument13 pagesASCARIASISSandra MichelleNo ratings yet
- F.Y.B.Sc. Sem II Practical II: Protozoan Parasites 1Document8 pagesF.Y.B.Sc. Sem II Practical II: Protozoan Parasites 1Mithun MejariNo ratings yet
- Coccidiosis in Rabbits Indian FarmingDocument13 pagesCoccidiosis in Rabbits Indian FarmingDr. K.P.JithendranNo ratings yet
- Enfermedades Por Protozoos Criptosporidiosis, Giardiasis y Otras Enfermedades Por Protozoos IntestinalesDocument18 pagesEnfermedades Por Protozoos Criptosporidiosis, Giardiasis y Otras Enfermedades Por Protozoos IntestinalesCarol VelezNo ratings yet
- NematodaDocument96 pagesNematodaPurplesmilezNo ratings yet
- Parasites of Ruminants 7Document14 pagesParasites of Ruminants 7JAD IMADNo ratings yet
- Apicomlexan: Plasmodium (Malaria)Document31 pagesApicomlexan: Plasmodium (Malaria)hanan mziryNo ratings yet
- Ascaris Lumbricoides Diagnostic and Infective Life CycleDocument17 pagesAscaris Lumbricoides Diagnostic and Infective Life CycleRaymundo III DoceNo ratings yet
- Ascaris lumbricoides Literature ReviewDocument10 pagesAscaris lumbricoides Literature ReviewDina Fitri FauziahNo ratings yet
- D Latum NotesDocument3 pagesD Latum NotesSalsabila Putri AmrilNo ratings yet
- PBL - Tropis: MalariaDocument11 pagesPBL - Tropis: MalariaArifin Ayob0% (1)
- Apicomplexa (Sporozoa) 5.1general Future and ClassificationDocument10 pagesApicomplexa (Sporozoa) 5.1general Future and Classificationtedela gulumaNo ratings yet
- Tropical Medicine Lecture Edited-1Document96 pagesTropical Medicine Lecture Edited-1inspiredwriter617No ratings yet
- CryptosporidiosisDocument46 pagesCryptosporidiosisruthNo ratings yet
- Parasitology - Trematodes - Intestinal & Liver FlukesDocument76 pagesParasitology - Trematodes - Intestinal & Liver FlukesNicole ManogNo ratings yet
- Myxidium SalveliniDocument4 pagesMyxidium Salvelinimigas1996No ratings yet
- Medical Biology 6Document58 pagesMedical Biology 6Yusuf Yağız TimurNo ratings yet
- Schistosomes: Diecious TrematodesDocument6 pagesSchistosomes: Diecious TrematodesShivanshi KNo ratings yet
- Other Trematodes (Intestinal, Liver and Pancreatic Flukes) : Fasciolopsis BuskiDocument5 pagesOther Trematodes (Intestinal, Liver and Pancreatic Flukes) : Fasciolopsis BuskiChristine BuenNo ratings yet
- Bilharzia in the Philippines: past, present and future control strategiesDocument5 pagesBilharzia in the Philippines: past, present and future control strategiesVincent ReyesNo ratings yet
- CoccidiosisDocument6 pagesCoccidiosisAnaNo ratings yet
- Salmonellosisincluding Entericfever: Farah Naz Qamar,, Wajid Hussain,, Sonia QureshiDocument13 pagesSalmonellosisincluding Entericfever: Farah Naz Qamar,, Wajid Hussain,, Sonia QureshiAnak MuadzNo ratings yet
- Cattle Meat Inspection Chapter 2Document35 pagesCattle Meat Inspection Chapter 2hadiminshawi2029No ratings yet
- The Topics Include Definition, The Pathogen, Epidemiology, Etiology and Life Cycle, Pathobiology, Clinical Manifestations, Diagnosis and TreatmentDocument48 pagesThe Topics Include Definition, The Pathogen, Epidemiology, Etiology and Life Cycle, Pathobiology, Clinical Manifestations, Diagnosis and TreatmentAnonymous yE9u7tVQo9No ratings yet
- Faculty of Health Sciences: DepartmentDocument35 pagesFaculty of Health Sciences: DepartmentAbdirashiid Mahdi HirsiNo ratings yet
- Malaria: Etiology and PathogenesisDocument8 pagesMalaria: Etiology and PathogenesissabilafaNo ratings yet
- Revision: Types of Life Cycle in Trematoda and CestodaDocument71 pagesRevision: Types of Life Cycle in Trematoda and CestodaMicroscopeGeekNo ratings yet
- Aljas&Bama (Microbm9evaluate)Document8 pagesAljas&Bama (Microbm9evaluate)Mary Clare Fuentes BamaNo ratings yet
- Angio Strong Yl UsDocument29 pagesAngio Strong Yl UsIndra MahaputraNo ratings yet
- Cats and Toxoplasma: A Comprehensive Guide to Feline ToxoplasmosisFrom EverandCats and Toxoplasma: A Comprehensive Guide to Feline ToxoplasmosisNo ratings yet
- Filariasis: Causes, Tests, and Treatment OptionsFrom EverandFilariasis: Causes, Tests, and Treatment OptionsRating: 5 out of 5 stars5/5 (2)
- DecalcificationDocument7 pagesDecalcificationPau SorianoNo ratings yet
- Donor BloodDocument2 pagesDonor BloodPau SorianoNo ratings yet
- Biological Safety CabinetDocument9 pagesBiological Safety CabinetPau SorianoNo ratings yet
- Specimen Collection, Processing & Chain of Custody GuideDocument4 pagesSpecimen Collection, Processing & Chain of Custody GuidePau SorianoNo ratings yet
- Chapter 1Document30 pagesChapter 1Pau SorianoNo ratings yet
- Differentiating Staphylococcus and Micrococcus with BacitracinDocument13 pagesDifferentiating Staphylococcus and Micrococcus with BacitracinPau SorianoNo ratings yet
- Major OrgansDocument20 pagesMajor OrgansPau SorianoNo ratings yet
- We Need To Be Fit To Fight The VirusDocument2 pagesWe Need To Be Fit To Fight The VirusPau SorianoNo ratings yet
- MYCOVIRODocument11 pagesMYCOVIROPau SorianoNo ratings yet
- TLE Menu Performance TaskDocument23 pagesTLE Menu Performance TaskPau SorianoNo ratings yet
- Hepatic FlukesDocument3 pagesHepatic FlukesPaul Avila SorianoNo ratings yet
- Identification of Bacteria (40Document11 pagesIdentification of Bacteria (40Pau SorianoNo ratings yet
- Bernabe Q Biagtan Elementary School property reportDocument19 pagesBernabe Q Biagtan Elementary School property reportPau SorianoNo ratings yet
- How Can We Live A World Like ThisDocument2 pagesHow Can We Live A World Like ThisPau SorianoNo ratings yet
- AttendanceDocument1 pageAttendancePau SorianoNo ratings yet
- National Training Service Program (NSTP) : Don Mariano Marcos Memorial State University La Union, PhilippinesDocument24 pagesNational Training Service Program (NSTP) : Don Mariano Marcos Memorial State University La Union, PhilippinesPau SorianoNo ratings yet
- Acid-base disorders summaryDocument6 pagesAcid-base disorders summaryPau SorianoNo ratings yet
- Sample: Practicum PortfolioDocument21 pagesSample: Practicum PortfolioPau SorianoNo ratings yet
- Acid-base disorders summaryDocument6 pagesAcid-base disorders summaryPau SorianoNo ratings yet
- A Message From 2080Document1 pageA Message From 2080Pau SorianoNo ratings yet
- Effects of Virtual Learning Among Medical Laboratory Science Students in Their Academic PerformancesDocument13 pagesEffects of Virtual Learning Among Medical Laboratory Science Students in Their Academic PerformancesPau SorianoNo ratings yet
- Instrumentati ON Lesson: Group 6Document39 pagesInstrumentati ON Lesson: Group 6Pau SorianoNo ratings yet
- NSTP 1 MODULE 2 Drug EducationDocument12 pagesNSTP 1 MODULE 2 Drug EducationPau SorianoNo ratings yet
- Report 1Document12 pagesReport 1Pau SorianoNo ratings yet
- STS Module 1 Lesson 1-2Document38 pagesSTS Module 1 Lesson 1-2Pau SorianoNo ratings yet
- STS Module 1 Lesson 1-2Document38 pagesSTS Module 1 Lesson 1-2Pau SorianoNo ratings yet
- A Warning From 2080Document2 pagesA Warning From 2080Pau SorianoNo ratings yet
- Thyroid-CC Group6Document35 pagesThyroid-CC Group6Pau SorianoNo ratings yet
- Explore the heritage and culture of Calasiao, Pangasinan through its people, churches, and foodDocument5 pagesExplore the heritage and culture of Calasiao, Pangasinan through its people, churches, and foodPau SorianoNo ratings yet
- PNEUMONIADocument24 pagesPNEUMONIAwheeyycoldandhot55No ratings yet
- Upaya Kesehatan Masyarakat Esensial Pencegahan - Pengendalian PenyakitDocument56 pagesUpaya Kesehatan Masyarakat Esensial Pencegahan - Pengendalian PenyakitGiselleNo ratings yet
- 5.1.7 Anaemia in Pregnancy - MauwaDocument17 pages5.1.7 Anaemia in Pregnancy - MauwaSetlhare MotsamaiNo ratings yet
- Acute Bronchitis Symptoms Causes TreatmentDocument5 pagesAcute Bronchitis Symptoms Causes TreatmentDianne LegionNo ratings yet
- 09 Science Notes ch13 Why Do We Fall Ill PDFDocument3 pages09 Science Notes ch13 Why Do We Fall Ill PDFthiruNo ratings yet
- Oswego E 2012 PDFDocument14 pagesOswego E 2012 PDFA SeulNo ratings yet
- Species Affected: Bluetongue (BTV)Document3 pagesSpecies Affected: Bluetongue (BTV)Andrei CiobanuNo ratings yet
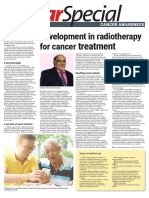
- Cancer Awareness - 4 February 2023Document6 pagesCancer Awareness - 4 February 2023Times MediaNo ratings yet
- Causes and Risk Factors of Stis: Sexually Transmitted Diseases GuideDocument12 pagesCauses and Risk Factors of Stis: Sexually Transmitted Diseases GuideCabiomilaNo ratings yet
- Relative Resource Manager 2 TestDocument4 pagesRelative Resource Manager 2 Testmezuniga1No ratings yet
- Syllabus EPHDocument44 pagesSyllabus EPHSujitNo ratings yet
- Warta Kerajaan Persekutuan: Federal Government GazetteDocument3 pagesWarta Kerajaan Persekutuan: Federal Government GazetteAswadi MohamadNo ratings yet
- Concept Map RSVDocument1 pageConcept Map RSVNoemi GabayNo ratings yet
- MCQ 2019 Part 1 UseDocument94 pagesMCQ 2019 Part 1 UseWanny WattakavanichNo ratings yet
- Colitis IndeterminadaDocument6 pagesColitis IndeterminadaMaria FannyNo ratings yet
- Bantay ASF Sa BarangayDocument18 pagesBantay ASF Sa BarangayJoeboyTiuNo ratings yet
- The Newcastle-Ottawa Scale (NOS) For Assessing The Quality of Nonrandomized Studies in Meta-AnalysisDocument39 pagesThe Newcastle-Ottawa Scale (NOS) For Assessing The Quality of Nonrandomized Studies in Meta-AnalysisFouadYoussefNo ratings yet
- SP ACCURE InjectablesDocument8 pagesSP ACCURE Injectablessanjay_gawaliNo ratings yet
- Utilities of CEA and CA19-9 As Markers in Colorectal CancerDocument6 pagesUtilities of CEA and CA19-9 As Markers in Colorectal CancerIJCRM Research JournalNo ratings yet
- Italy Travel Declaration FormDocument1 pageItaly Travel Declaration FormMarius NenciuNo ratings yet
- Abstract Book of The XXII Congresso Nazionale DellDocument211 pagesAbstract Book of The XXII Congresso Nazionale DellMuh ParditunasNo ratings yet
- PANDAS Fact Sheet: Understanding Pediatric Autoimmune Neuropsychiatric DisordersDocument11 pagesPANDAS Fact Sheet: Understanding Pediatric Autoimmune Neuropsychiatric Disordersgun gorNo ratings yet
- Pediatric Case 6: Eva Madison (Complex) : Guided Reflection QuestionsDocument3 pagesPediatric Case 6: Eva Madison (Complex) : Guided Reflection QuestionsKathy ArenasNo ratings yet
- Patofisiologi Kanker RahimDocument98 pagesPatofisiologi Kanker RahimOjo Nesu100% (1)
- Public Health-Relevant Consequences of The COVID-19 Pandemic On Malaria in Sub-Saharan Africa: A Scoping ReviewDocument16 pagesPublic Health-Relevant Consequences of The COVID-19 Pandemic On Malaria in Sub-Saharan Africa: A Scoping ReviewM Franck MakongaNo ratings yet
- Guillain Barre SyndromeDocument32 pagesGuillain Barre SyndromeDada MundaNo ratings yet